Diffuse linear streaks on the trunk and limbs

Test your diagnostic skills in our regular dermatology quiz. What has caused this rash of maculopapular linear streaks?
Case presentation
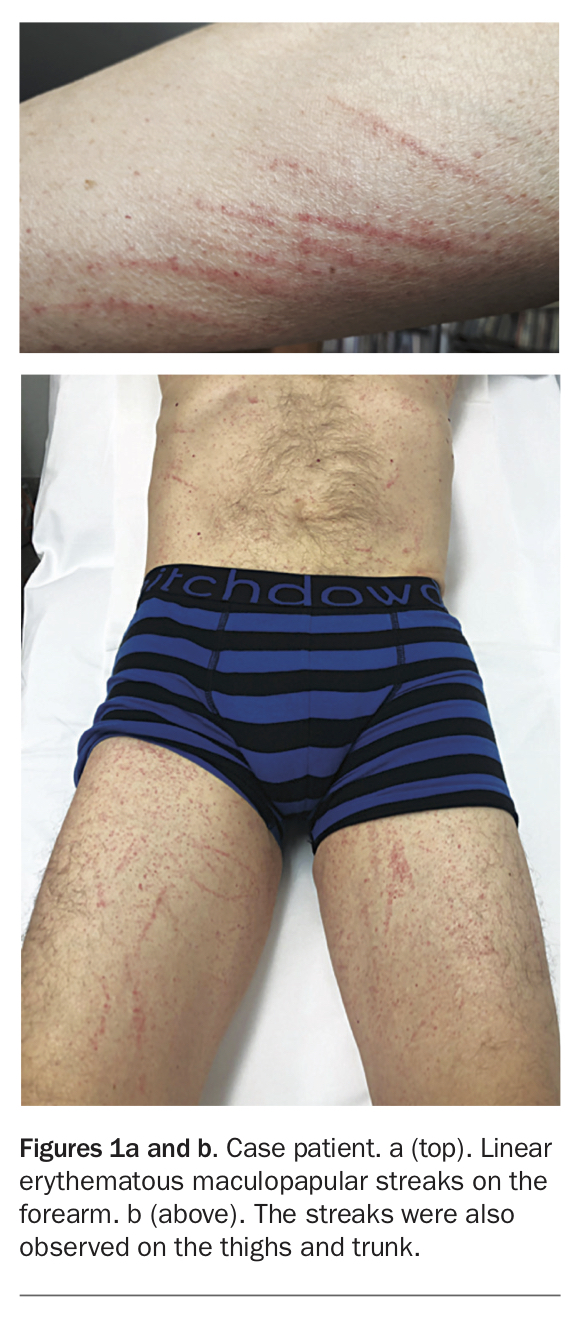
A 65-year-old man presents with a two-day history of a mildly itchy rash (Figures 1a and b). He has been otherwise well and denies any fevers, night sweats or unintentional weight loss. The patient does not have any other medical issues or take regular medications. He has not recently travelled or started any new medications.
{kind=link}
On examination, there is a symmetrical maculopapular rash involving the patient’s trunk and his upper and lower limbs. The macules and papules are erythematous and have a distinct linear ‘flagellate’ appearance.
Differential diagnoses
The morphology of the eruption is consistent with a flagellate dermatosis. The term flagellate describes a distribution that is patterned in linear streaks, as though the patient has been whipped. Flagellate rashes are often erythematous at first, evolving to become pigmented with time, and are rare. There are several known causes, some of which are serious. Conditions to consider among the differential diagnoses include the following.
- Bleomycin toxicity. Bleomycin, which is derived from Streptomyces verticillus, has antineoplastic and antibiotic properties and is used to treat Hodgkin’s lymphoma and germ cell tumours.1 Bleomycin hinders the incorporation of thymidine into DNA and is inactivated by bleomycin hydrolase in most
organs – except for the lungs and the skin, where this enzyme is absent.2 Thus, bleomycin toxicity is usually observed in the lungs, causing pulmonary fibrosis, and the skin, causing multiple mucocutaneous reactions such as flagellate dermatitis.1,2 Bleomycin-induced flagellate dermatitis presents with linear, hyperpigmented and erythematous pruritic flagellate streaks on the trunk, which can appear within one day and up to nine weeks following bleomycin administration.1 The pathogenesis of bleomycin-induced flagellate dermatitis is not known and can occur with a total dose as low as 15 mg.2 Biopsy features are nonspecific and include spongiosis, perivascular eosinophilia, acantholysis, basal vacuolisation, dyskeratosis and melanin incontinence.1,2 - Adult-onset Still’s disease (AOSD). This systemic idiopathic inflammatory disease presents with arthralgia and has a characteristic salmon-pink maculopapular erythematous eruption involving the upper and lower limbs that coincides with fever.3 AOSD requires prompt attention because the complications include aseptic pericarditis, pleuritis and haemophagocytic lymphohistiocytosis.3 Despite being the most commonly observed cutaneous manifestation of AOSD, the classic salmon-pink rash is only one of many morphologies. An atypical presentation is linear erythematous and hyperpigmented flagellate streaks of papules and plaques that may bear surface crusting and involve the trunk and limbs.3 Biopsy of these flagellate lesions shows hyperkeratosis, scattered neutrophilic dermal infiltrate, dermal mucin and dyskeratosis.3
- Dermatomyositis (DM). This inflammatory condition presents with progressive symmetrical myopathy that usually involves proximal muscles and skin.4 Pathognomonic cutaneous changes include hyperkeratotic violaceous papules and plaques on the extensor surfaces of the upper and lower limbs (Gottron’s papules) and a periorbital violaceous, maculopapular rash involving the eyelids (heliotrope rash).4 An uncommon morphological manifestation of DM is a pruritic, flagellate erythema consisting of linear, violaceous streaks that mainly involve the truncal skin.5 This type of flagellate erythema is associated with idiopathic DM, and has not been reported in paraneoplastic, juvenile or amyopathic DM.5 Skin biopsy features of DM are nonspecific and often difficult to distinguish from systemic lupus erythematosus; histopathological changes include perivascular inflammation, increased deposition of dermal mucin, telangiectasias and vacuolar change at the dermoepidermal junction.6
- Shiitake mushroom dermatitis. This is the correct diagnosis. First described in 1977, the consumption of shiitake mushrooms (Lentinula edodes) can cause a characteristic flagellate dermatosis.7,8 It presents with pruritic, linear streaks of erythematous papules and vesicles commonly affecting the trunk, limbs and posterior neck within one to three days of consuming the mushrooms.8,9 When the case patient was questioned about his diet, he described eating shiitake mushrooms two days prior to the onset of the rash. The aetiology is thought to stem from the thermolabile polysaccharide toxin lentinan, a known immunomodulator capable of inducing interleukin-1 release and vasodilatation. However, despite initial reports relating to inadequately cooked shiitake mushrooms, flagellate dermatitis also occurs in patients who have consumed thoroughly cooked shiitake mushrooms.9 The mechanism by which lentinan results in a flagellate dermatitis is unknown. The histopathological features of shiitake mushroom dermatitis are nonspecific and include spongiosis, a focal lymphocytic interface reaction and a perivascular lymphocytic infiltrate.9
Diagnosis
In this patient, the diagnosis of shiitake mushroom dermatitis was made from a combination of a clinical history confirming shiitake mushroom consumption and a physical examination demonstrating the typical skin reaction. The absence of a history of medication use and hyperpigmentation excluded bleomycin-induced flagellate dermatitis. A full blood count showed normal white cell count and neutrophils, while a C-reactive protein level was within normal limits. The lack of constitutional symptoms concerning for DM (muscle weakness, photosensitive rash) or AOSD (fever, night sweats, arthralgia) made a systemic inflammatory process less likely. Skin biopsies were performed, which showed a patchy mild interface reaction with patchy vacuolar change and a perivascular lymphocytic infiltrate in the superficial dermis, consistent with shiitake mushroom dermatitis. Immunofluorescence testing returned negative results for IgA, IgG, IgM, C3 and fibrinogen.
Management and outcome
The patient was reassured that the rash was not indicative of a sinister process and he was advised not to consume shiitake mushrooms again. His pruritus resolved with regular application of topical betamethasone dipropionate 0.05% ointment and moisturiser with oral antihistamines as required. He was reviewed two weeks later and his rash had resolved. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.