Common skin problems in children. Infectious rashes and infestations

Skin infections
Skin conditions
Cutaneous infections and infestations are common in children; the key to their diagnosis is a positive culture or scraping to confirm infection and/or response to anti-infective agents.
- Although impetigo is usually due to Staphylococcus aureus, certain groups (including Aboriginal and Torres Strait Islander people) are particularly susceptible to group A Streptococcus infections.
- Children with recurrent S. aureus infections are usually carriers of this bacterium.
- Not all cases of folliculitis are due to S. aureus; Pseudomonas aeruginosa acquired from contaminated water or bath toys may be responsible.
- Most acute genital infections in children are due to group A Streptococcus.
- Tinea capitis is a childhood condition, which may at times present with an inflammatory mass.
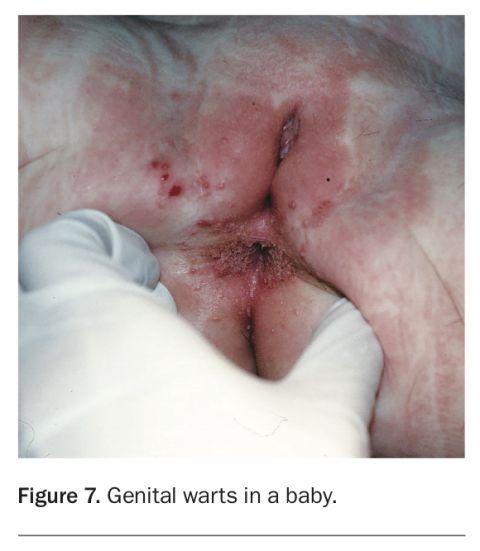
- Genital warts in children should always be a cause for concern.
- Scabies is often a very difficult diagnosis to make; it is often mistaken for dermatitis.
Few children escape having a Staphylococcus aureus skin infection of some sort, a viral exanthem, warts, molluscum contagiosum, head lice or scabies at some time in their childhood. Although most children with a rash are assumed to have an infection or a bite, this is not always the case, and many noninfectious rashes also affect children.1,2 Positive cultures or scrapings are needed to confirm the diagnosis of an infectious rash or infestation.
Bacterial infections
Impetigo
Impetigo presents most often in children, although it may be seen at any age. It is caused most often by S. aureus and less often by Streptococcus pyogenes, and both organisms may occur together. Certain groups, including Aboriginal and Torres Strait Islander people, appear to be more susceptible to S. pyogenes infections. Impetigo is contagious, and if it is due to S. pyogenes, glomerulonephritis may follow within eight weeks. It is always helpful to confirm the diagnosis by a skin swab to define the infective organism and establish antibiotic susceptibility.
Impetigo presents in three ways:
- crusted or nonbullous impetigo, presenting as yellow crusts and erosions that are itchy or irritating but not painful; this is the most common presentation and is often subacute
- bullous impetigo (Figure 1), which is always caused by S. aureus, and presents as mildly irritating blisters that erode rapidly leaving a brown crust
- ulcerative lesions, which are always caused by S. pyogenes.
{kind=link}
Until culture results are available, it is reasonable to suspect S. aureus as the pathogen and to treat accordingly. Minor lesions may be successfully treated with topical antibiotics.
Community acquired methicillin-resistant (but not multiresistant) S. aureus (MRSA) is common. Treatment should be guided by susceptibility testing. These strains are generally susceptible to clindamycin or trimethoprim plus sulfamethoxazole as well as the drugs normally chosen for the multiresistant strains, such as vancomycin. It is always helpful to ask for expert advice from the laboratory or an infectious diseases physician before treating patients infected with any form of MRSA.
It is not uncommon for impetigo to become recurrent or resistant to treatment. Sometimes this is caused by an underlying dermatosis, but usually it is due to chronic carriage of S. aureus. This can be confirmed by taking a nasal and/or perineal swab for culture, depending on the location of the impetigo lesions. If swabs are positive, the whole family and close contacts need decolonisation treatment. Mupirocin 2% nasal ointment should be used intranasally twice daily for seven days and half a cup of bleach should be added to bathwater or, if showering, an antiseptic wash containing triclosan or chlorhexidine should be used for four weeks. During this time, clothes, towels and sheets should be washed in hot water. If lesions continue to recur despite these measures, treatment with a combination of rifampicin and flucloxacillin or clindamycin usually ends the problem.
Folliculitis and boils
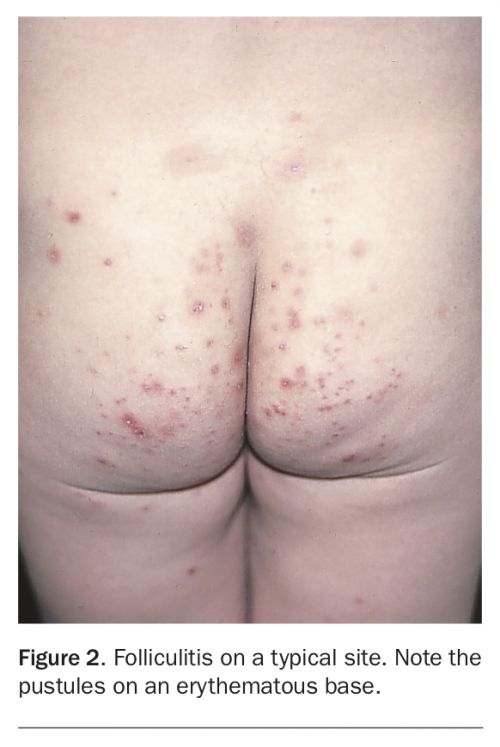
Folliculitis is a common condition, particularly in hot weather. It presents with mildly itchy pustules on an erythematous base (Figure 2). It may affect any part of the hair-bearing skin, and it often occurs in macerated areas, including under dressings or nappies.
{kind=link}
Although folliculitis is most often due to S. aureus infection (patients are often chronic carriers of S. aureus), this should be confirmed by culture. Folliculitis may also be caused by Pseudomonas aeruginosa (usually acquired from contaminated water supplies or mouldy bath toys), pityrosporum yeasts, dermatophytes and herpes simplex virus.
Folliculitis caused by S. aureus is treated in the same way as impetigo with a staphylococcal carrier state. For pseudomonal folliculitis, identify the source (by culturing water in the hot water tank, for example) and cease contact with it until it has been treated. If a child is still wearing nappies at night and the folliculitis involves the buttocks, there is usually marked improvement when nappies are no longer worn.
Boils are a deep form of folliculitis and are usually tender and painful. The causative organism is generally S. aureus, occasionally in association with S. pyogenes. It is common for boils to be recurrent, but this does not usually indicate any form of immunological abnormality. Small lesions may be treated with drainage alone, but it is usual to treat them in the same way as folliculitis and recurrent impetigo.
Streptococcal genital and perianal infections
Healthy prepubertal children do not suffer from candidal infections of the genital area, unlike adults. In children, most cases of infection of the penis, vulva and perianal area are due to the group A streptococcus S. pyogenes, which may possibly be acquired by haematogenous spread from the throat.
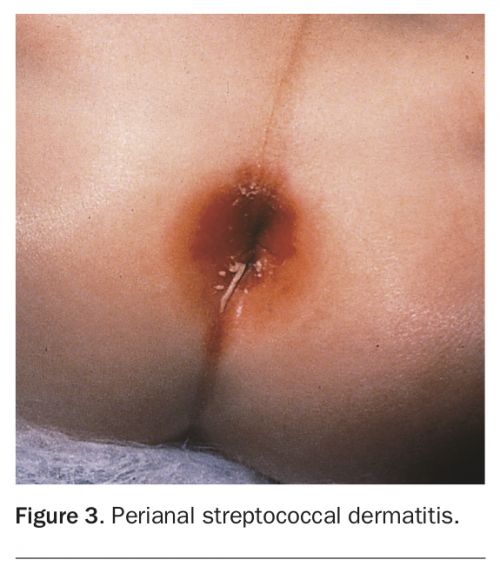
Streptococcal perianal dermatitis in children presents with a persistent perianal eruption (Figure 3). The rash is itchy and tender and may be complicated by painful fissuring. There is usually well-defined erythema, with scaling or weeping, which may extend to several centimetres from the anal verge. Bleeding and discharge may occur.
{kind=link}
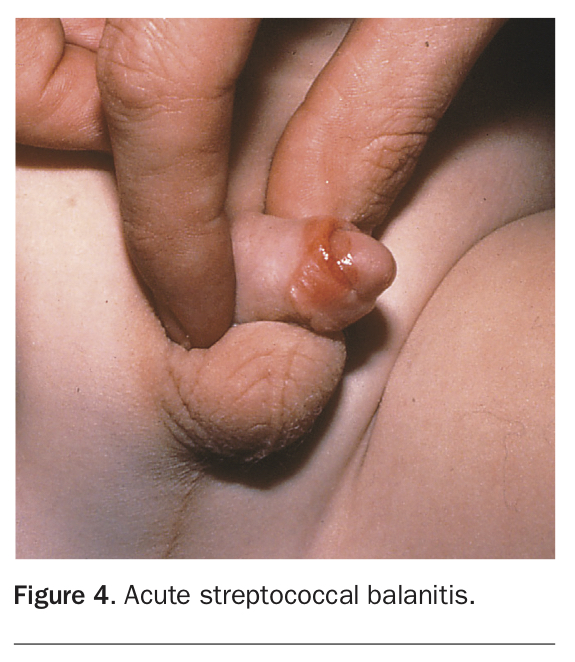
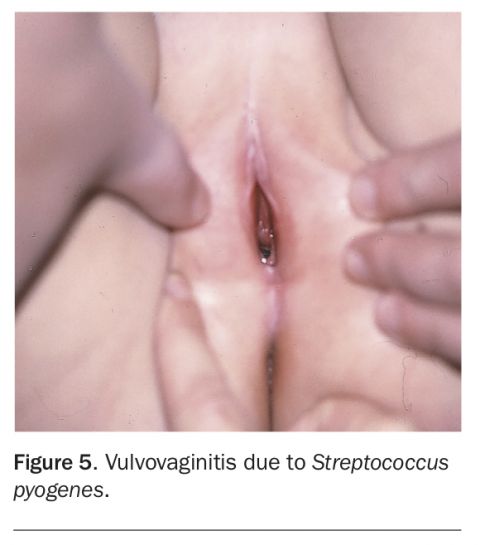
Acute balanitis (Figure 4), which is seen most often in uncircumcised boys, and vulvovaginitis (Figure 5) in girls are most often due to S. pyogenes. They may occur in conjunction with perianal lesions or in isolation.
{kind=link}
{kind=link}
Confirmation of the infection should be made by culturing a skin swab, and a low vaginal swab in cases of vulvovaginitis. The infection must be treated with oral antibiotics (penicillin, cefalexin or roxithromycin), and unless a full 10-day course is adhered to, recurrence is common. It is helpful to use topical mupirocin ointment twice daily at the same time to prevent recurrence.
Some children with this infection do not immediately lose their symptoms after adequate antibiotic treatment. This does not necessarily mean that the infection is persistent, and a second swab should be done before repeating antibiotics. Many simply have residual dermatitis or psoriasis that has been flared by the infection, and treatment with topical 1% hydrocortisone is all that is required.
Common fungal infections
Tinea
In children, tinea (dermatophyte infection) most often involves the scalp, face and body. Tinea pedis is less common in children than adults. In children, tinea is often acquired from dogs, cats, pet mice and guinea pigs, but human pathogens may also be responsible, especially in the case of tinea pedis. Animal dermatophytes tend to produce a more inflammatory and acute form of tinea.
Tinea capitis
Tinea of the scalp is very uncommon in adults and occurs almost exclusively in children. Usually there is loss of hair, which occurs most often in round patches, but occasionally is diffuse. This is associated with itching and scaling. A kerion is a very acute form of tinea capitis, usually caused by an animal dermatophyte, in which a large boggy, pustular mass appears on the scalp. Despite the alarming appearance, the child is well systemically and the lesion is not severely tender, which differentiates it from a bacterial infection where there would be fever and pain.
If tinea capitis is suspected, fungal culture of skin scrapings and plucked hairs should be done before starting therapy. It is important to confirm the diagnosis for future monitoring and to justify what is usually a prolonged course of oral treatment, but treatment may start before the results are available. Wood’s light examination is unreliable for diagnosis.
Topical therapy is ineffective in treating tinea capitis and oral treatment must be used. Although tinea capitis is not a PBS indication for terbinafine, this antifungal agent has the advantage of being effective in about six weeks with once daily dosing. Overseas trials have confirmed its safety and usefulness in children. Other oral antifungals including fluconazole and itraconazole are also effective.
At the end of the treatment period, the culture should be repeated. If the culture is negative, the hair has regrown and there is no scalp inflammation, treatment can be ceased. If the culture is positive, continue therapy, repeating the culture every four to six weeks. Therapy may be stopped when a negative culture is obtained and hair has regrown. Occasionally this may take several months. Permanent alopecia is a very unusual sequel of tinea capitis.
Ketoconazole shampoo and selenium sulfide shampoo reduce shedding of spores and are a useful adjunct to therapy; however, if used alone they are ineffective.
The use of antibiotics, oral corticosteroids and surgical debridement does not add to the management of a kerion. This is an important point as children with a kerion are sometimes taken to theatre in an attempt to drain the mass. This is unnecessary as the lesion does not contain pus.
Tinea corporis
Tinea corporis usually presents with annular, scaly lesions; there may be one or many (Figure 6). Usually they are itchy. Many rashes that are common in children, such as dermatitis and psoriasis, may mimic tinea, but a fungal scraping for culture makes it possible to differentiate tinea.
{kind=link}
Localised tinea corporis in children is easily treated with topical antifungal creams, but if the infection is widespread, longstanding or has been treated with topical corticosteroids, oral treatment with griseofulvin is indicated, using the same antifungals as for tinea capitis. Griseofulvin may be used but is slow to work and hampered by the side effects of diarrhoea and photosensitivity. Clinical improvement usually occurs promptly, but ceasing treatment prematurely results in relapse. Treatment should be continued for a minimum of three weeks after resolution of all signs and symptoms.
Common viral infections
Warts
Warts are benign tumours that are seen at any age but most often in children. Common warts usually occur on the hands, feet and extensor surfaces. Facial warts often take the form of multiple tiny brown papular lesions. Warts adjacent to mucosal surfaces are often filiform. There is no specific or reliably effective treatment for warts, but in children they often resolve spontaneously within two years, making aggressive or painful therapy inappropriate.
The presence of warts in the genital area in children of either sex should raise the question of child sexual abuse (Figure 7). In children under 2 years of age there is the possibility of vertical transmission from a mother with genital or cervical warts. In theory, warts may be acquired from a parent with warts on the hands or by autoinoculation if the child has warts elsewhere on the skin. Although many published studies have stated that genital warts in children are not always sexually acquired, the fact is that children rarely disclose sexual abuse. Given that genital warts are usually sexually acquired in adults, in my opinion this finding is always cause for concern. The origin of genital warts in children is still controversial.
{kind=link}
There are many over-the-counter treatments for warts. Plane warts may respond to topical tretinoin 0.05% cream, and genital warts to topical podophyllotoxin or imiquimod. Painful procedures such as cryotherapy, cautery or laser are often impractical in children.
Immunotherapy with the topical sensitiser diphencyprone is effective and well tolerated by children but can be hazardous because of the risk of severe allergic contact dermatitis and the possibility of systemic reactions. This treatment requires referral to a dermatologist.
It is often best to wait for warts to resolve spontaneously, but when they are causing distress or embarrassment and conservative treatment has failed, specialist referral of the patient is recommended.
Molluscum contagiosum
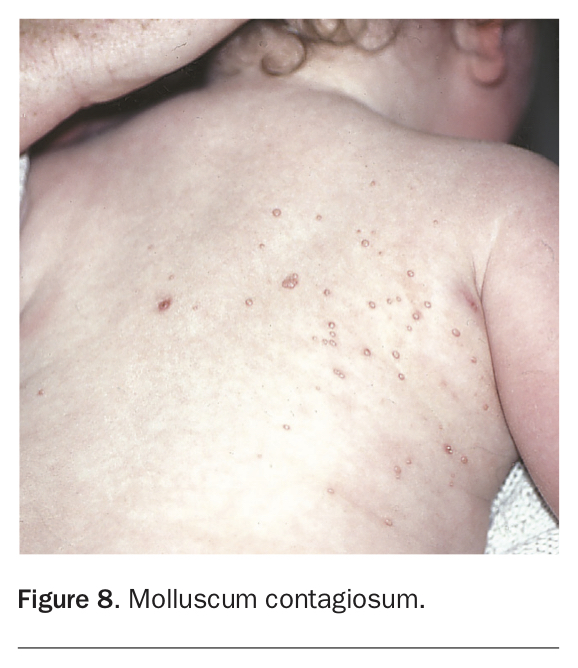
Molluscum contagiosum is a common contagious poxvirus infection (Figure 8). In young children, the lesions occur anywhere on the body and the infection is usually acquired from family members or others with whom they swim or bathe as the virus is spread in water.
{kind=link}
The typical lesion is a pearly papule with central umbilication and a core that may be expressed by applying firm pressure to either side of the lesion. With dermoscopy, it is usually easy to see the central core. This differentiates mollusca from HPV induced lesions.
Molluscum contagiosum usually resolves spontaneously in immunocompetent patients, but this may take up to two years. Atrophic scarring may occur, regardless of whether the lesions are treated. The infection may be complicated by dermatitis, particularly in atopic patients, and bacterial superinfection. Sometimes just before resolution there is an inflammatory flare of all lesions.
Showering rather than bathing may reduce the spread of lesions because of the transmissibility in water. It is not practicable or necessary to isolate children with molluscum contagiosum. Most chemical therapies are ineffective, although topical imiquimod works in some cases. In children, conservative management – i.e. waiting for spontaneous resolution – is usually best, unless lesions are widespread and interfering with lifestyle and function. If treatment is needed and the lesions are small, they may be curetted or expressed. When lesions are numerous, patients may require sedation, nitrous oxide analgesia or even a general anaesthetic. Secondary dermatitis requires treatment with topical therapy, and it is helpful for the patient to have a tube of mupirocin ointment at home in case of superinfection.
Viral exanthemata
Now that the classic exanthemata such as measles and rubella are uncommon because of immunisation, most of the viral rashes seen in children are due to enteroviridae such as coxsackie viruses and echovirus. Despite vaccine being available, varicella is still encountered from time to time.
Generally, viral exanthemata have two main presentations in children:
- generalised, bilaterally symmetrical maculopapular rashes, often with confluence on the face and involvement of the helix of the ears
- peripheral papular eruptions, mainly on the arms and legs.
In most cases, the child is well and afebrile but the rash may be quite itchy. Children may have had mild fever and diarrhoea at the onset of the rash. It is not uncommon for the lesions to take several weeks to resolve, and only symptomatic treatment is possible.
A few viral infections have specific presentations. These include:
- parvovirus infection (slapped cheek disease), which presents with confluent erythema of the cheeks associated with a reticulate rash on the arms and legs
- hand, foot and mouth disease, which presents with small vesicles on the hands and feet associated with mouth ulcers
- roseola, due to herpes virus 6, which is a transient maculopapular rash associated with fever and lymphadenopathy and seen in children under the age of 3 years
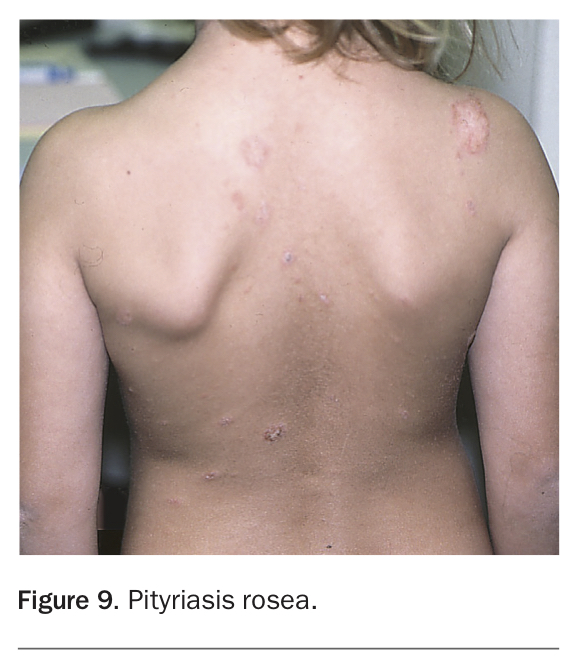
- pityriasis rosea (Figure 9), which presents with a single scaly herald patch, followed by multiple ovoid, erythematous macules with a peripheral scale mainly on the trunk; this is probably viral but is yet to be confirmed
- herpes simplex infection, which most often causes a stomatitis in children and only generalises in those with eczema, causing a widespread vesicular rash
- varicella, which presents with fever and a vesicular eruption that rapidly forms umbilicated pustules and crusts; all mucosal surfaces, including the conjunctivae, may be involved.
{kind=link}
Common infestations
Scabies
Scabies is caused by infestation with a tiny six-legged insect that is a specific human pathogen. It is not visible to the naked eye. It is spread by close physical contact between infected persons and is not acquired from animals. Scabies is common in children and, if untreated, can spread to all members of a patient’s family. Indigenous children living in crowded communities are particularly susceptible and scabies is a major cause of morbidity in these communities because of secondary bacterial infection with S. pyogenes to which this group is susceptible (see above).
The diagnosis of scabies is often difficult, especially if it is not suspected. The clinical picture is variable because it is due to an allergic reaction to the mite and this is very individual. Some patients have very few signs, and occasionally the only complaint is itch without an obvious rash. The itch exacerbates at night and after hot showers. Typically, there is an itchy, excoriated but nonspecific rash on the trunk associated with scaly burrows on the fingers and wrists. Papular and nodular lesions are often seen around the major flexures in children, and in babies and toddlers there are often vesicles and pustules on the palms and soles and sometimes on the scalp. Secondary bacterial infection may occur.
Confirmation of the diagnosis is made by microscopy of scalpel scrapings from a burrow. Dermoscopy is also useful in visualising burrows. The main pitfall in using this technique is the selection of a suitable burrow, as these are few in number and difficult to identify. Therefore, the most practical diagnostic test may be response to antiscabetic medication.
For the topical treatment of scabies, the treatment of choice in terms of safety and efficacy is permethrin 5% cream. Benzyl benzoate 25% emulsion can be effective in scabies if used correctly, but it is more irritating than permethrin. The treatment is applied from the neck down and left on for a minimum of eight hours for permethrin and 24 hours for benzyl benzoate. If the hands are washed during this time, the treatment should be reapplied. In central and northern Australia, scabies above the neck is common and treatment should also be applied to the face and hair (avoiding eyes and mucous membranes). In babies, the scalp and face should also be treated, and mittens should be worn to stop them sucking their hands. In all cases, the treatment should be repeated after a week.
There is some controversy regarding the treatment of scabies in babies. Although permethrin is not approved for use in those under 6 months of age, this has to be balanced against the high morbidity of untreated scabies, which can be severe in this age group. Although some authors recommend the use of 10% sulfur and 10% crotamiton cream in this age group, there may be no rationale in doing so and, in fact, safety data on these preparations are very sketchy.
For severe infestations in children aged 5 years and over, oral ivermectin may be used. It is given as two doses one to two weeks apart using 200 mcg/kg for each dose.
Head lice
Head lice are common in school children, affect all sections of society and are harmless. They are not a sign of poor hygiene. The infestation is acquired by head to head contact. Although it can be asymptomatic, the scalp and nape of neck can be itchy and nits are noticeable on the hairs. The itching can result in excoriations and lymphadenopathy can follow.
Head lice are crawling mites the size of a sesame seed. They live on the scalp but lay eggs, known as nits, on the hair. Diagnosis of active lice infestation is made by observing a live, moving mite on the scalp. This can be achieved by wet combing the hair with a fine-toothed comb after applying a generous amount of hair conditioner to dry hair. The conditioner stuns the lice and stops them crawling for about 20 minutes. Conditioner from the comb is wiped on to a paper towel and lice and nits are detected. Even when all the lice are dead, nits may remain on the hair. If they are 1.5 cm away from the scalp, they are unlikely to contain live larvae, and just represent old infestation.
Treating head lice can be difficult. Treatment resistance is well documented, and reinfestation is always a risk. Some cases can be cured by wet combing every day for 10 to 14 days until no lice are found. This method has only about a 40% success rate.
Alternatively, topical scabicides can be used. Most contain permethrin and are usually left on for 20 minutes, but maldison is another insecticide that appears to be more effective. Maldison should be left on for eight hours and is not recommended in infants aged under 6 months. Parents and even pharmacists are often worried about using these insecticides on children, and parents may need reassurance before starting treatment. Oral ivermectin may also be used as in scabies.
All head lice treatments should be repeated seven to 10 days later, and the conditioner and combing method (above) should be used the next day to check that there are no further live mites on the scalp. Between treatments, the same combing method should be used twice, with all eggs less than 1.5 cm from the scalp being removed with a head lice comb or pulled off with fingernails. These eggs may contain viable larvae. Wet combing should be repeated weekly for several weeks after cure to detect any recurrence.
Pillowcases, combs and brushes should be washed in hot water (at least 60°C). Family and close physical contacts should be examined and treated if live lice are found. The child’s school should be notified, but it is not necessary to exclude children with head lice from school after their initial treatment.
Conclusion
Most children at some time in their childhood have an infectious rash or infestation, some of which can mimic noninfectious rashes (see Practice Points). The key to the diagnosis of infectious rashes or infestations is a positive culture or scraping, which also guides treatment decisions. MT
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.