Common skin problems in children. Managing atopic dermatitis


Atopic dermatitis is the most prevalent chronic skin disease seen in children, particularly before puberty. Accurate, family-focused advice from the GP is key to treatment success and maintaining remission.
- Atopic dermatitis (AD) is common and the range of severity large, ranging from trivial to life ruining.
- Diagnostic criteria for AD have been established.
- About 50% of patients with AD have an abnormality of filaggrin, an epidermal protein involved in the protective skin barrier.
- Itch, which results in sleep deprivation, can disrupt the lives of children with AD and significantly affect their families.
- Environmental modification is an essential part of management; however, house dust mite reduction measures are only effective among a subgroup of patients and are controversial.
- Topical therapy with emollients that restore the skin barrier is key.
- Topical corticosteroids are gold standard therapy.
- Corticosteroid phobia continues to be a significant barrier to effective treatment.
- Allergy testing is often requested by parents, but it does not change management in most cases and is probably carried out more than is necessary.
- When a child fails to respond to treatment, consider noncompliance, infection, allergy or combination with another dermatosis, most often psoriasis.
- The prognosis for AD is good, with most children recovering by the end of primary school.
Worldwide, atopic dermatitis (AD) is the most common condition seen in paediatric dermatology practice. The prevalence of atopy in the Australian population is about 20% and most patients with the condition are children.
AD is a genetic condition with complex genetic susceptibility moderated by environmental factors. Most affected children have a first-degree family member with an atopic condition, not necessarily dermatitis, and about 40% have a deficiency of the epidermal protein filaggrin, which is involved in the normal skin barrier. Additionally, atopic immune dysregulation related to the T-helper 2 (Th2) cytokine cluster can occur. Children with severe AD commonly have raised total immunoglobulin (Ig) E levels.
Various scoring methods are used to determine severity of AD, for instance the Eczema Area and Severity Index (EASI). These are most useful in a research setting. Assessing severity in a clinical setting can be done pragmatically, not only by noting the extent and clinical severity but also by assessing the impact on quality of life of the child, burden of treatment on the family and degree to which sleep is disturbed.
Clinical features
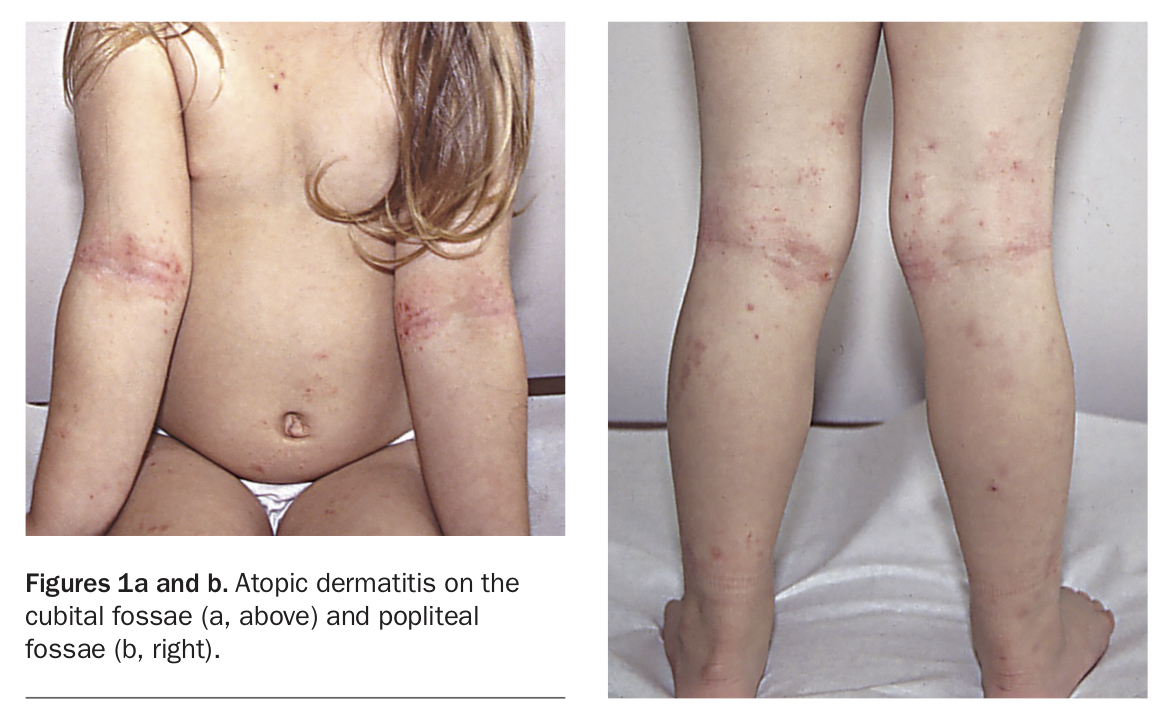
The onset of AD most often occurs in the first year of life between the ages of 3 and 12 months. Clinical criteria for AD established by Rajka and Hanifin and the UK Working party include three or more of itch, typical flexural distribution, patchy, excoriated erythema and personal history of atopy or atopy in a family member.1 Commonly there is also skin dryness. In children the rash is most often found on the face, cubital fossae and popliteal fossae (Figures 1a and b). The distribution and severity are highly variable, ranging from mild dryness and a minor rash on the arms and legs to total body involvement (Figure 2).
{kind=link}
{kind=link}
The itching of AD may be very disruptive, particularly during sleep. Severely affected children may wake up many times during the night, and parents often comment that the child’s sheets are streaked with blood from excoriations in the morning. Interestingly, small children often forget about the itchiness during waking hours until their clothes are removed, when they can literally go into a frenzy of scratching all over. Constant scratching often leads to areas of thickening of the skin. This is termed lichenification when it occurs in plaques and prurigo when it occurs in discrete nodules. Lichenification complicates AD, making it more challenging to treat.
Cutaneous infections
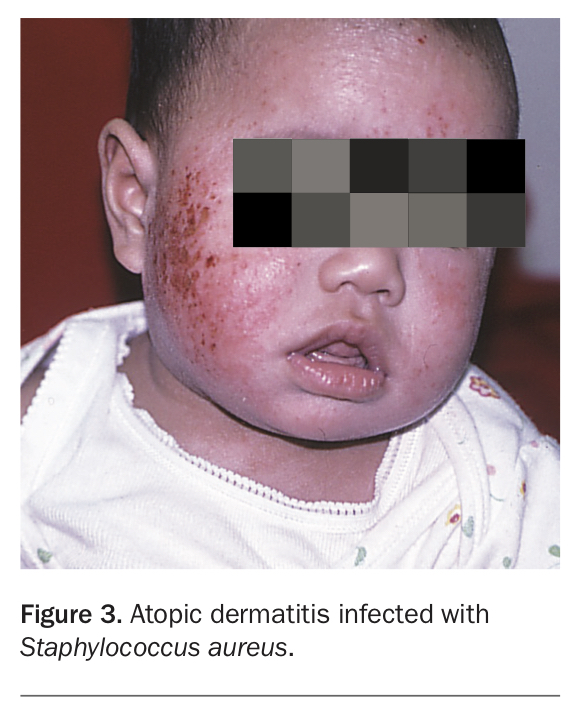
Cutaneous infections are very common, not only because of constant scratching and disruption of the epidermal barrier, but because of inherent immunological and cutaneous abnormalities in these patients that increase susceptibility. The most common bacterial pathogen is Staphylococcus aureus, which causes areas of weeping, crusting and folliculitis (Figure 3). Chronic S. aureus carriage exacerbates eczema and is a much more common cause of treatment resistance than allergy.
{kind=link}
In some cases, children with AD are also prone to relatively severe infections with herpes simplex virus. In contrast to most children, who may only ever suffer from stomatitis or herpes labialis, widespread or generalised infection with systemic upset may occur. Atopic children are probably not more prone than others to molluscum contagiosum, but the presence of this viral infection certainly exacerbates AD.
Environmental irritants and allergens
Children with AD are sensitive to environmental irritants and allergens, and this can include their topical therapy. It is well known that sand, wool, nylon, grass, soap and bubble bath cause irritation. Temperature changes and overheating are also problematic. Sometimes, even labels and rough seams in clothing can be a problem. Allergy to latex can be a little thought of trap for the unwary if caregivers are wearing gloves. It is common for these children to complain that their topical treatments sting and for their parents to comment that they cause erythema. This does not always indicate true allergy and may only be a problem when skin is excoriated and inflamed. The antiseptic triclosan in some bath oils can cause a cutaneous reaction that simulates a chemical burn. Although many patients with AD have raised IgE levels or positive skin prick test results to house dust mite, its role in causality and management is controversial and probably overvalued. Contact with grass and other airborne allergens such as animal danders, moulds and pollens can exacerbate AD.
Food allergy and intolerance
Food allergy, which is immunologically mediated, and food intolerance, caused by direct histamine release, are not common exacerbating factors in AD but they can be very relevant in some patients. It is common for parents to request allergy testing. Often they have good reason to do so, having observed their child’s reactions to certain foods – particularly cow’s and soy milk, peanuts, eggs, shellfish and high salicylate foods such as tomatoes and fresh fruits. However, misinformation on the internet leads many to believe that AD is an allergy in itself and to hold high hopes that if they can discover and eliminate the allergen(s) that a cure will result. This is rarely the case.
Dermatitis and psoriasis
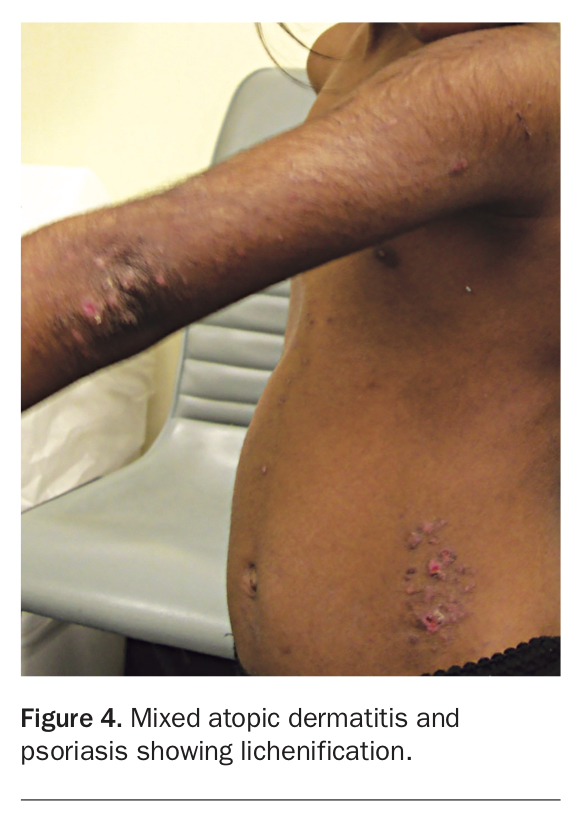
The coexistence of dermatitis and psoriasis is not uncommon when AD seems more difficult than usual to control or never completely responds to topical corticosteroids (Figure 4). Both are common skin conditions. Psoriasis in young children is much more subtle than that in adults, and the classic thickened plaques rarely occur. When AD and psoriasis occur together a clinical picture termed ‘psoriasiform dermatitis’ applies.2 These children have features of both; however, their condition is usually much more treatment resistant than children with AD only and requires specific psoriasis therapy.
{kind=link}
Parents should be asked about the family history, and signs of psoriasis in the child and parents looked for – for example, scaling of scalp and postauricular skin, or cracking under the earlobe and nail pits. Scaling, lichenification and papules on the dorsal surface of the knees and elbows in combination with dermatitis on the ventral surface is common and rarely looks like a typical psoriatic plaque seen in an adult.
Dermatitis and symptomatic dermographism
When children with apparently mild or well-suppressed eczema experience itch out of proportion to their clinical signs, they may have coexistent symptomatic dermographism. Dermographism is a form of chronic inducible urticaria. In this condition, histamine is easily released from mast cells in skin as a result of minor friction such as scratching or overheating. It can uncommonly be associated with allergy. Dermographism is easy to diagnose simply by firmly stroking the skin. This will result rapidly in a red wheal which takes 10 to 20 minutes to resolve (Figure 5). Although in general antihistamines are unhelpful in treating AD other than acting as night-time sedatives, they are useful in this subgroup.
{kind=link}
Psychological problems and other pressures
Psychological problems are more often seen in children who are severely affected with AD, and the impact on quality of life should never be underestimated. An Australian study has shown that severe AD is as impactful as other severe paediatric conditions such as diabetes and epilepsy.3
The most common problem is exhaustion from not sleeping well, leading to behavioural problems and poor concentration at school. However, the management of AD can come to dominate the child’s and parents’ lives, and it is common for any child with a chronic condition to become weary of the daily routine of treatment and to complain, fight, abscond and resist. Many parents are also exhausted, and, in the worst cases, outright rejection of the child by the parents may ensue.
Cost can also become a factor, as many of the required treatments, particularly emollients and bath oils, are not listed on the PBS. In addition, many parents are confused by conflicting information on the safety of treatments, particularly corticosteroids, and almost paralysed by the fear of long-term effects of treating their children.
Management
The management of children with AD is not simple, particularly in severe cases. The following factors need to be considered:
- compliance and counselling
- environmental modification
- control of skin dryness
- medical management of the dermatitis
- control of infection
- management of the dermatitis plus psoriasis combination
- in some cases, investigation and management of allergy.
Compliance and counselling
It cannot be stressed too strongly that AD is a chronic genetic condition. The patient’s parents or carers must understand the need for both continuous suppressive therapy at times of activity and ongoing preventive environmental modification in times of remission (see Practice Points and the Parent and Carer Handout). Further, they must understand that AD is rarely entirely caused by allergy and that management of allergy alone rarely delivers good outcomes. Treatment often fails because therapy is ceased as soon as the dermatitis clears, in the belief that a ‘cure’ has been achieved. When the inevitable relapse occurs, parents may then believe that treatment has been a failure and subsequently abandon further therapy.
{kind=link}
Treatment also often fails because parents are apprehensive about using topical corticosteroids. Parents need to be reassured that, when used correctly, topical corticosteroids have an excellent safety record. An Australian study has demonstrated that appropriate use of topical corticosteroids in mild to moderate eczema can maintain an EASI score of 0, without side effects.4 To encourage compliance, parents need education about the nature of AD, that it tends to become less severe with each passing year, the safety of the medication and the relative unimportance of allergy in aetiology and management.
It is often little things that make a big difference, such as:
- devising a simple regimen that fits in with the family lifestyle
- minimising cost with the use of authority prescriptions
- providing clear written instructions
- recommending that the parents talk to the child’s teachers about dust, sand and grass exposure at school. Small children are often expected to sit on the bare floor during school hours and are exposed to grass during sport and recess.
Regular follow up is always important to keep reassuring and reaffirming that parents are doing the right thing, modifying treatment according to response and complications, and praising positive results. There are so many negative influences on these families that it becomes imperative to keep repeating that of all the treatments available, by and large Western medicine still works best and is safe.
Environmental modification
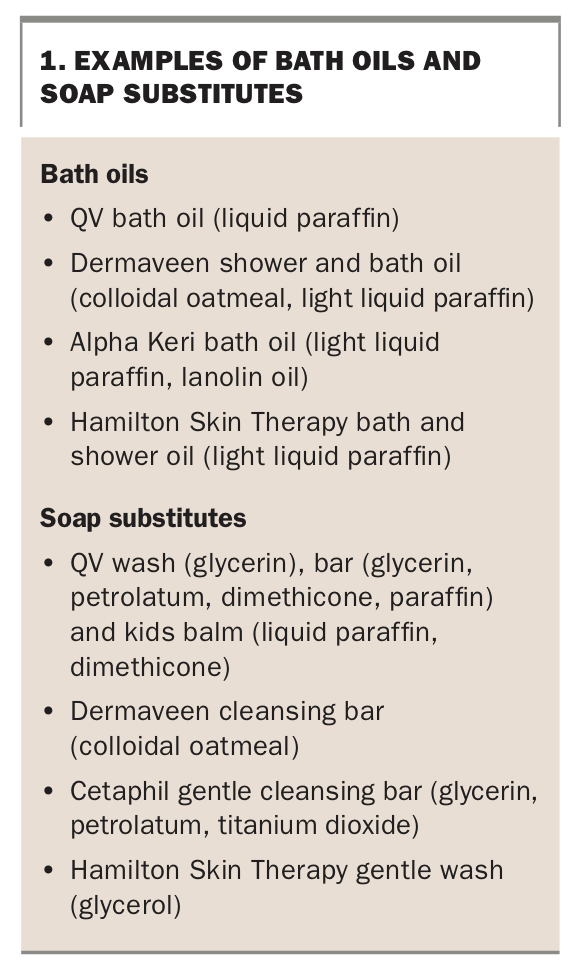
Environmental modification is an essential part of AD management, and one that parents readily accept, in theory at least. It is always important when telling parents what to take out of the child’s environment that you suggest what they should put in instead. Soap, shampoo and bubble bath do need to be eliminated. There are numerous soap substitutes that can be used (Box 1). Skin contact with woollen or acrylic clothes, blankets and toys should also be avoided, substituting pure cotton or at least 70% cotton blends.
{kind=link}
When dust and other aeroallergens such as animal dander, pollen, grasses and moulds are a genuine problem, children often have an accentuation of their rash in exposed areas such as the periocular area or the thighs where their skin contacts dust on the floor when sitting cross-legged at school. There is a history of exacerbation on exposure, and these children are more likely to have asthma and hayfever.5 Dust is difficult to minimise; however, using mattress and pillow covers, washing bedding and other fabric that comes in contact with the child’s skin in hot water, eliminating dust-catching objects (e.g. fluffy toys) and vacuuming thoroughly can help. If the child has to sit on the floor at school, a washable bathmat should be used. Before taking steps to reduce aeroallergens it is important to confirm with allergy testing that there genuinely is a very significant reaction present.
Many households, preschools and primary kindergartens have a sandpit. Sand is a major problem for children with AD. It is easy to get rid of the sandpit at home, but parents need to talk to carers about trying to keep the child out of sand elsewhere. Sand tends to accumulate in socks and shoes and is mostly a problem for hands and feet.
In summer, or year-round for the child who is swimming training, chlorinated pools can be a problem. It can be helpful to apply a greasy emollient before swimming and to shower and apply emollient immediately afterwards.
Control of skin dryness
Dispersible bath oil should be used daily in the bath. It is a common belief that baths should be taken infrequently and kept cool, but a normal daily bath helps to reduce bacteria and airborne allergens and irritants on skin without causing dryness as long as such an additive is used (Box 1).
After bathing, an emollient should be applied over the whole body. The frequency of use will depend on the child’s degree of skin dryness. For mild cases, application of emollient after bathing is sufficient. For more severe xerosis, application two or three times daily is often necessary. Emollients are easiest to apply when the skin is still damp after bathing.
Numerous emollients are available (Box 2), and the choice depends on the severity of the AD (greasier emollients are used for more severe xerosis), the climate (a less greasy product is needed in hot, humid weather) and personal preference. Cost can also be a factor and, as large amounts are required, compliance is more likely if this is minimised. Simple generic preparations, such as emulsifying ointment BP mixed with water, are as effective as proprietary compounds. Generally, greasier emollients available in tubs tend to be better moisturisers than thinner lotion preparations in pump packs. The adverse effects of some emollients can limit their use. The ubiquitous product sorbolene cream can cause stinging in some children that can lead to noncompliance and loss of confidence in treatment. It is helpful to keep samples of various emollients in the office for patients to try before purchase to determine if there is a problem. Useful over-the-counter emollient preparations include, for example, QV cream, Cetaphil moisturising cream, Dermaveen moisturising lotion, and Dermeze, Epaderm and DermaDrate products (the latter brand is useful for severe xerosis, but may sting).
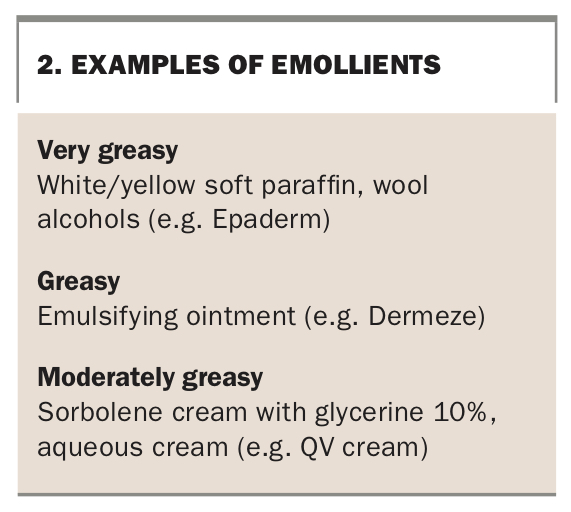{kind=link}
Medical management of dermatitis
Topical corticosteroids, which have been available for many years and for which we have long-term follow up information, remain the treatment of choice for mild to moderate AD. If used correctly, they are very safe and effective. Despite these facts, fear of their use is widespread in the community and is termed corticosteroid phobia. Social media have only added to the distrust of these medications and fear of corticosteroids is as prevalent and troubling now as it was 25 years ago.6 Thus it is important that doctors prescribing them are positive and reassuring about their usefulness. It is important to keep in mind that many other people, including the pharmacist, baby health nurse, naturopath, friends and relatives – all possibly more trusted by the patient than their doctor – may be denouncing them as dangerous.
The main fears with topical corticosteroids are that they will ‘thin the skin’ and ‘depress the immune system’. Both are theoretically true if potent preparations are overused or applied under plastic occlusion. However, when used as recommended below, this is highly unlikely.
Topical corticosteroids should be applied daily to any areas of active dermatitis, titrating the strength of the preparation and the frequency of application to the severity of the dermatitis. An emollient is applied to the entire skin before the corticosteroid is applied. Patients should have a range of topical preparations. If there is an inadequate response to a milder preparation after three days, a stronger one should be used.
Generally, the use of corticosteroids in children does not differ significantly from that in adults; however, the issues discussed in Box 3 are important to consider.
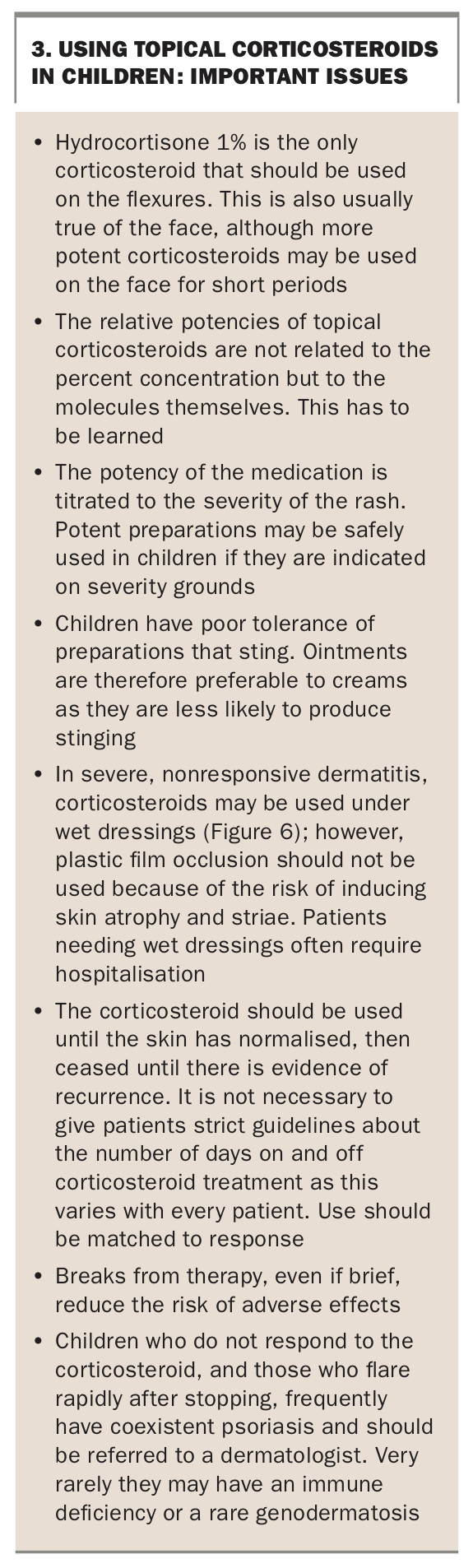{kind=link}
Other topical anti-inflammatory medications
There are two topical calcineurin inhibitors: pimecrolimus, which is available commercially as a 1% cream; and tacrolimus, which is available through compounding chemists as a 0.1% and 0.03% cream or ointment. Of the two preparations, tacrolimus is the more effective. These products are certainly no more effective, are more expensive and are much more likely to be irritating than topical corticosteroids. A recent meta-analysis has not shown that they are superior.7
Pimecrolimus has been evaluated in children and is indicated for the treatment of AD in children over 3 months of age. It is used twice daily. Its main advantage over topical corticosteroids is its lack of atrophogenic properties, particularly in thin skin such as the face in children who are unresponsive to mild corticosteroid preparations or who need to use them continuously.
Pimecrolimus is available on the PBS only with an authority prescription and only for the treatment of facial and periocular AD where there are contraindications to the use of topical corticosteroids. It is significantly more expensive than topical corticosteroids. Compared with topical corticosteroids, its very long-term safety is not as well known, although we have up to 20 years of follow up with calcineurin inhibitors so far. Because of the immunosuppressive properties of these agents, there has been concern that in the long term we may see skin cancer as a result of their use, particularly in sunny climates like Australia. It is wise, therefore, to use a sunscreen on exposed skin being treated. Only time will tell how safe the use of these compounds on young children really is.
Parents of children with AD are sometimes keen to avoid the use of topical corticosteroids by substituting pimecrolimus. Most do not realise that it is an immunosuppressant with its own hazards.
Another new anti-inflammatory product is the topical phosphodiesterase-4 inhibitor crisaborole. It is indicated only for mild to moderate AD, is not PBS listed and is significantly more expensive than topical corticosteroids. Its role in treatment is similar to the calcineurin inhibitors and it may well appeal to parents with exaggerated fears of topical corticosteroids.
Oral immunosuppressive therapy
Most children with AD can be very successfully managed with topical therapy. However, for very severely affected children systemic immunosuppression is required. Any child for whom topical corticosteroids are needed in such large amounts that there could be a genuine chance of side effects is a candidate for such treatment.
Oral corticosteroids are contraindicated because severe rebound is usually experienced on withdrawal, and repeated courses destabilise the dermatitis and can result in erythroderma. This situation is completely different from treating acute exacerbations of asthma.
Oral ciclosporin may be initiated by a dermatologist or clinical immunologist for the treatment of very severe AD in children. Treatment must be very carefully monitored, and this means numerous blood tests and blood pressure readings for the child. This is a huge step for most parents, although certainly it can be sanity-saving in children with severe, life-disrupting AD. It is used when all conservative measures have failed to control the dermatitis and the patient’s quality of life is severely affected.
Other medications that may be used in children include azathioprine and methotrexate, which is particularly useful when there is coexisting psoriasis. Newer systemic biologic agents that will become available in future include the injectable interleukin (IL)-4/IL-13 receptor inhibitor dupilumab and the Janus kinase (JAK) inhibitors, which are oral medications. Both can be highly effective and are relatively low in side effects.
Control of infection
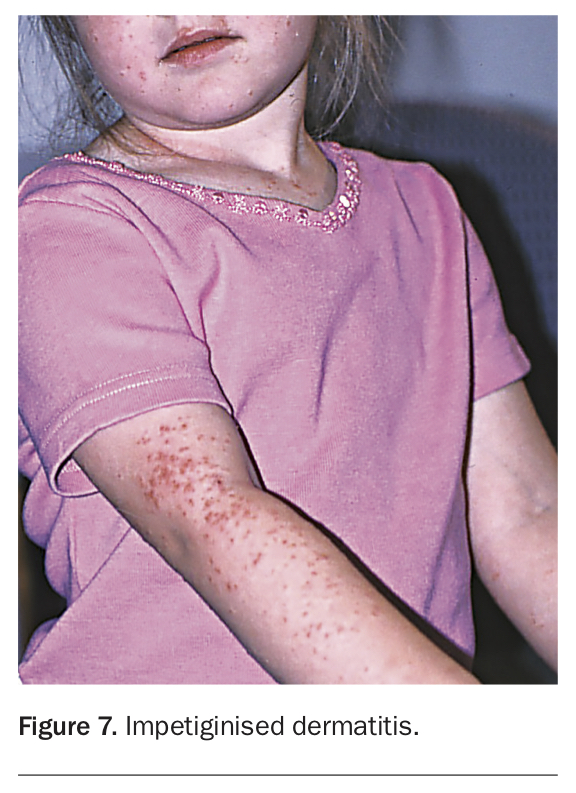
The most common infections seen in children with AD are:
- impetigo (Figure 7) – most often due to S. aureus; occasionally due to a mixed infection of S. aureus and Streptococcus pyogenes, or S. pyogenes alone
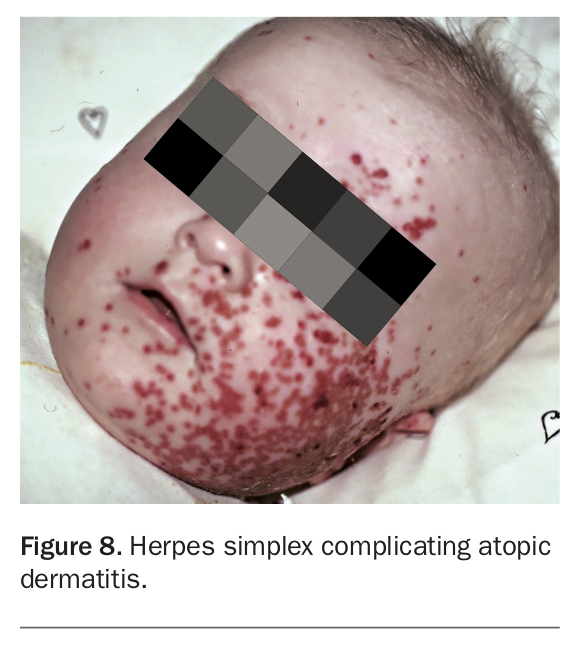
- herpes simplex (Figure 8)
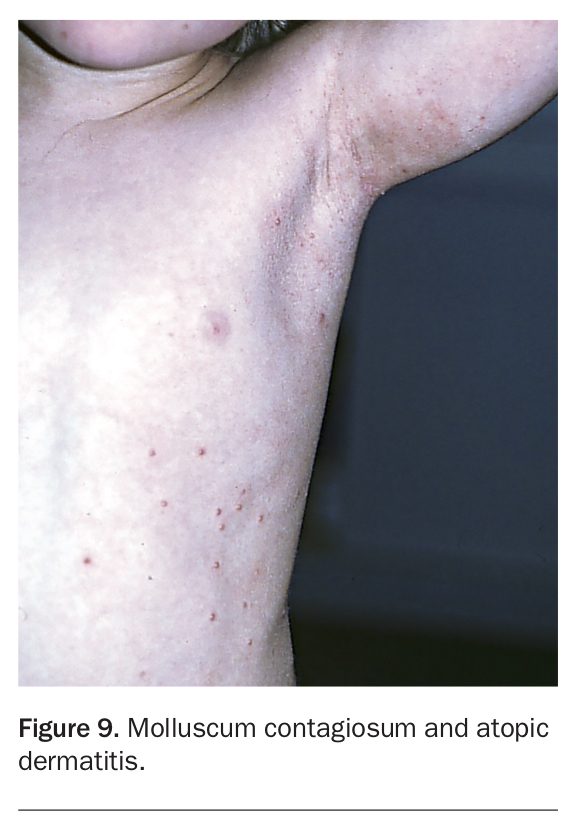
- molluscum contagiosum (Figure 9).
{kind=link}
{kind=link}
{kind=link}
Any of the above infections often exacerbate AD, and control of infection is essential before the dermatitis can be treated effectively. A bacterial swab of involved skin is a useful, inexpensive test that confirms infection and determines antibiotic sensitivities. Community acquired methicillin-resistant S. aureus is becoming more common and often requires treatment with clindamycin. If herpes simplex is suspected clinically by the presence of grouped vesicles or erosions, viral swabs should be taken. This is always an acute, and sometimes also recurrent, event. When the infection is widespread, treatment with aciclovir or valaciclovir is needed and specialist referral recommended.
Molluscum contagiosum infection, although by no means confined to children with dermatitis, does often make the dermatitis refractory to treatment. The best way to eradicate the lesions is to remove them physically; however, this is often easier said than done. It can be difficult to change the course of the infection and one may have to accept that until the lesions resolve spontaneously, more aggressive treatment of the dermatitis may be necessary.
In many cases, the child’s skin is chronically colonised by S. aureus. This can result in exacerbation of the dermatitis, difficulty in controlling it, and crusting and folliculitis. When any of these are encountered, cutaneous and nasal bacterial swabs should be taken to confirm the infection and determine the sensitivities of the S. aureus. This situation requires more than one course, and at times repeated courses, of oral antibiotics. Adding bleach to the bath water has been shown to be very effective in controlling chronic bacterial skin infection.8 A topical antibiotic such as mupirocin 2% ointment should be kept on hand to apply to crusted areas twice daily for a week. It is more effective if the crusts are removed by soaking under a wet cloth or in the bath. If nasal carriage is detected, mupirocin 2% nasal ointment should also be used twice daily for seven days.
Dicloxacillin or flucloxacillin are the treatments of choice for obvious secondary infection, but cefalexin or roxithromycin are useful for patients who are allergic to penicillin. Many strains of S. aureus are resistant to erythromycin. In some children in whom chronic infection makes AD impossible to control, long-term oral antibiotic treatment may be useful. However, before embarking on this, specialist referral is recommended.
Treating the dermatitis/psoriasis combination
Patients with a combination of dermatitis and psoriasis need treatment for both conditions. Therefore, in addition to the usual management of AD, tar creams and shampoos or topical calcipotriol may be needed. It is important that the parent understands which areas of the rash are AD and which are psoriasis. Managing this situation can be difficult, and referral to a dermatologist is recommended; this often happens anyway because the ‘dermatitis’ does not respond to treatment.
Investigation and management of allergy
Most parents of children with AD want to know why they have it, and the answer, ‘It’s genetic’, is not enough. As a result, many will request allergy testing. The thought that they may find a substance that if avoided will end the problem is very attractive and also gives them something tangible that they can control without the use of drugs. Further, parents who think their child has an inherited health problem often feel unnecessarily guilty and one response to this is denial of the diagnosis.
In an ideal world, a child should be considered for allergy assessment if:
- the dermatitis is severe or difficult to control
- parents report exacerbations in relation to particular foods or infant formula
- there is an urticarial component
- the distribution is on exposed areas, particularly the periocular area or other parts of the face, indicating the role of an aeroallergen such as house dust mite.
In practice, however, many unnecessary allergy tests are conducted because of parental pressure, and children are sometimes put on very restrictive diets on thin evidence. Parents may also embark on expensive measures such as pulling up carpets and removing all the curtains, only to find that these make little difference. Allergy testing may be carried out by either skin prick testing (SPT) atopic patch testing (APT) or radioallergosorbent testing (RAST). The latter is a blood test and is readily available for a wide range of allergens. Allergy testing has many pitfalls, and results need to be considered in conjunction with the clinical presentation. Not all food reactions are detectable with these tests, particularly when salicylates and other food additives are involved. Referral is strongly recommended before any major action, either dietary or environmental, is put into practice.
Prognosis
Generally, the prognosis of AD is good, with most children substantially improving by the time they start school and remitting by the end of primary school. A minority still suffer from the condition as teenagers, but it continues into adult life in only a few. Treatment resistance is often due to noncompliance, but infection, allergy or the onset of a new skin condition such as psoriasis should be considered.
Certain environmental situations may bring out the tendency for AD later - for example, an occupation or hobby where there is heavy aeroallergen or irritant exposure, or an outdoor sport in a patient who is allergic to grass. Certain geographical areas suit some patients better than others, no doubt related to humidity and aeroallergen levels.
Until remission occurs, parents need to maintain all environmental modification precautions and ensure treatment is given regularly. It is important in young children, and even in many teenagers, never to leave treatment up to the child. It is a bit like teeth cleaning: unless the parent nags, it often does not happen.
Conclusion
AD is a common paediatric presentation in primary care and GPs maintain key long-term relationships with both the child and their parent or carer. Educating parents and carers about the safety of gold standard therapy and the importance of day-to-day skin maintenance measures and environmental modifications is central to treatment success and maintaining remission. The GP’s assistance in negotiating many of the associated considerations, such as minimising the cost of treatment and suggesting simple solutions for when the child is at school, make the world of difference to the wellbeing of children with AD. MT