Discoid eczema – more than just dermatitis

Discoid, or nummular, eczema is a chronic form of dermatitis characterised by well-defined circular plaques. Associations include allergic contact dermatitis, low environmental humidity and excessive alcohol intake. It is managed by avoidance of triggers and use of emollients and topical corticosteroids.
- Discoid eczema is a sub-type of nonatopic eczema defined by circular or oval plaques of eczema with a well-demarcated edge.
- It tends to follow a chronic course.
- The four clinical variants of discoid eczema are exudative nummular eczema, dry type nummular eczema, discoid eczema of the hands and exudative discoid with lichenoid chronic eczema.
- Differential diagnoses for eczema include tinea corporis, psoriasis and pityriasis rosea and are important to rule out for optimal management.
- It is managed through conservative skin care measures, as well as use of emollients and topical corticosteroids.
- Secondary infection with Staphyloccocus species is common and requires treatment with systemic or topical antibiotics.
The word eczema (also called dermatitis) derives from the Greek word ‘ekzema’, meaning ‘to boil’. It is a clinical and histological pattern of inflammation of the skin characterised by pruritus and discomfort. It can be classified in several ways, one of which is morphologically.1 Discoid eczema, or nummular eczema, is one form of dermatitis that can be classified this way. Discoid eczema is defined by circular or oval plaques of eczema with a clearly demarcated edge.2,3 Many patients with eczema have at least one or two circular lesions, and few patients with discoid eczema have solely discoid lesions.4
Discoid eczema has an incidence of 2 per 1000 people and is particularly common in men aged 35 to 70 years.2,5 The exact aetiology is unknown, although a significant percentage of patients may have an underlying allergic or irritant contact dermatitis.3-7 Other associations include low environmental humidity, excessive chronic alcohol intake, staphylococcal colonisation, lifestyle factors (such as irritating soaps and fabrics and frequent exposure to hot water), trauma (the Koebner phenomenon) and certain medications including antivirals, interferon, isotretinoin, ribavirin and gold.2,3,5,8-10 Chronic venous stasis has also been implicated, especially when the discoid eczema involves the lower legs.3
Presentation
The diagnostic lesion is a coin-shaped plaque of closely-set thin-walled scaling and vesicles on a scaly erythematous base, classically on the extensor surfaces of lower limbs.2,3,11 The lesions are sharply defined and range in size from 1 to 10 cm in diameter.3 They arise rapidly from a confluence of tiny papules and papulovesicles.2,3 In the acute phase, these lesions are dull red, very exudative or crusted and highly pruritic.2 They progress towards a less vesicular and more scaly stage, with central clearing and peripheral extension. There is sometimes a drier scale and lichenification.3 The lesions subsequently fade as dry, scaly patches.2 The eruption can be precipitated by localised injury (such as from scratching, insect bites or burns), infections, contact dermatitis, dry skin or varicose eczema.4,7 Secondary lesions occur between 10 days and several months after the primary eruption in a mirror-image configuration on the opposite side of the body. It is characteristic that dormant patches become active again especially if treatment is discontinued.1
There are four clinical variants of discoid eczema.
- Exudative nummular eczema involves leakage of serous fluid and crust formation from lesions (Figure 1).1
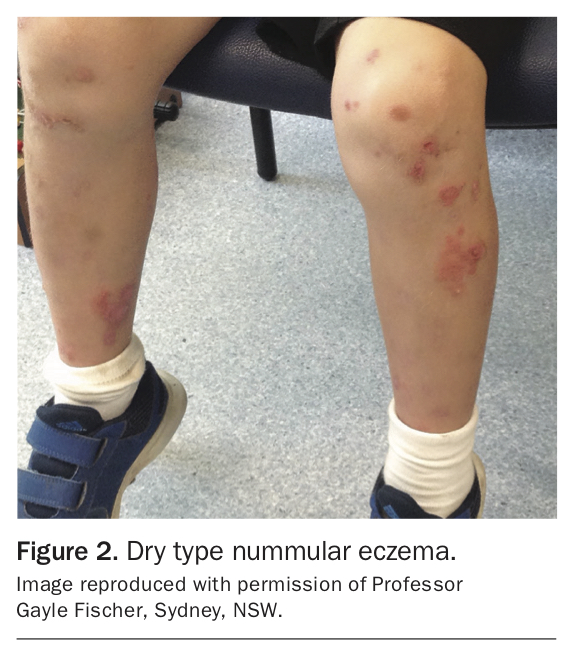
- Dry type nummular eczema is less common and consists of multiple dry scaly, round or oval discs on the arms or legs, with scattered microvesicles on an erythematous base on the palms and soles (Figure 2). Itching is minimal in this subtype. It is notably resistant to treatment and persists for years.1
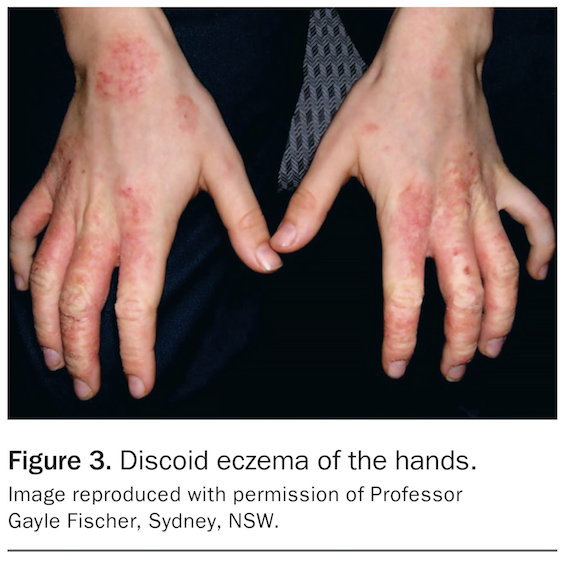
- Discoid eczema of the hands affects the dorsa of the hands or backs and sides of the fingers (Figure 3). It often develops as a single plaque at the site of the original irritant. Secondary lesions may occur locally, but generalised spread is uncommon.
- Exudative discoid with lichenoid chronic eczema is a widespread, extremely pruritic eruption characterised by discoid lesions with lichenoid and exudative phases that coexist or may alternate rapidly over several days (Figures 4a and b). After a chronic course of months or years, it may end in spontaneous cure. It occurs predominantly in Jewish adult men aged 40 to 60 years.12 There is some conjecture as to whether this is a distinct clinical entitity.13
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Differential diagnoses
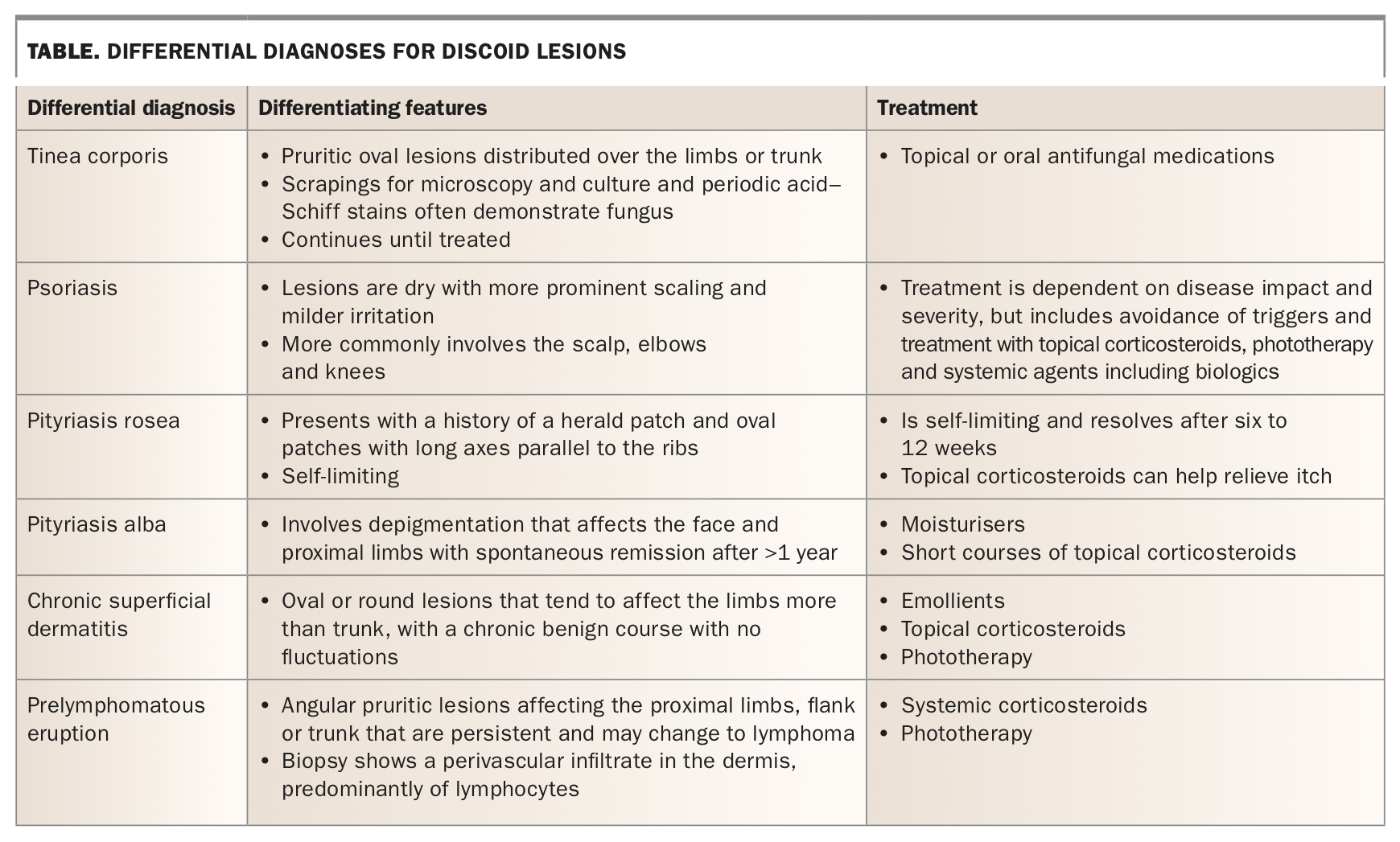
Differentiating discoid eczema from other forms of dermatitis is important for optimal management, particularly in avoiding triggers. Differential diagnoses for discoid eczema are summarised in the Table and include the following.
{kind=link}
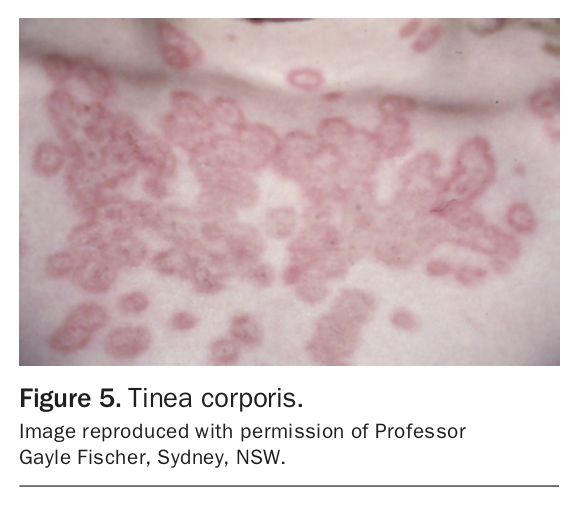
- Discoid eczema may appear to be similar to tinea corporis with central clearing. Tinea corporis is an infection often found after close contact with an infected animal, and presents as annular, scaly erythematous lesions that spread centrifugally (Figure 5).11,14
- Psoriatic lesions differ in their dryness and more prominent silvery scaling with milder irritation (Figure 6).11
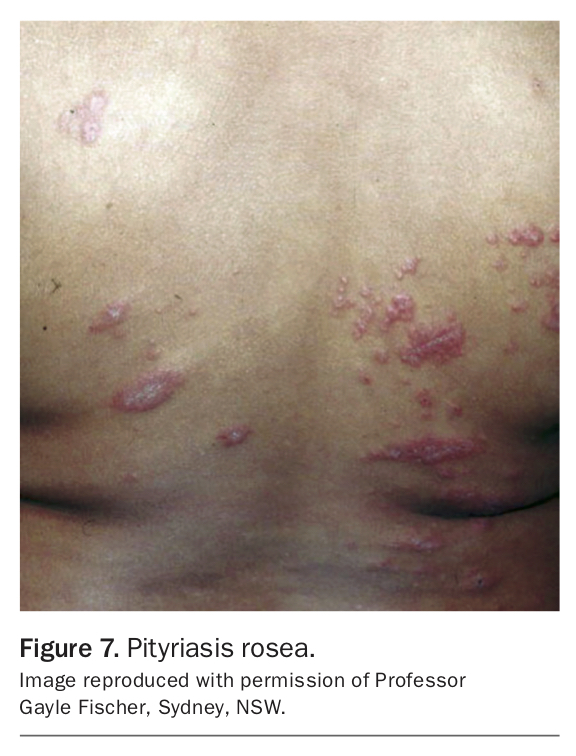
- Pityriasis rosea presents with a herald patch and salmon-coloured oval patches with long axes parallel to the ribs, although it may transiently resemble discoid eczema (Figure 7).11
- Pityriasis alba more commonly affects the face and proximal limbs in depigmented lesions.
- Chronic superficial dermatitis tends to affect the limbs more, is oval or round with no infiltration, and is chronic with few fluctuations.
- Prelymphomatous eruption more commonly affects the flank, trunk and proximal limbs with angular lesions.
- Allergic contact eczema may present with nummular lesions, although can be differentiated on history and through patch testing.3
{kind=link}
{kind=link}
{kind=link}
Discoid eczema is also more likely to occur in a generalised distribution and is less likely to occur on the face, neck, lips, ears and anogenital areas.5 30% of patients may have both discoid eczema as well as an irritant (or allergic) contact dermatitis.5
Pathophysiology
Triggers including bacterial colonisation, contact allergens, certain medications and chronic venous stasis may compromise the cutaneous lipid barrier. This results in the subsequent release of cytokines, including interferon gamma and interleukin 17, and recruitment of T cells, dendritic cells and Langerhans cells. This causes epidermal hyperplasia and the formation of the lesions characteristic of discoid eczema.3
Association of discoid eczema with surgical sites has been reported, with occurrence of the isomorphic Koebner phenomenon between three months and 10 years after surgery.10 Alcohol misuse has also been associated with discoid eczema. This relationship might be due to alcohol impairing the immune response, thus predisposing the skin to a bacterial infection, which in turn triggers the eczema.8,9 However, there is no reported association between alcohol misuse and other forms of eczema.8,9
Investigations
Discoid eczema is a clinical diagnosis.3 However, exogenous contact dermatitis should be suspected if the condition is unusually severe and persistent, or if the lesions are few, asymmetrical or of unusual configuration. In these cases, patch testing can be performed.6,7 Often, scrapings are taken for mycology to exclude tinea corporis.
Some studies have highlighted the role of infection in triggering and prolonging discoid eczema, and heavy colonisation of lesions by Staphylococcus species may increase its severity.15 Allergic sensitivity to Staphylococcus may be partly responsible for secondary dissemination.16 Thus, bacterial swabs may be taken, especially if the rash is not responsive to therapy.
Although discoid eczema does not generally require a biopsy, histological examination demonstrates a subacute dermatitis, with spongiotic vesicles and lymphohistiocytic infiltrate.2,3 Electron microscopy has demonstrated that intercellular oedema leads to a reduction in the number of desmosomes between the cells of the basal layer, whereas those in the stratum spinosum are preserved.
Management
The management of discoid eczema is aimed at restoring the natural skin barrier and minimising exposure to triggering factors. This can be achieved through short, cool showers using gentle soaps or soap substitutes. Tight clothing and irritating fabrics such as wool and nylon should be avoided.2,3
Patients should frequently moisturise, including immediately after showering. Intermittent topical corticosteroids are used to dampen eczema flares.2,3 Corticosteroid-sparing agents including topical calcineurin inhibitors (such as tacrolimus and pimecrolimus) may also be used in combination or alternately with topical corticosteroids.
Classically, coal tar pastes or ointments are used in the less acute stages of discoid eczema.1 As with other types of eczema, there has traditionally been a role for rest and minimisation of stress. Sedating antihistamines also have a role in helping patients with severe pruritus to sleep at night.3
For widespread disease, alternative treatment therapies include narrowband UVB light therapy two to three times weekly, with duration titrated to treatment response.3 Systemic immunosuppressants and immunomodulators have been used as more last-line options for extensive disease.3 Dupilumab is an emerging treatment option for recalcitrant discoid eczema.17 Other last-line therapies include immunosuppressants such as ciclosporin, methotrexate, mycophenolate and azathioprine.18 Systemic corticosteroids should be avoided as they are associated with high rates of rebound disease.
Patients with the exudative subtype of discoid eczema may benefit from an oral antibiotic such as cefalexin, clarithromycin or a tetracycline. Secondary bacterial infections should be treated with topical or oral antistaphylococcal antibiotics depending on the size and distribution of the lesions, with further treatment based on bacterial swab results and local antibiotic resistance.3 Discoid eczema associated with alcohol misuse may be particularly predisposed to becoming secondarily infected, and such patients should be examined carefully to ensure infection has been properly treated.9
Referral to a dermatologist is appropriate if the disease does not respond to conservative skin care measures, bland emollients, topical corticosteroids and antibiotics. Referral can also be considered should the diagnosis be in question.
Prognosis
Discoid eczema is chronic, with partial remission during which plaques tend to clear in their centres. Relapse occurs at variable intervals, and is often worse in winter. With appropriate therapy and avoidance of skin irritants, discoid eczema may either clear within a year, or if not, will often persist for many years.2 As with other forms of eczema, some patients will experience postinflammatory dyspigmentation of the skin (hypo- or hyperpigmentation).3
Conclusion
Discoid eczema is a skin rash consisting of annular disc-shaped plaques typically affecting the trunk and lower limbs of adult male patients. It is sometimes associated with irritant (or allergic) contact eczema, chronic alcohol misuse, bacterial colonisation and certain medications. In most patients, discoid eczema can be controlled through general skin care measures of avoiding irritants and using regular emollients, intermittent topical corticosteroids and antibiotics as needed. MT
COMPETING INTERESTS: None.