Common skin problems in children. Birthmarks

Skin conditions
Although most birthmarks are small and harmless, some are large and can cause cosmetic or functional impairment. Others can indicate an underlying abnormality, and a few have malignant potential. Some birthmarks can be removed, but others remain a challenge to treat even with present surgical and laser techniques.
- ‘Birthmark’ is a lay term that encompasses many skin conditions, including malformations, neoplasms and hamartomas; not all are obvious at birth.
- The risk of melanoma in children is low; most melanocytic naevi are removed for cosmetic reasons, not malignancy.
- Naevus sebaceous is the most common epidermal naevus and one of the few with a malignant potential.
- Most haemangiomas are uncomplicated, requiring no intervention; however, facial haemangiomas need to be carefully observed over time as even a modest increase in size can cause substantial problems.
- The ‘gold standard’ treatment for haemangiomas that are large, ulcerated, likely to cause deformity or affecting an orifice is oral propranolol.
- Children with capillary malformations (port wine stains) may be treated with pulsed dye laser therapy and should be referred for assessment as early as possible.
- Most small birthmarks can be removed; however, the decision should be postponed in most cases until the child can be involved in decision making.
To the layperson, the term ‘birthmark’ indicates a permanent skin lesion that a child is born with. However, not all congenital lesions are permanent, and not all permanent lesions are present at birth. From a medical viewpoint, birthmarks encompass a wide variety of cutaneous lesions, including malformations, neoplasms and hamartomas. The cells of these lesions include melanocytes, vascular elements, keratinocytes and skin appendages such as sebaceous glands, all of which occur normally in the skin.
This article reviews the most common types of birthmarks occurring in childhood and their presentation and management.
Pigmented naevi
Melanocytic naevi
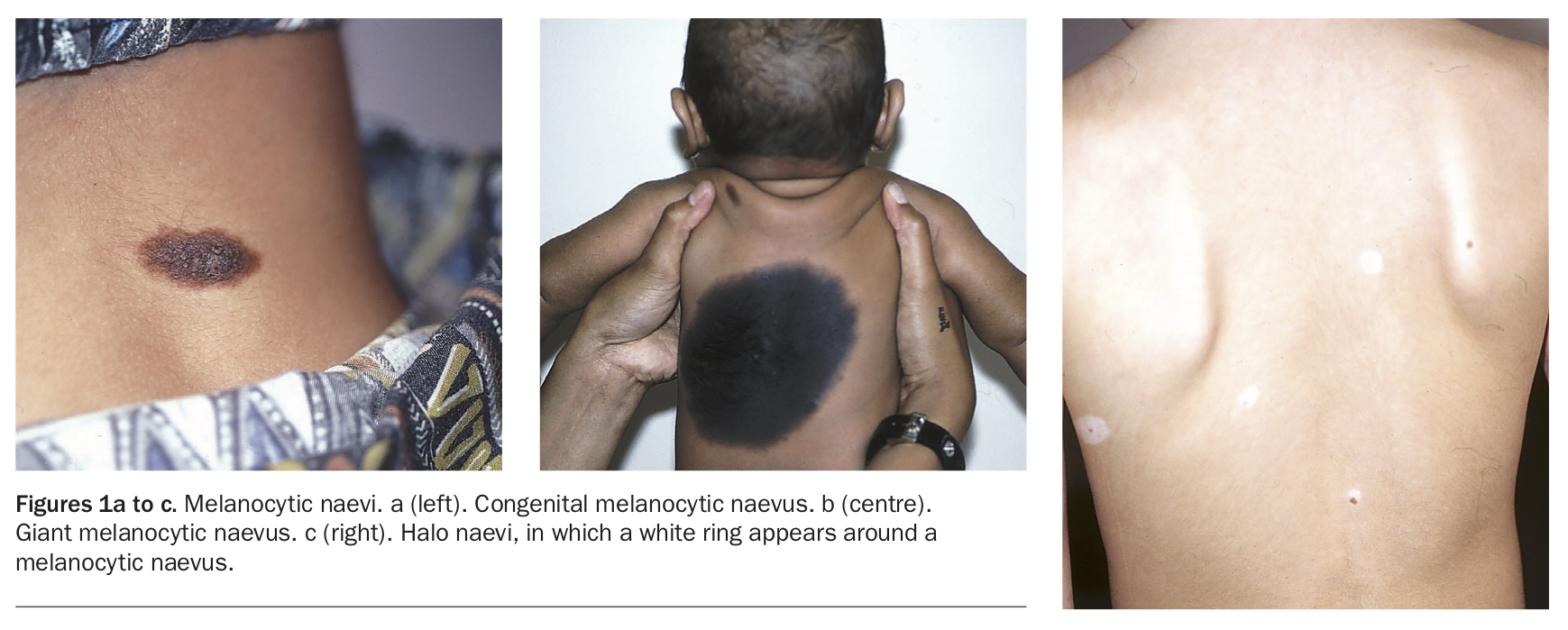
A melanocytic naevus is a benign collection of pigmented naevus cells. Most melanocytic naevi (often known as ‘moles’) are not present at birth and are termed acquired. However, they can be congenital, occurring in about one to two in 100 newborns (Figure 1a). The size of melanocytic naevi is highly variable; congenital lesions tend to be larger and can be extensive.
{kind=link}
Large congenital melanocytic naevi
Very large melanocytic naevi, with a projected adult size of 20 cm or more, are invariably present at birth, occur in about one in 20,000 births and are often covered in long dark hair (Figure 1b). They may be raised, with a pebbled surface and occasionally nodules. They may occur in a garment distribution on the trunk and may be surrounded by numerous satellite lesions.
Classically, this type of lesion is associated with early onset melanoma; however, this is still very uncommon even in the setting of large naevi. These large lesions, particularly when there are two or more discrete lesions, may also be associated with other abnormalities, including neurological problems. They may present a serious cosmetic issue particularly if located on the face.
Acquired melanocytic naevi
Nearly all children develop at least some melanocytic naevi after the age of 2 years; they can appear at any time up to the age of about the mid-20s. Most are completely harmless and do not require treatment. The number of lesions is determined by a combination of genetic potential and degree of sun exposure. Although melanocytic naevi are most common on sun-exposed sites, they can occur anywhere on the body.
Presentation, life cycle and complications
The appearance of melanocytic naevi is very variable. Colour varies from pink to brown to black, the latter being seen particularly in dark-skinned individuals. Naevi on the scalp often have a pale centre. The lesions may be associated with a variable amount of hair. The shape is usually round to ovoid, but the edge can be somewhat irregular.
It is not always appreciated that melanocytic naevi have a life cycle. It is normal for them to change slowly with time (over years) in size and colour, and eventually they involute so that older people have very few. At puberty they often darken, enlarge and may become hairy, and these normal changes often cause concern about melanoma.
Certain events may complicate all pigmented naevi. Occasionally, they may become itchy or swollen. In some cases, a white halo may appear around the naevus, termed halo naevus (Figure 1c). In children with atopy, dermatitis may localise around naevi. Pedunculated lesions may strangulate, making them look suddenly and temporarily black. All these changes are benign.
The risk of melanoma in children with small melanocytic naevi is negligible; melanoma in prepubertal children is very rare. In those with large congenital naevi, melanoma may uncommonly occur before puberty. In at least half the cases of melanoma occurring in patients with giant melanocytic naevi, the malignancy is found in areas other than the naevus. Therefore, removing the naevus does not completely remove the melanoma risk.
Melanoma risk is correlated with the number of naevi and family history of melanoma. Some families have a history of numerous, unusual-looking naevi that are associated with multiple melanomas. Termed ‘dysplastic naevus syndrome’, this is quite uncommon. Many patients with multiple naevi never have a melanoma.
Treatment of melanocytic naevi
Most melanocytic naevi do not require treatment. In children, the strongest indication for removal of most melanocytic naevi, particularly small ones, is not concern about their malignant potential but cosmetic embarrassment. Surgical removal of cosmetically distressing lesions can be considered before the child starts school. Sometimes the appearance of the lesion can be improved simply by removal of hair, if present. This may be achieved with hair removal laser therapy. The response to other laser therapy is poor.
Removal of large lesions is rarely easy and may involve numerous complex surgical procedures. Laser treatment may be used, but results are variable. These cosmetic procedures still leave a cancer risk, and the cosmetic effect may not be lasting. Referral to a dermatologist is recommended for any newborns with large lesions.
Mongolian spot
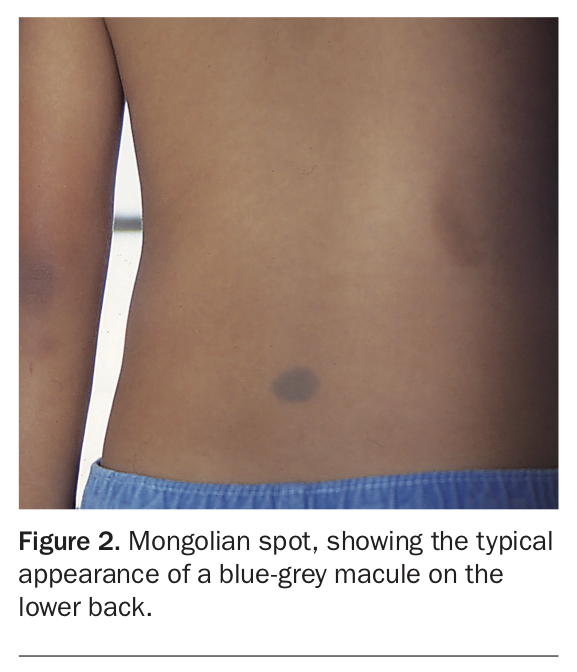
Mongolian spot is a very common congenital lesion in Asian babies and is seen occasionally in children of European background. Typically, a Mongolian spot is a blue-grey macule, occurring most often on the lower back, although they can also be found on the limbs (Figure 2). Some are quite large. These lesions usually resolve spontaneously during the first decade of life.
{kind=link}
Café au lait macule
Although most doctors think of neurofibromatosis when they see the flat, well-demarcated, light brown lesions of café au lait macules, these lesions are in fact common as solitary birthmarks and are benign and without significance (Figure 3). They are permanent and darken in summer with sun exposure. Neurofibromatosis needs to be considered only when six or more lesions are present, particularly if there is freckling in the axillae and groin.
{kind=link}
Café au lait macules can be lightened with laser treatment but have a tendency to recur.
Mosaic disorders of pigmentation
Not all birthmarks involving melanocytes are caused by increased numbers. Naevoid areas of hyper- and hypopigmentation are also part of the naevus spectrum. The patches are usually linear. These lesions may resemble epidermal naevi, but when examined closely are completely macular. Most are harmless. However, syndromes such as McCune-Albright syndrome, where macular hyperpigmentation is associated with bone and endocrine abnormalities, are well known.
Epidermal naevi
Epidermal naevi are the least common and most heterogeneous group of naevi. These lesions are composed of any element present in the epidermis and dermis, including keratinocytes (nonorganoid naevi) and glands (organoid naevi). This results in areas that are darker or lighter than surrounding skin. Epidermal naevi can be part of the epidermal naevus syndrome, which is associated with other abnormalities, particularly of the skeleton, eyes and central nervous system.
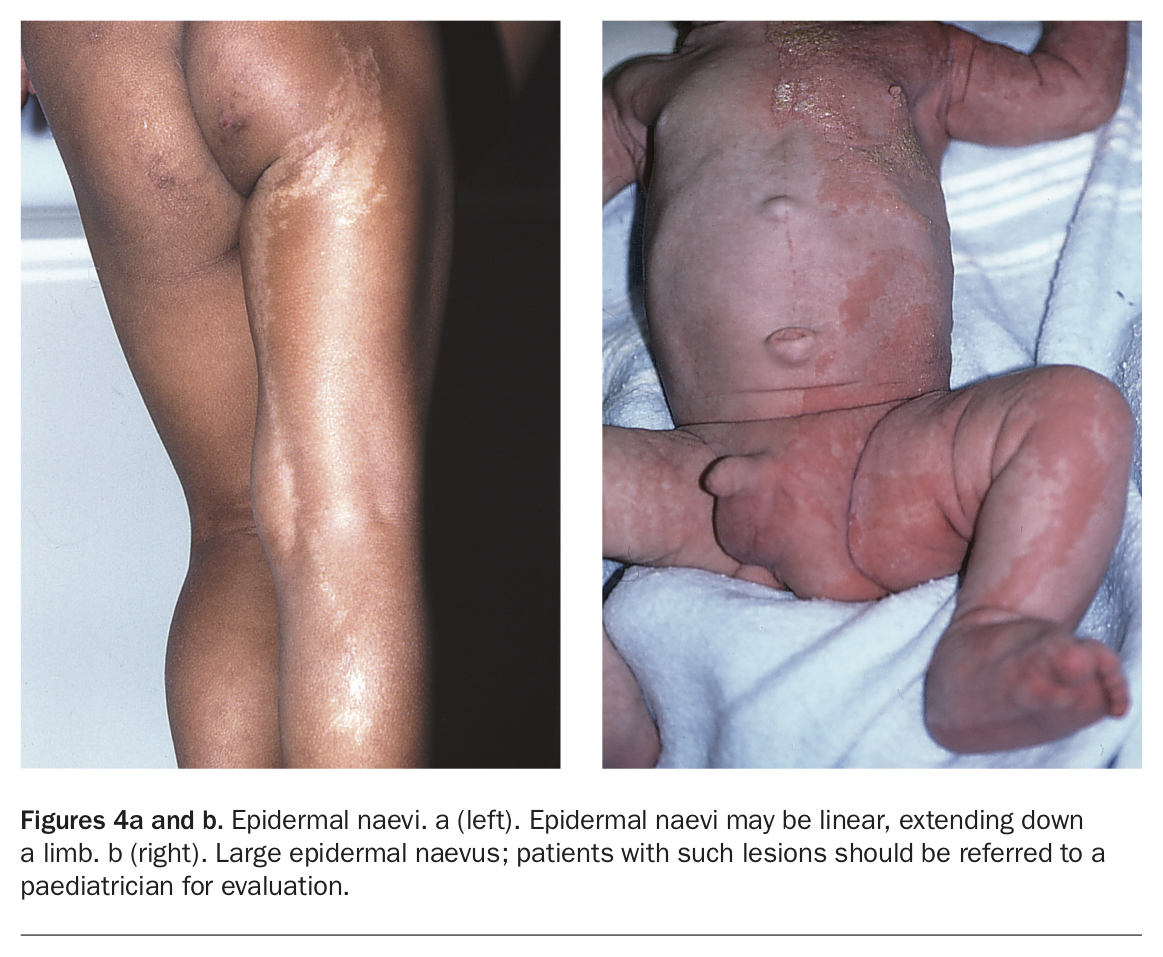
Epidermal naevi are not always obvious at birth. They may present for the first time in early childhood and then extend for several years. They can be linear, extending all the way down a limb (Figure 4a). Like melanocytic naevi, they may enlarge and become more problematic at puberty, mainly because of cosmetic and functional concerns. Malignancy is rarely a complication, except in patients with naevus sebaceous.
{kind=link}
Genetically, epidermal naevi most often arise from mosaic and somatic postzygotic mutations. The genes involved have been elucidated in many of them.
Epidermal naevus syndrome
In epidermal naevus syndrome, epidermal naevi are associated with abnormalities of the skeleton, eyes and central nervous system. The naevi in this syndrome are often quite extensive, occurring over large areas of the body in linear whorls and streaks (Figure 4b). Children with large epidermal naevi should be referred to a paediatrician for evaluation.
Naevus sebaceous
Naevus sebaceous is the most common type of epidermal naevus, with an incidence of 1 in 1000 live births. Naevus sebaceous consists predominantly of sebaceous glands and usually occurs on the head and neck. It is usually present at birth, appearing as a hairless, orange-yellow plaque (Figure 5).
{kind=link}
Unlike most other epidermal naevi, naevus sebaceous has a small malignant potential and may be complicated by carcinoma, most often basal cell carcinoma, in late teenage to adult life. Because of this, it may be wise to surgically remove these lesions prophylactically by the time the patient is 15 years old; they are rarely large or difficult to excise. They are also often removed for cosmetic reasons.
Verrucous epidermal naevi
Naevi composed of keratinocytes (verrucous epidermal naevi) have the appearance of warty linear streaks (Figure 6). They may be mistaken for warts or even lichenified dermatitis.
{kind=link}
Treatment of epidermal naevi
If an epidermal naevus is localised, the best treatment is complete full-thickness excision. Laser therapy is helpful, but the lesions usually recur after treatment. In most cases, epidermal naevi are benign and only a cosmetic problem. However, in some locations, such as the genital area or fingers, they may become a functional problem. These naevi are sufficiently unusual to warrant referral of affected patients to a dermatologist in most cases.
Vascular birthmarks
Haemangioma of infancy
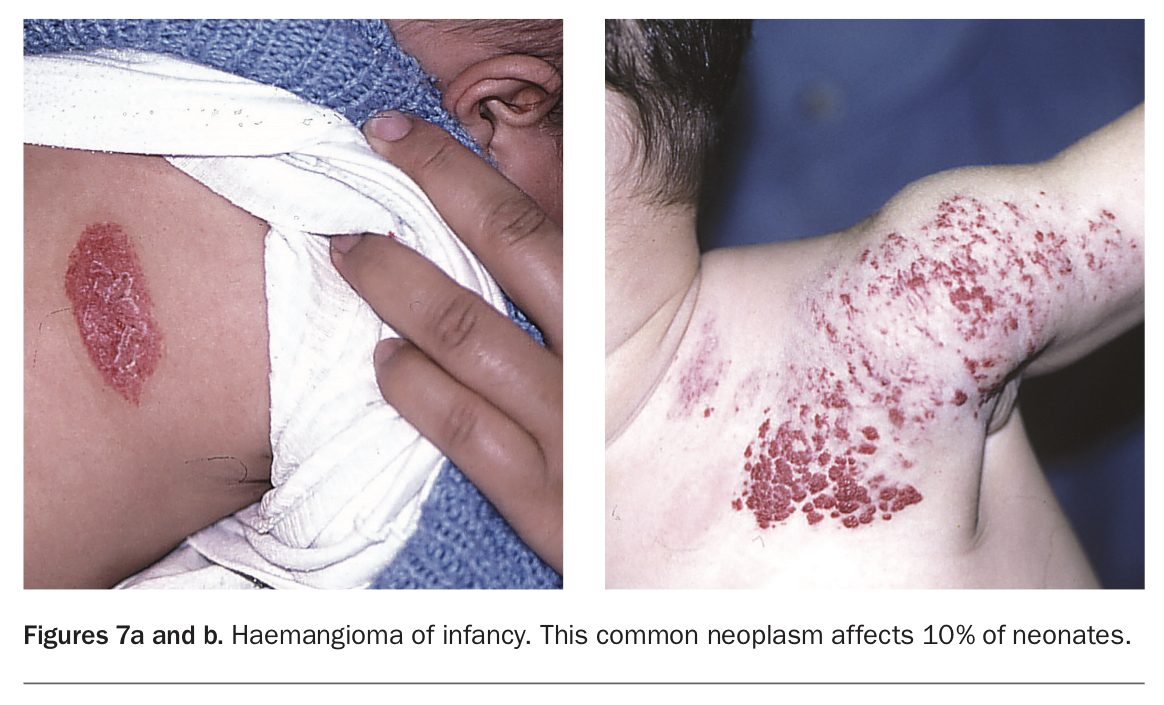
Haemangioma of infancy (previously termed capillary haemangioma or strawberry naevus) is a common neoplasm affecting 10% of neonates (Figures 7a and b). It is more common in girls and premature babies. Haemangiomas are not usually present at birth but appear within the first month of life, often initially as an area of pallor, erythema or telangiectasia. There is then a period of growth, usually no longer than about six months. The lesions rarely reach very large proportions. After stabilising, they slowly regress, resolving substantially by the time the child is of school age and completely by the age of 9 years.
{kind=link}
Many haemiangiomas of infancy are superficial, but some have a deep component. The characteristic appearance is of a bright red nodule, with the deep part appearing bluish and obviously below the skin surface. Sometimes, the entire lesion is deep, making it difficult to distinguish from a vascular malformation (see below). During regression, grey areas appear on the surface and are a good prognostic sign. The superficial portion usually resolves before the deep one does. In 20% of cases, there is more than one lesion.
Complications of haemangiomas
Most haemangiomas are uncomplicated and never require any form of intervention. When complications do occur, the most common is ulceration. This occurs most often under the nappy and on the lip. It is important to be aware of ulceration as a complication, because affected children are sometimes reported as cases of child abuse. Ulceration is usually treated conservatively with hydrocolloid dressings; however, persistently ulcerated lesions heal with oral propranolol. Referral to a dermatologist is recommended in cases such as these.
Other complications of haemangiomas are unusual. Bleeding and infection occur rarely and, if dermatitis occurs, it may localise to the lesion.
Parents often report that the worst impact of their child’s haemangioma, particularly if on a visible area such as the head or neck, is the comments it attracts from strangers in public places, especially supermarkets. Parents often need support and encouragement to develop resilience to this intrusion.
Treatment of haemangiomas
Most haemangiomas do not cause problems and, because of their natural history, no treatment is recommended. However, doctors should beware the following situations:
- facial lesions that may become disfiguring if they enlarge
- lesions that interfere with an orifice (ear, nose, genitals or mouth)
- lesions that may occlude an eye (which may cause blindness)
- rapidly growing large lesions
- large, flat facial lesions around the mouth (these are associated with laryngeal haemangioma that can cause dangerous airway obstruction).
In these cases, treatment with oral propranolol is now gold standard to halt progression and speed up involution. Treatment should be started as early as possible, and urgent referral to a paediatrician or dermatologist is essential. Treatment with propranolol is highly effective, well tolerated and very safe. Smaller, flat lesions may be treated with topical timolol, but this is much less effective than oral therapy.
Any baby with a haemangioma of infancy should be closely followed up. Large haemangiomas of infancy may leave residual stretched tissue and telangiectasia, which may require later surgical intervention and pulsed dye laser therapy.
Naevus flammeus
Naevus flammeus, also known as a ‘stork mark’, is seen in 50% of newborns. These lesions are seen on the glabella, upper eyelids and nuchal area as irregular red macules that become more obvious when the infant cries.
When these lesions occur on the face, they invariably resolve by 12 months of age. However, those occurring on the nuchal area persist into adult life in many cases and are found in 10 to 20% of adults.
Capillary malformation
Capillary malformation (port wine stain) is encountered in one in 1000 births (Figure 8). Although present at birth, a capillary malformation is not always obvious and may not be diagnosed for several months.
{kind=link}
In capillary malformation, the lesion consists of excess superficial capillaries that were formed early in fetal life. Because of this, the cutaneous lesion may be the ‘tip of the iceberg’, with underlying abnormalities of vessel, soft tissue, nerve and bone. Unlike haemangiomas, capillary malformation lesions are permanent, and do not undergo a growth and resolution phase. Generally, they tend to darken with age and may become thickened, particularly at puberty.
Complications of capillary malformations
Capillary malformations on the face in the distribution of the first trigeminal nerve, particularly if involving the upper eyelid, may be associated with epilepsy and ocular abnormalities (Sturge-Weber syndrome). When found on the midline over the lumbosacral spine, they may be associated with abnormalities of the lower spinal cord.
Lesions on the lower legs may be associated with soft tissue hypertrophy and underlying vascular anomalies (Klippel-Trenaunay syndrome). When such a lesion feels warmer than surrounding skin and is associated with soft tissue hypertrophy or pulsation, it may in fact be an arteriovenous malformation.
Children with these rare lesions should be referred to a paediatrician. They will usually require MRI investigation.
Treatment of capillary malformations
Capillary malformations may be treated by pulsed dye laser, and this is best done as early as possible in the child’s life as response is best in the first two years. Children with capillary malformations should be referred to a paediatric dermatology unit at a children’s hospital. Treatment may be performed very early, even in the first month of life. This is limited by the pain of the procedure and the risk of general anaesthesia in a baby. The result of laser treatment is usually not perfect; however, a substantial number of children achieve some degree of lightening.
Extensive lesions require imaging to determine whether there are underlying abnormalities. Patients with lesions on the face may require MRI of the brain and ophthalmology referral.
Other vascular malformations
Other types of vascular malformation are rare and consist of a mixture of subcutaneous venous and lymphatic elements. Again, they form early in fetal life. In the past, they were termed cavernous haemangiomas.
These lesions may be small or large, sometimes infiltrating muscles and joints. Their appearance is highly variable, but usually there is obvious hypertrophy and sometimes visible enlarged veins, discolouration or bruising. When the lesion is predominantly lymphatic, it may be repeatedly infected or leak clear fluid (Figure 9). Ultrasound or MRI is required to determine the exact nature of the lesion.
{kind=link}
Previously, these lesions were generally treated with surgical excision, often with great difficulty and variable results. More recently, interventional radiologists have used sclerosant therapy under fluoroscopic guidance. Some lasers, such as the long-pulsed neodymium:yttrium-aluminium-garnet (Nd:YAG) laser, have enough penetrance to treat intracutaneous and superficial malformations. These modalities are available at only a few major centres with specialised expertise.
Conclusion
Although it is unusual for babies to be born with skin lesions, nearly all children have at least some melanocytic naevi after the age of 2 years. Birthmarks are rarely dangerous and hardly ever have malignant potential but may be cosmetically embarrassing, particularly if they occur on the face. Some birthmarks, particularly the lesser known epidermal naevi, may be mistaken for other lesions such as warts or even dermatitis. Ulcerated haemangiomas may be mistaken for child abuse. Some lesions can interfere with function.
Most birthmarks do not resolve spontaneously in childhood; however, the common haemangioma of infancy always does and so usually does not need treatment. If they are small, most melanocytic and epidermal birthmarks can be easily removed surgically, with or without the aid of laser therapy, if the child and parents wish it. However, removal of larger lesions can present a significant challenge.
Vascular lesions are often the most difficult to treat because they are too large to be excised, and the visible component on the skin surface may be the tip of the iceberg. A combination of surgery, laser and sclerotherapy is used to treat these.
Although malignant potential and interference with function are important, the most common reason for removal of a congenital lesion is cosmesis. With the exception of laser therapy for capillary malformations, which is most effective early in life, the decision to have treatment can, and should, involve the wishes of the child. MT
COMPETING INTERESTS: None.
Further reading
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.