Chronic fatigue syndrome in adolescents. Beyond tiredness

Chronic fatigue syndrome (CFS) in adolescents can have significant physical, social and psychological impacts. A comprehensive history and assessment and exclusion of other fatigue-causing conditions are crucial to timely diagnosis. An individualised multidisciplinary rehabilitative approach to adolescents with CFS is key to management.
Chronic fatigue syndrome (CFS) in adolescents is a condition primarily characterised by severe, persistent, unexplained fatigue.1 In CFS, the fatigue is exacerbated by exertion (postexertional malaise) and may be accompanied by other symptoms including musculoskeletal pain, cognitive ‘brain fog’, unrefreshing or disturbed sleep, and neurological and autonomic symptoms such as headache and dizziness on standing or exertion consistent with orthostatic intolerance.2 There are many proposed hypotheses for the aetiology of CFS including infectious agents, immune dysfunction, autoimmune disorders, genetic susceptibility or abnormality, neuroendocrine disorders, circulatory abnormalities, toxins, metabolic disturbances, or a combination of these.2,3 The estimated national incidence of paediatrician-diagnosed cases of CFS in adolescents aged 10 to 17 years in Australia is 6.38 per 100,000 per year.1 Adolescence has been identified as one of two age peaks in incidence of CFS in a Norwegian-based population registry study.4 Diagnostic criteria are based on commonly used case definitions for the diagnosis of CFS/myalgic encephalomyelitis (ME) in children and adolescents and are discussed in detail below.5-7
CFS in adolescents is frequently triggered by a viral or infective illness, with about two-thirds of paediatric patients identified as having a presumed viral or infective trigger for symptom onset.1 In addition to severe fatigue, adolescents with CFS may present to their general practitioner with nonspecific symptoms, including frequent sore throats, headaches or pain, or because of concerns regarding decreased level of functioning, school attendance, decreased engagement with their regular activities or with friends.2
CFS in adolescents typically occurs during middle to late adolescence, during a critical period of social, emotional and physical development.8 Disruption during this key stage of development can be associated with significant functional impairment, such as decreased school attendance, impaired social participation and emergence of comorbid mental health conditions including depression and anxiety, as well as long-term health, social, emotional and vocational implications.2,8 There is often a protracted period of time between symptom onset and the diagnosis being made, with 52% of children or adolescents diagnosed 13 months after symptom onset.1 Timely diagnosis is important to ensure appropriate medical care and management and to minimise the long-term morbidity of CFS.9
Adolescents have a relatively good prognosis compared with adults with CFS. Adolescents engaged in multidisciplinary rehabilitative treatment have shown significant improvements in parent-reported adolescent physical and psychosocial functioning over time.10 Of those seen in a specialised Australian adolescent CFS service, 50% reported recovery from CFS, with 38% recovering within five years and 68% within 10 years.11 All improved functionally, with only 5% reporting remaining very unwell.11 Supportive professionals who made or understood the diagnosis were highly valued by young people with CFS, highlighting the importance of accurate diagnosis and therapy.12
Assessment and diagnosis
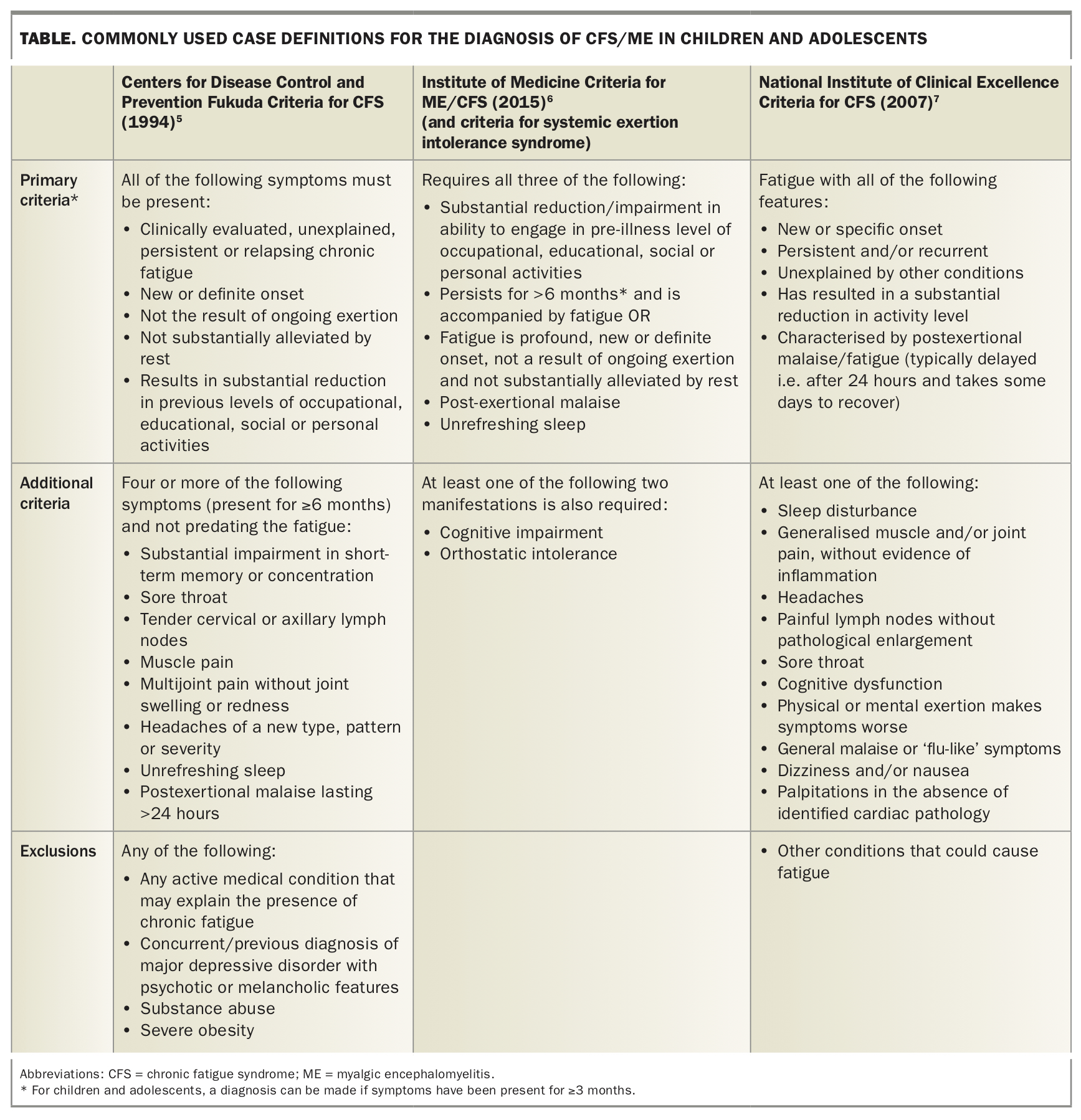
Since it was first described by Holmes in 1988,13 the terminology surrounding CFS has often been confusing, with various clinical criteria and case definitions described. Commonly used terminology includes myalgic encephalomyelitis (ME) and the umbrella term of CFS/ME.6 The diagnosis of CFS/ME is a clinical diagnosis, based on thorough history, recognition of the pattern of symptoms and exclusion of other conditions causing fatigue, through comprehensive history-taking, physical examination and appropriate medical investigations.2 Diagnosis is based on the young person fulfilling diagnostic criteria. A number of varied clinical criteria are currently used to diagnose CFS in children and adolescents, including the 1994 Fukuda case definition for CFS/ME adopted by the Centers for Disease Control and Prevention, the 2015 Institute of Medicine Diagnostic Criteria for Children and Adults, and the 2006 Canadian Paediatric Clinical Case Definition for CFS/ME, which is best used for research purposes.5,6,14 The Fukuda criteria remain the most commonly cited case definition for CFS;15 however, this definition was predominantly designed for use in adults. More recently formulated case definitions were designed for children and adolescents.6,8,14,16 Commonly used case definitions/clinical criteria are outlined in the Table.
{kind=link}
Common across these criteria are the presence of the following three core features:
- postexertional malaise (following cognitive or physical exertion)
- unrefreshing sleep
- significant fatigue that is severe, of new onset and not substantially alleviated by rest, with reduction of function compared with before illness.
Other core features seen in adolescents include cognitive impairment and autonomic dysfunction/orthostatic intolerance.2,6,7 Importantly, the case definition requirement for CFS is typically a duration of illness of more than three months for adolescents compared with more than six months for adults.7
Assessment should also include the identification of predisposing factors, such as genetic factors, family history and joint hypermobility, as well as complicating factors such as orthostatic intolerance, sleep disturbance, and anxiety and mood disorders, as outlined below.2
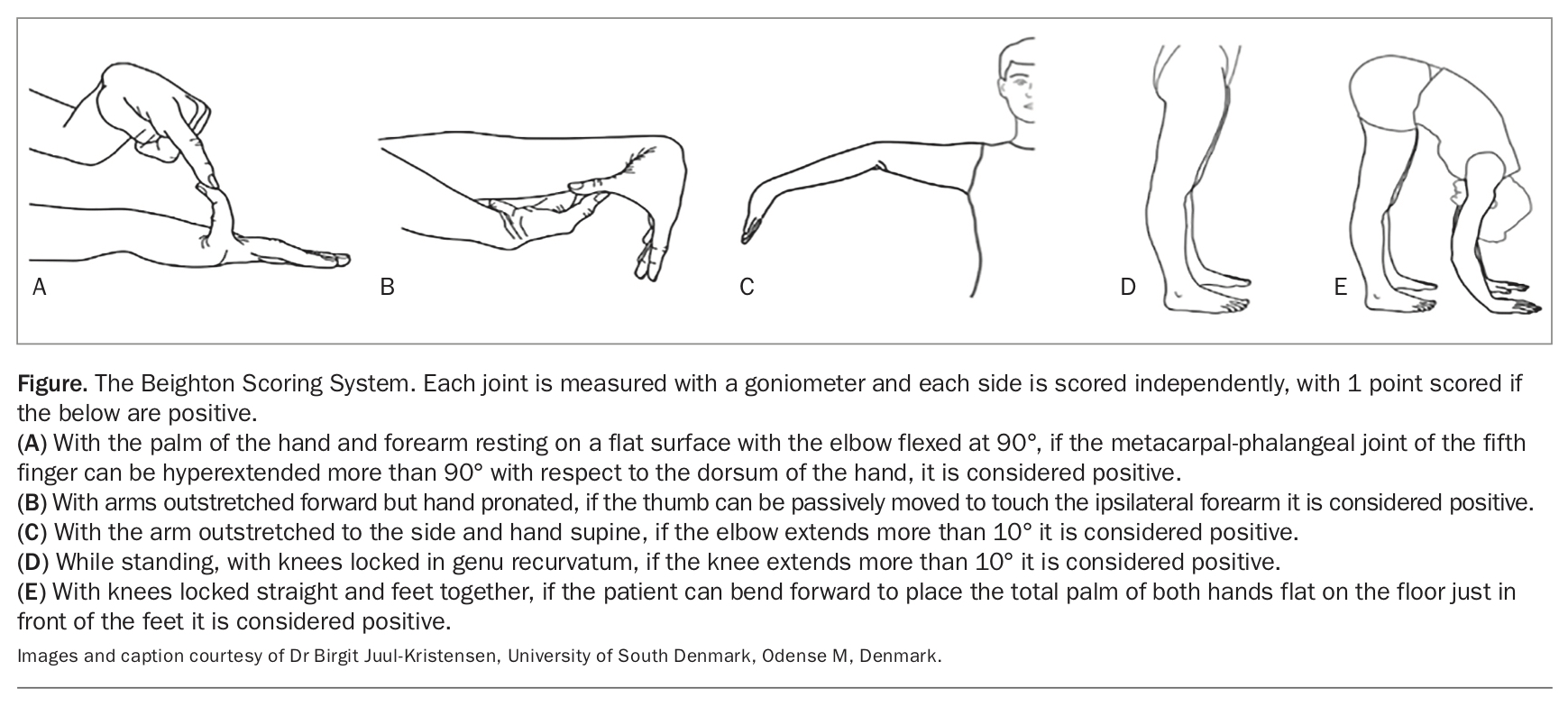
Physical signs in CFS are subtle and are not diagnostic.2 Physical examination should include growth parameters and pubertal staging, an orthostatic standing test to assess for orthostatic intolerance, Beighton score to assess joint hypermobility (Figure) and musculoskeletal signs.2 There is no current valid, reliable laboratory test for diagnosing CFS, and baseline blood tests are usually normal. Recommended initial investigations according to main symptomatology are outlined in the Box.7
{kind=link}
{kind=link}
UK guidelines on CFS/ME diagnosis and management recommend that children and adolescents presenting with a history suggestive of CFS be referred to a paediatrician within six weeks of assessment and have the diagnosis confirmed by a paediatrician.7 For children or young people with significant functional impairment associated with fatigue, referral to a paediatrician or adolescent physician should not be delayed.
Assessment and management of complications and comorbidities
A number of conditions commonly associated with CFS in children and adolescents can predispose to and exacerbate the fatigue, most notably postural orthostatic tachycardia syndrome (POTS) and clinical joint hypermobility. Functional gastrointestinal disorders, chronic persistent widespread pain, headaches, sleep disturbance, depression and anxiety are also frequently reported.1
Orthostatic intolerance/postural orthostatic tachycardia syndrome (POTS)
Orthostatic intolerance refers to symptoms that worsen with upright posture and improve with lying down.2,17 Symptoms of orthostatic intolerance include lightheadedness or dizziness, whiteout or blackout of visual fields, blurred vision, headaches, nausea and increased fatigue. Signs on physical examination include acrocyanosis or mottling of the dependent limbs and facial pallor with standing for more than a few minutes.2 The most common syndromes of orthostatic intolerance are POTS, neurally mediated hypotension and orthostatic hypotension, the latter two being less frequent in the paediatric/adolescent population.2
POTS is a form of autonomic dysfunction, characterised by orthostatic intolerance, excessive postural tachycardia and fatigue.18 It is the most common comorbid condition in paediatric CFS and is present in 26.2% of paediatric patients diagnosed with CFS in Australia.1 Therefore, accurate identification and management of POTS is important as part of management of CFS in children and adolescents.
To diagnose POTS, a 10-minute orthostatic standing test should be undertaken as follows: with the adolescent resting supine for at least 5 minutes, record a baseline heart rate and blood pressure when supine; then ask them to stand while you measure heart rate and blood pressure every minute for 10 minutes. The diagnosis of POTS requires the presence of orthostatic signs and/or symptoms (such as lightheadedness, dizziness, syncope, visual disturbance, nausea, headache, palpitations), as well as an increase in heart rate of 40 bpm or more when going from supine to upright posture, and a heart rate sustained at over 120 bpm.2,18,19 The co-occurrence of POTS and fatigue needs to be identified in order for concurrent management of POTS and CFS and to prevent increased functional impairment. POTS is often associated with joint hypermobility, functional gastrointestinal disorders, sleep disturbance and mood disorders, which can complicate CFS.19 Undiagnosed POTS is associated with significant social and emotional consequences, including decreased function, school attendance and engagement with extracurricular activities, multiple health care visits, increased carer burden and missed work for parents.18
Management of POTS includes nonpharmacological strategies of increasing fluid and salt intake to maintain intravascular volume, use of compression stockings when standing, incorporation of aerobic and strengthening exercises and re-engagement with academic activity in a graded fashion.18 Pharmacological interventions should be targeted at improving the dominant symptoms that do not respond to conservative measures. Pharmacological interventions for orthostatic intolerance/POTS include: medications that increase blood volume such as fludrocortisone and the combined oral contraceptive pill; sympathetic tone modifiers such as propranolol, clonidine and vasoconstricting agents (e.g. midodrine); and selective serotonin reuptake inhibitors such as fluoxetine or sertraline, which have the added benefit of treating concurrent depression or anxiety.2
Joint hypermobility
Joint hypermobility is commonly associated with CFS and 60% of young patients who meet the criteria for CFS/ME also have joint hypermobility (compared with 20% of healthy adolescents).2 An Australian cohort of paediatrician-diagnosed cases of CFS found that 13% had associated joint hypermobility.1
Adolescents presenting with symptoms suggestive of CFS should be assessed for generalised joint hypermobility (GJH). If GJH is present, screening for Ehlers-Danlos syndrome (EDS), particularly hypermobile EDS (hEDS), should be undertaken, as a subset of individuals with CFS may have hEDS as the underlying aetiology.20 Diagnosing joint hypermobility is important, as the condition can add to the burden of illness in CFS/ME and requires different approaches in physical therapy.2
Joint hypermobility is best assessed through the use of the Beighton Score during physical examination (Figure). A score of 5 or greater in adolescents is indicative of GJH. If joint hypermobility is present, history and examination looking for signs of hEDS (using the detailed diagnostic criteria for EDS subtypes outlined in the 2017 international classification of the Ehlers-Danlos Syndromes21) should be undertaken to ensure that appropriate management is recommended. The recommended management for joint hypermobility is physical strengthening, stabilising joints with maintenance of healthy muscle and reconditioning to prevent injury and musculoskeletal pain, in conjunction with pain management and psychological strategies to prevent distress.22
Sleep disturbance
Adolescents commonly present to primary care providers with nonspecific symptoms of tiredness and fatigue. Screening questions for sleep difficulties in adolescents should be included in the initial work-up of a fatigued adolescent. Sleep disorders including delayed sleep phase disorder, obstructive sleep apnoea, narcolepsy, idiopathic hypersomnolence and periodic leg movement in sleep need to be excluded or treated appropriately.23,24 Consider referral to a sleep specialist and formal polysomnography if there are concerns regarding diagnosis or ongoing issues with sleep with significant impact on function despite instituting adequate sleep hygiene methods.24
Adolescents with CFS experience unrefreshing sleep and sleep disturbances.2 They have been identified as having significantly longer sleep onset latency, time in bed and total sleep time, later rise time and significantly poorer subjective sleep quality compared with healthy adolescents.25 There may also be frequent wakenings, day-night reversal and difficulty staying asleep.2 Education around sleep hygiene is important, in particular avoiding or minimising daytime sleep, while still balancing daytime activity with restful activities to avoid symptom exacerbation from overexertion. If refractory symptoms occur after sleep hygiene strategies are in place, the addition of melatonin can be helpful.2,7
Mental health conditions
Depression and anxiety are common in adolescents with CFS and may be secondary to the impact of CFS on the young person’s life (i.e. reactive); however, we often do not know which came first.26 A UK study evaluating adolescents who were referred to a specialist CFS unit using structured psychiatric interview found that 38% met the criteria for major depressive disorder, 28% met the criteria for an anxiety disorder and 15% had coexisting anxiety and depression.27 Australian studies of paediatric CFS diagnosed by paediatricians reported comorbid anxiety and depression in 26% and 13% of cases, respectively.1 It is important that anxiety, depression and mood disorder are assessed in all adolescents with CFS and appropriate treatment is initiated.7,27,28
Somatisation can also complicate the management of CFS. Studies have shown that adolescents with CFS have more somatic complaints than comparison groups of adolescents with other chronic illnesses, and higher somatisation scores on the Children’s Somatization Inventory than adolescents with migraine or healthy controls.29 Somatisation can reinforce illness behaviour and influence illness attribution and needs to be considered in the management of CFS.
Educational impact
Adolescents with CFS have significantly higher rates of school absenteeism, decreased participation, poorer quality of life in the school setting, decreased school connectedness and lower academic performance than healthy adolescents.30 The high rate of school absenteeism is exacerbated by delays in diagnosis and appropriate management. The average amount of time away from school for students with CFS has been estimated as one year across their school life.31 Young people with CFS often want to attend school but are prevented from doing so by physical limitations or fear of symptom exacerbation.2 School refusal is often hard to differentiate from inability to attend school due to symptoms, indicating the importance of a thorough psychosocial assessment. Maintaining engagement in an education system that is flexible and can accommodate the illness and aspirations of adolescents with CFS has been reported as crucial to long-term functioning.11 Therefore, providing good communication with the school and advocating for the young person to receive flexibility and support at school is essential. This usually involves collaborative decision making between healthcare services, education providers, and the young person and their family around educational options.
Approach to management
The management of children and adolescents with CFS requires an individualised multidisciplinary rehabilitative approach that addresses the biopsychosocial needs of the young person and their family.32 Recent studies and current clinical practice guidelines recommend that comprehensive management includes:2,10,29,33,34
- education and a clear explanation around the condition and complications
- optimising management (pharmacological and nonpharmacological) of troublesome symptoms
- reinforcing sleep regulation
- identifying and managing comorbidities
- encouraging maintenance of social contact and some enjoyable activities
- supporting engagement in education with regular verbal and written school liaison and advocacy.
Individual psychological assessment to elucidate the adolescent’s perceptions of their illness and any associated psychological comorbidities, in conjunction with family assessment and support, are important components of CFS management in adolescents.
Referral to a psychologist can be framed as an important step in supporting the adolescent to learn how to manage their illness and the often unavoidable and understandable impact it has on their lives and sense of self. Psychological assessment guides the use of a cognitive behavioural therapy framework, which is an evidence-based intervention for CFS that aims to identify and modify unhelpful beliefs and behaviours that may interfere with the adolescent’s capacity to actively manage their illness and to increase their understanding of the interaction of biopsychosocial factors in managing symptoms, with the goal to improve level of function and reduce symptom severity.32,33 Other therapeutic approaches may also be beneficial, with emerging evidence that mindfulness strategies can help to reduce anxiety and stress in adolescents with CFS.35 Cardiopulmonary exercise testing and consultation with a skilled exercise physiologist can be helpful to guide activity pacing, supported by cognitive behavioural therapy and regular review of progress.2,3,30,36
Most adolescents with CFS can be managed within an ambulatory outpatient setting;2,7 however, adolescents with severe functional impairment are likely to require an inpatient multidisciplinary rehabilitation admission, with a specialised adolescent medicine or chronic fatigue service for further assessment, to manage contributing factors or complications and to allow a more intensive approach to improve level of function and return to school. Ongoing multidisciplinary follow up and educational support as an outpatient can maintain the gains made from an inpatient stay.
Conclusion
CFS in adolescence can be associated with significant functional impairment, as well as medical and psychological comorbidities. However, the prognosis for adolescents with CFS is promising, with recovery expected. General practitioners are essential in identifying children and adolescents with a history suggestive of CFS, undertaking initial assessment and management, providing ongoing support, monitoring progress and ensuring timely referral to a paediatrician or adolescent physician and allied health professionals in order to facilitate optimal outcomes (see Practice points on CFS). MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.