Nodular basal cell carcinoma
The diagnosis of skin lesions is a daily challenge in general practice. Dermoscopy can provide extra clues, as illustrated in this vignette.
Case presentation
A 70-year-old retired man presented for review of a lesion on his face, which had been enlarging in size over a period of three months and intermittently bleeding. He was otherwise well.
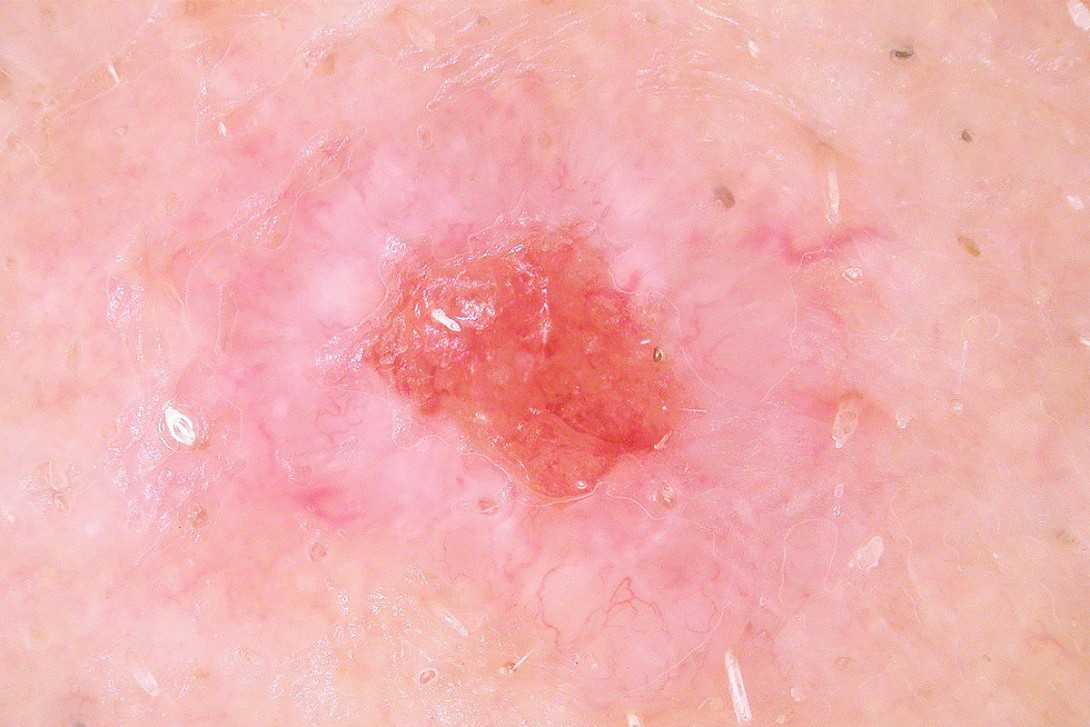
A careful patient history was taken as part of the skin lesion assessment (Box). On clinical examination, a 6-mm ulcerated papule with focal bleeding was identified on the left upper cutaneous lip, near the oral commissure (Figure 1). Dermoscopic examination demonstrated a central ulceration that was surrounded by a milky-pink area (Figures 2a and b). Prominent arborising telangiectatic vessels were observed.



A 3-mm punch biopsy was performed to further characterise the lesion.
Diagnosis
A diagnosis of a nodular basal cell carcinoma (BCC) was made on the basis of clinical and dermoscopic assessment and confirmed by histopathology.
Differential diagnoses
Important differential diagnoses in this case included squamous cell carcinoma, in situ squamous cell carcinoma (Bowen’s disease), amelanocytic melanoma and traumatised actinic keratosis.
Discussion
Dermoscopy was useful in evaluating this lesion, revealing key features of a nodular BCC:
- arborising telangiectasia (distinct branching serpentine vessels) – the hallmark feature
- central ulceration
- milky-pink colour.
There are other dermoscopic features (not seen in this lesion) that can be helpful for diagnosing a nodular BCC. These include bright white areas, which may represent the superficial stromal component of a BCC, often seen centrally or peripherally in the lesion. Pigmentation may be present in nodular BCCs, appearing as large blue-grey ovoid nests or peppering, representing aggregates of tumour cells. Shiny white and yellowish structureless areas may be visualised due to the presence of mucin or collagen. Slight hyperkeratosis or scaling may be present.
Management
Standard surgical excision with clear margins is the mainstay of treatment for nodular BCC.
Key points
- A nonhealing lesion that tends to bleed should raise suspicion of a nodular BCC.
- Dermoscopy can aid diagnosis. The presence of arborising telangiectasia is the hallmark feature of a nodular BCC.
- Histopathology can confirm a diagnosis of BCC and also be useful for guiding treatment options, particularly for cosmetically sensitive areas such as the face. MT
COMPETING INTERESTS: None.
Further reading
1. Pan Y, Chamberlain AJ, Bailey M, Chong AH, Haskett M, Kelly JW. Dermatoscopy aids in the diagnosis of the solitary red scaly patch or plaque –features distinguishing superficial basal cell carcinoma, intraepidermal carcinoma, and psoriasis. J Am Acad Dermatol 2008; 59: 268-274.
2. Reiter O, Mimouni I, Dusza S, Halpern AC, Leshem YA, Marghoob AA. Dermoscopic features of basal cell carcinoma and its subtypes: a systematic review. J Am Acad Dermatol 2021; 85: 653-664.
3. Samarasinghe V, Madan V, Lear JT. Focus on basal cell carcinoma. J Skin Cancer 2011; 2011: 328615.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.