Rosacea: a thorny problem with a rosy outlook

Rosacea is a common and often underdiagnosed chronic inflammatory centrofacial dermatosis, with a diverse clinical presentation. Symptoms can have profound impacts on the social and psychological wellbeing of affected patients. Optimising management requires an accurate diagnosis and tailored treatment to the presenting features of the individual patient.
- Rosacea is a common and often underdiagnosed inflammatory centrofacial dermatosis.
- Rosacea has a diverse clinical spectrum and includes symptoms of flushing, erythema, papules, pustules and, for some, skin thickening or ocular symptoms.
- Rosacea can have a profound impact on the social and psychological wellbeing of those affected.
- Early recognition and treatment can improve quality of life.
- Treatment options are diverse and should be tailored to the individual.
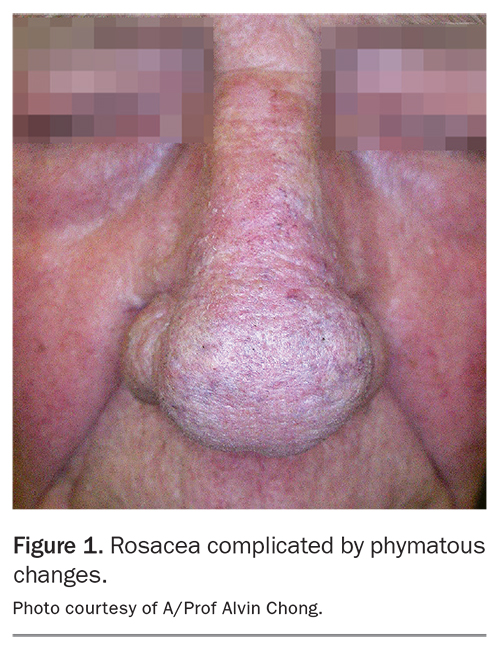
Rosacea is an often underdiagnosed chronic inflammatory centrofacial dermatosis.1 It is diverse in its clinical presentation and is characterised by exacerbations and remissions.2 Symptoms and signs encompass flushing, erythema, papules and pustules. Ocular involvement can occur in up to 50% of patients with rosacea and symptoms can be nonspecific.3 Phymas or enlargement and thickening of the facial skin, particularly the nose in men, is a diagnostic feature of rosacea (Figure 1).4 Initially, symptoms and signs may be transient, but persistent erythema with telangiectasia can develop over time due to repeated vasodilation.5
{kind=link}
Rosacea is estimated to affect up to 5.5% of the global population.6 It can occur in all skin types; however, it predominantly affects people with fair skin, especially those of Celtic heritage.7 Men and women are both affected, although women have a slightly higher prevalence and men develop phymatous changes more frequently.8,9 Typically, symptoms will peak from 30 to 50 years of age.10
Rosacea symptoms are often distressing and can have profound impacts on the social and psychological wellbeing of affected patients. People with rosacea have increased levels of embarrassment, social anxiety and depression and a decreased quality of life.1 Appropriate treatment of symptoms and signs of rosacea results in an improved quality of life for affected patients.1
Pathophysiology
The pathophysiology of rosacea is yet to be fully elucidated but is known to be influenced by genetics and neurovascular dysregulation, in association with an abnormal cascading innate and adaptive immune response.7,9
Flushing and erythema develop from increased vascular reactivity, which contributes to increased blood vessel density near the skin surface.11 Endogenous and exogenous triggers activate primary proinflammatory cytokines resulting in inflammation, which induces the characteristic histopathological features of rosacea. These triggers include sun exposure, heat and noxious cold, spicy food, smoking, exercise and alcohol.12 Microbes such as the Demodex mite are thought to be an additional trigger for this inflammatory cascade.13 In women during menopause, hot flashes may also trigger rosacea flares. Exposure to increased sunlight in the summertime may be a trigger for some people, whereas for others winter months will trigger symptoms through temperature fluctuations, cold temperature, icy winds and dry heat through heating systems.
Investigations
Rosacea is a clinical diagnosis and, as such, there are no histological or serological markers. Histology, patch testing and serology should be considered for cases if there is diagnostic uncertainty, such as the need to exclude allergic contact dermatitis or lupus erythematosus.
Diagnosis
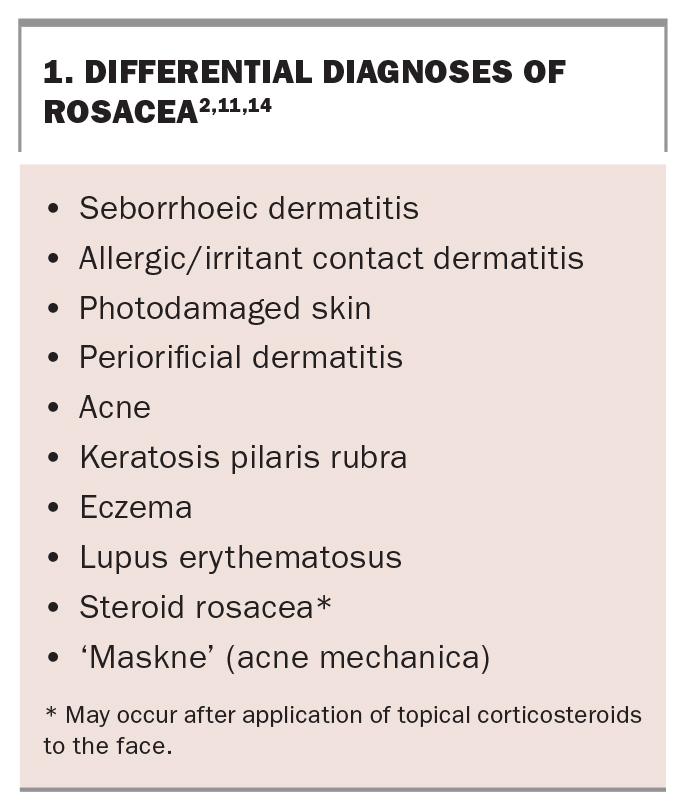
Erythematous facial dermatoses can pose significant diagnostic challenges. Differential diagnoses that need to be considered are outlined in Box 1.2,11,14 It is important to remember that rosacea can coexist with other conditions (e.g. rosacea and photodamage or rosacea and perioral dermatitis) so it is possible to have more than one condition contributing to the presenting features.
{kind=link}
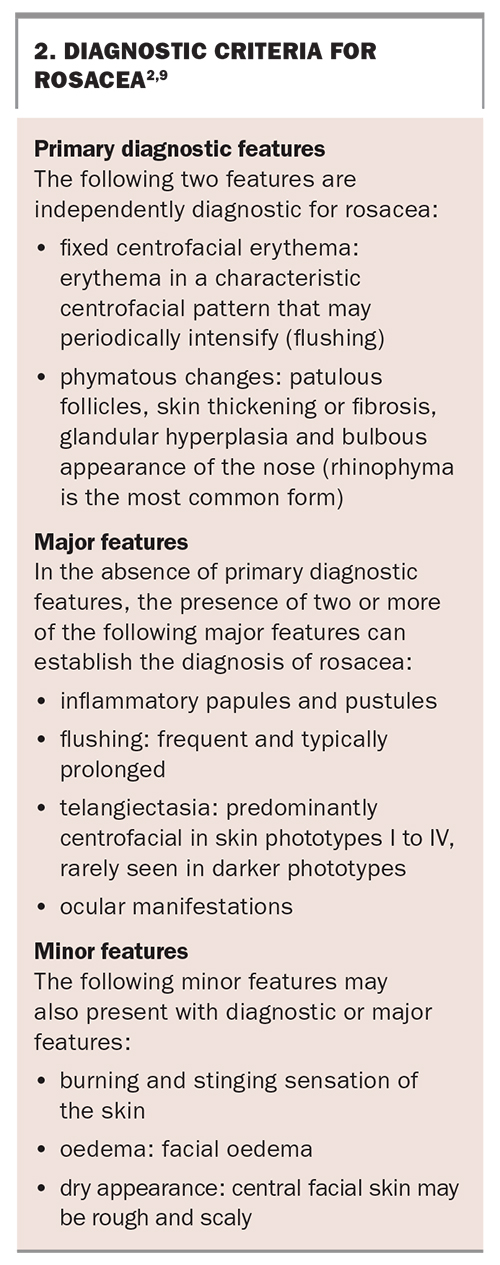
Rosacea was previously classified into four subtypes (erythematotelangiectatic, papulopustular, phymatous, ocular) with one variant (granulomatous). In recent years, our understanding of rosacea has evolved. A new classification system has been developed based on diagnostic criteria, including major and minor features (Box 2).9 The primary diagnostic features, which are independently diagnostic for rosacea, focus on persistent centrofacial erythema with periods of increased intensity and phymatous changes. In the absence of diagnostic features, a diagnosis of rosacea can be made if there are at least two major features, encompassing flushing (transient erythema), inflammatory papules and pustules, centrofacial telangiectasia and ocular manifestations. Minor features might also present with diagnostic or major features and encompass burning, stinging, oedema or dry sensation of the skin.2
{kind=link}
Ocular symptoms are common and may include burning, itching, watering, grittiness, photosensitivity, lid margin or conjunctival erythema with or without recurrent stye and chalazion formation.
Comorbidities
Rosacea can often occur with other dermatological conditions, including extrinsic photoaging, telangiectasias, seborrhoeic dermatitis, acne, irritant contact dermatitis and keratosis pilaris. More recently, it has often been associated with ‘maskne’, or acne mechanica, from mask wearing in the context of the pandemic.14 Maskne can be differentiated from rosacea as it will usually onset within six weeks of starting regular facial mask wear and will typically be distributed over the lower half of the face (underneath where the mask is worn). Maskne, unlike rosacea, will also typically present with comedones.15
There is also emerging evidence linking rosacea with other organ systems and comorbidities. Comorbidities include gastrointestinal, cardiovascular, respiratory and neurological disorders. Associations have also been found with several autoimmune diseases such as coeliac disease, rheumatoid arthritis, multiple sclerosis and diabetes mellitus.16
Treatment
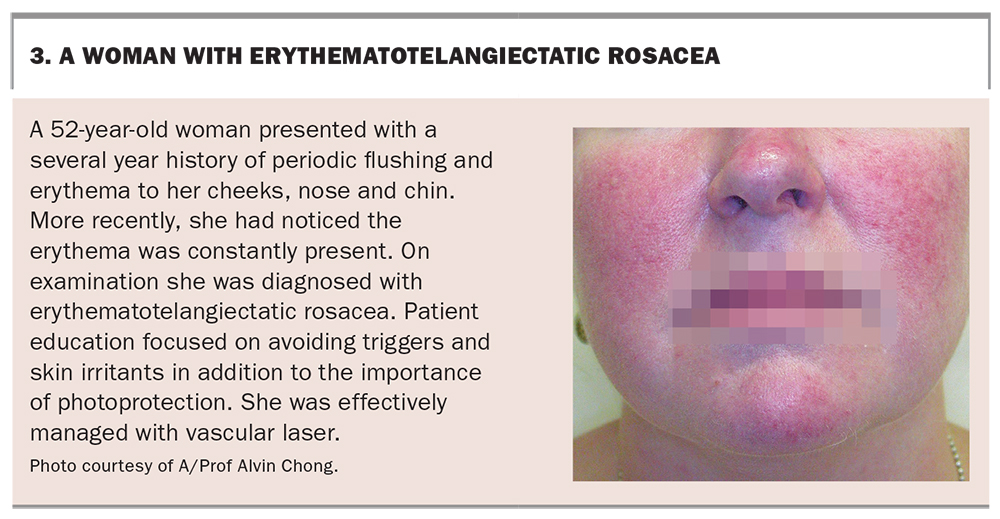
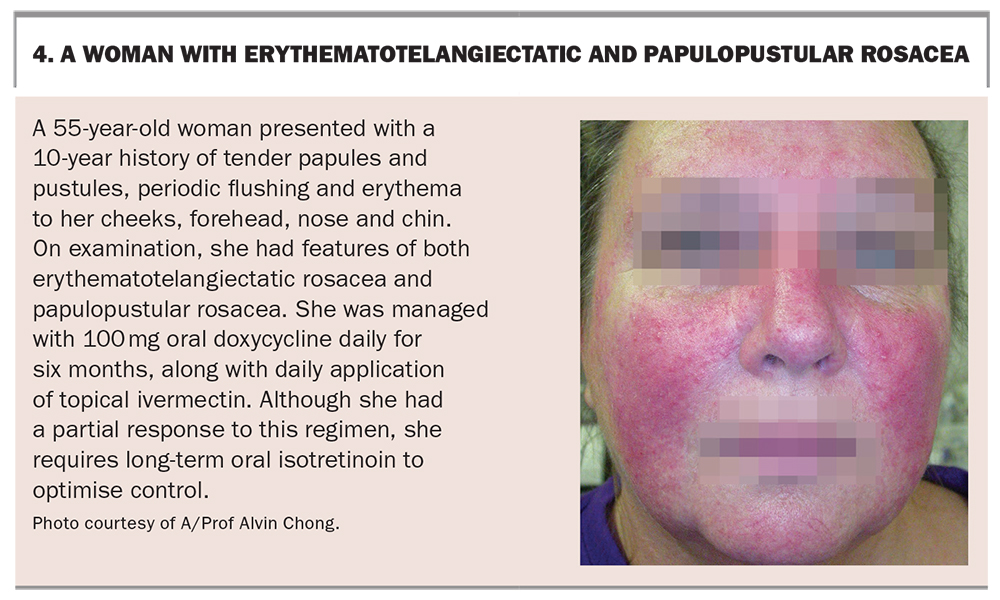
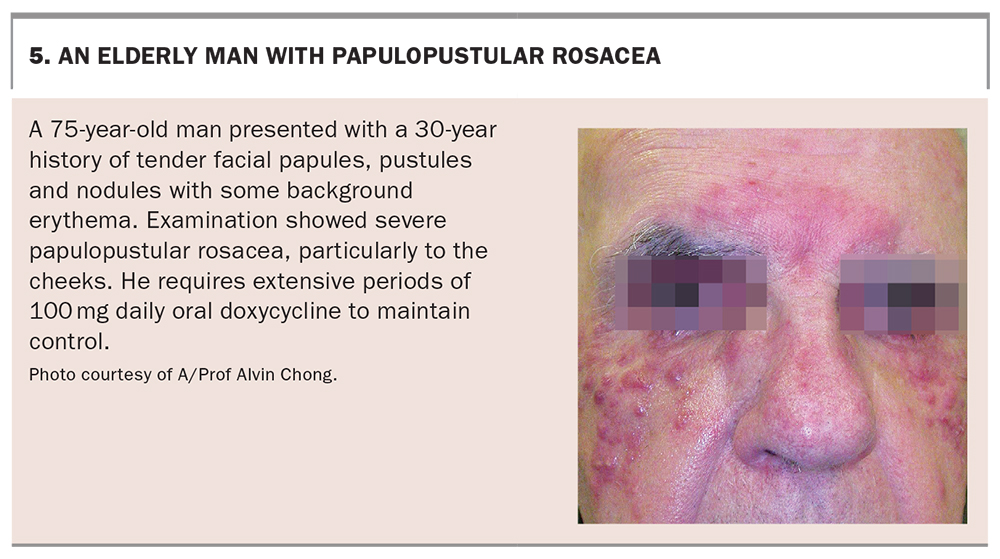
Treatments should be tailored to the presenting features of the individual and the degree of distress caused by the condition (see the case studies in Box 3, Box 4 and Box 5). Optimising treatment begins with appropriate patient education. Education should highlight that rosacea is a treatable but not curable condition. Although the exact aetiology is unknown, it is caused by a combination of an overactive immune system, alongside heredity and environmental factors. Education should also emphasise the important role of reducing irritation through photoprotection and gentle skin cleansing as well as the avoidance of exacerbating factors and triggers.5
{kind=link}
{kind=link}
{kind=link}
Skin care is important to maintain the epidermal barrier but ideally the cleansing and moisturising routine will be simple and contain a soap-free cleanser.17 Scrubs and abrasive cleansers should be avoided, along with alpha and beta hydroxy acids such as salicylic or glycolic acid. Cosmetic products should be free from fragrance, colours and essential oils.18 Patients should also be advised to avoid touching the face when possible throughout the day.19
Finding evidence-based and reliable patient information can be challenging, especially with the rise of social media. Although there is no Australian rosacea society, patients may find the US National Rosacea Society (rosacea.org) helpful for further information.
Topical agents
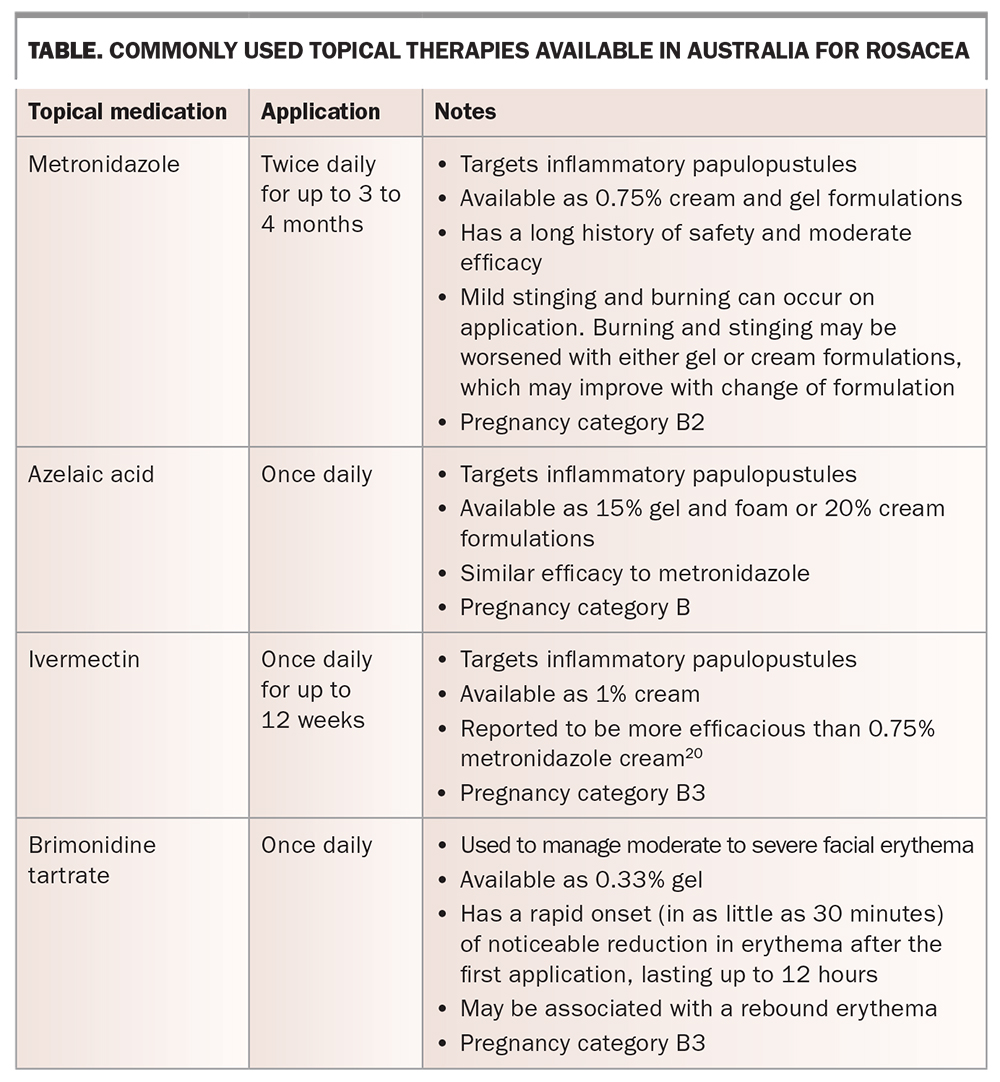
Topical agents are first-line therapy for the treatment of mild to moderate rosacea. They are typically used for their anti-inflammatory effects (such as metronidazole, ivermectin or azelaic acid) or their vasoconstrictive effects (such as brimonidine). Commonly used topical agents are outlined in the Table.20 Typically, patients are reviewed after six weeks on topical treatment to assess for response.
{kind=link}
Systemic agents
Oral antibiotics play a key role in the management of moderate to severe rosacea. Tetracyclines, such as doxycycline and minocycline, have been the long-term mainstay of papulopustular rosacea, but also have efficacy in ocular rosacea. The primary mode of action is anti-inflammatory. Typically, a patient is started on 50 to 100 mg doxycycline or 50 to 100 mg minocycline daily for six to eight weeks and then reviewed, with a view to ongoing treatment. If a patient fails to respond to doxycycline then referral to a dermatologist should be considered. Patients should not take doxycycline for longer than six months at a time. Additionally, if they respond but papules and pustules rebound on cessation, requiring repeat courses, then referral to a dermatologist is also required. Adverse reactions of doxycycline may include photosensitivity, candida vaginitis and oesophagitis.11 Treatment with minocycline should be limited to six months or less, due to the risks of iatrogenic hepatitis, drug-induced systemic lupus erythematosus and skin pigmentation changes. Erythromycin, although not always as effective, may also be trialled and has the benefit of being safe for use in pregnancy and breastfeeding.21
Off-label, low-dose oral isotretinoin, as prescribed by dermatologists, has good evidence of efficacy in people with rosacea, and has particular efficacy in the treatment of papulopustular rosacea variants.22 ,23 Isotretinoin is thought to act through its downregulation of local cutaneous immunity, but its effect on lipid metabolism may also play a role.5
Laser and light devices
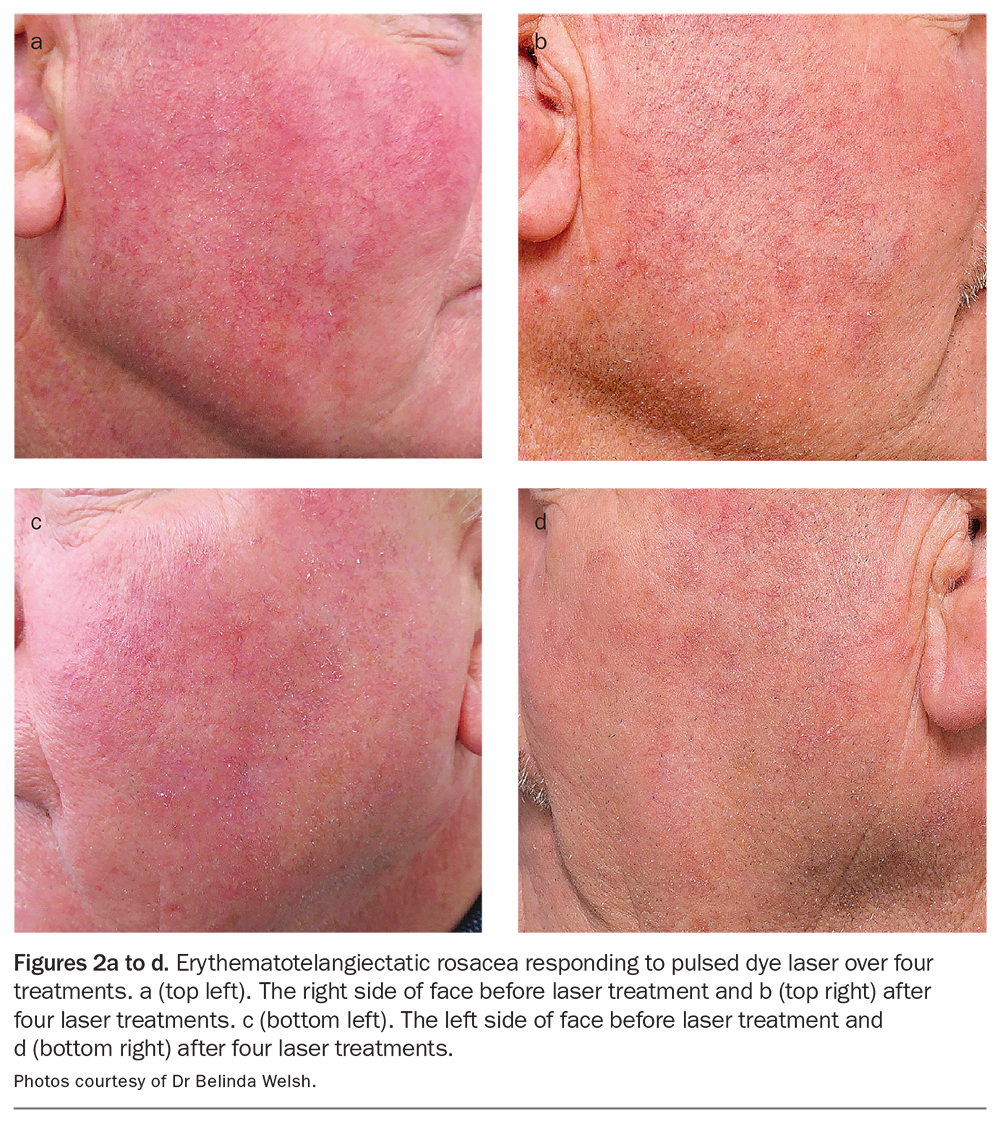
Laser and light devices are particularly valuable in the treatment of rosacea-associated erythema and telangiectasia. They can also remodel and rebuild dermal collagen, assisting in improving overall skin quality. Numerous different laser and light therapies are available, including pulsed dye laser (Figure 2), potassium titanyl phosphate laser, long-pulsedneodymium-yttrium-aluminium garnet laser, intense pulsed light and nonablative and ablative lasers. The choice of laser or light devices should be tailored to the specific presentation of the patient.
{kind=link}
Management of specific features
Specific presentations of rosacea may require tailored management. Phymatous changes can be managed through oral isotretinoin, fully ablative carbon dioxide laser resurfacing or surgical excision.24
First-line therapies for ocular rosacea are eye hygiene measures and artificial tears. Often, patients will also benefit from use of systemic antibiotics such as tetracyclines. Early referral for ophthalmological care should be considered for moderate to severe cases.24
Treatment options for problematic flushing include beta-adrenergic blockers, such as propranolol or carvedilol. Monitoring for side effects such as bronchospasm, bradycardia and hypotension is important. Alpha-adrenergic receptor agonists, such as clonidine, may also be used but may be associated with systemic side effects.5 Recently described emerging treatments include off-label use of botulinum toxin.25
Conclusion
Rosacea is an extremely common chronic centrofacial dermatosis with diagnostic features of erythema and flushing and tissue fibrosis (phymas). Its impact on the psychological wellbeing of patients should not be underestimated. Although our understanding of the pathophysiology of rosacea remains incomplete, current management strategies are very successful in controlling the signs and symptoms. Optimising management requires accurate diagnosis and tailored treatment to the unique circumstances of each patient and their presenting features. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.