An update on combined hormonal contraceptive pills

Women's health
Latest developments in combined oral contraceptives (COCs) offer women more choice. Extended-cycle regimens are available and some COCs have non-contraceptive uses.
Although women in Australia are following the international trend of increasingly choosing more effective long-acting reversible contraception, combined oral contraceptives (COCs) continue to be used by about 33% of women.1 Clinicians should therefore be aware of the latest developments in COCs.
The earliest COCs contained the synthetic oestrogen ethinyl oestradiol (EE) or its prodrug mestranol combined with either of the progestogens levonorgestrel (LNG) or norethisterone (NET). They had high hormonal doses, high risks and troublesome side effects. Reduced dosages and new hormonal constituents and regimens have enhanced the safety and side effect profile of COCs and provided additional non-contraceptive benefits for conditions such as acne and heavy menstrual bleeding.2,3
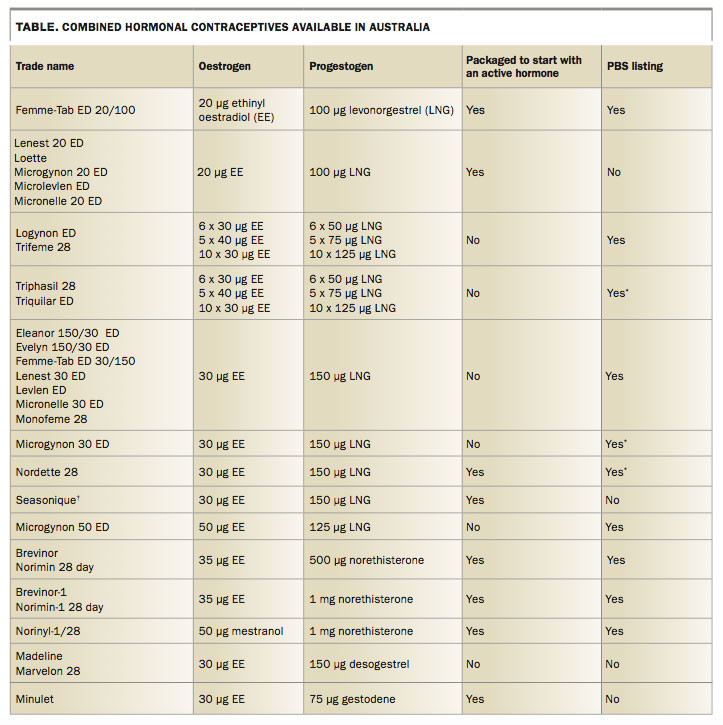
This article provides guidance to currently available COCs for medically-eligible women who do not have contraindications to oestrogen.4 The table provides a summary of COC formulations and brands. All COCs containing NET and most containing LNG are listed on the PBS, whereas others are non-PBS listed.
First-line COC choice
A monophasic PBS-listed LNG pill containing 30 μg EE or less is a good first choice of COC. As well as being relatively cost-effective, COCs containing LNG appear to have the lowest risk of venous disease, with those containing 20 μg of EE being associated with a lower risk of venous and arterial disease than those with 30 μg EE.5
Pills with lower EE doses
Early pills contained the equivalent of 100 to 150 μg EE. However, this dose has been reduced to as low as 20 μg EE in newer pills in Australia, usually in combination with 100 µg LNG or 3 mg drospirenone.
Multiple brands of pills with the lowest EE dose are available but only one is listed on the PBS: the COC containing 20 μg EE and 100 μg LNG (Femme-Tab 20). Pills with 20 μg EE are likely to have fewer hormonally-related side effects such as headaches or mood swings than those with 35 or 30 μg EE, although trials comparing pill types are lacking.
A recent French national database study reported a statistically significant lower risk of pulmonary embolism, ischaemic stroke and myocardial infarction (MI) in women taking LNG-containing COCs with 20 μg EE rather than those containing 30 to 40 μg EE.5 It is uncertain whether the pill containing 20 μg EE and 3 mg drospirenone is associated with a lower risk of venous thromboembolism (VTE) compared with pills containing 30 μg EE and 3 mg drospirenone.6 The absolute risk of these serious conditions is, however, very low for women without additional vascular risk factors. The lower risk of vascular diseases with the lower EE-dose COCs has to be balanced against a higher chance of breakthrough bleeding, which can lead to early discontinuation of the COC.7 Note that there is no place for pills with 50 μg EE in the management of women with breakthrough bleeding. These pills are also unsuitable for women taking concurrent liver enzyme-inducing medication because they contain insufficient progestogen. Combinations of lower-dose pills making up at least a total of 50 μg EE can be used for women taking concurrent liver enzyme-inducing medication who prefer not to switch to another method.
Pills with oestradiol or oestradiol valerate in place of EE
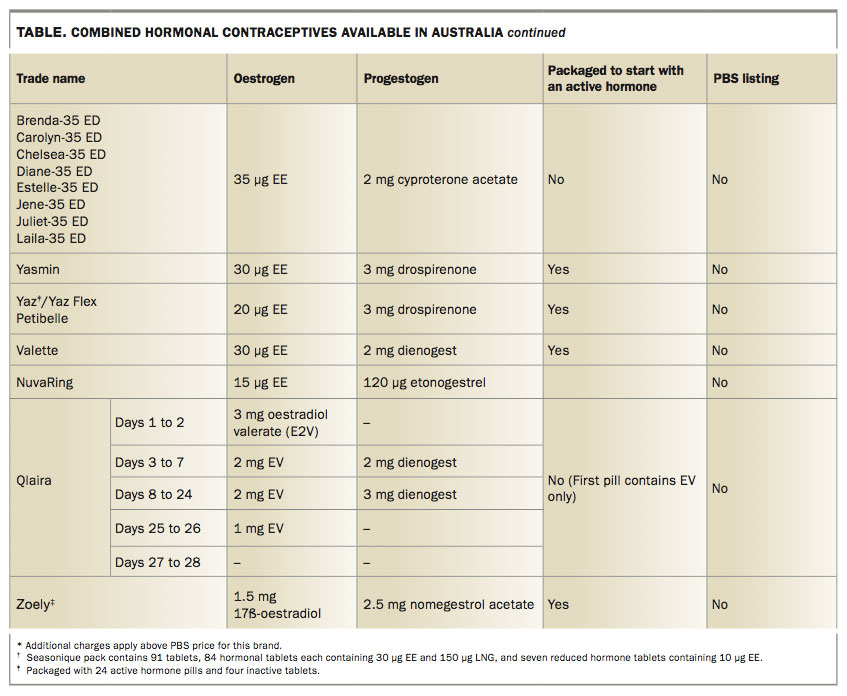
Since 2010 COCs containing 17β-oestradiol (E2; Zoely) or its prodrug oestradiol valerate (EV; Qlaira) instead of EE have been available. E2 and EV are sometimes referred to as ‘body identical’ hormones because they are structurally identical to oestradiol produced by the ovaries. Given that the major risks of COCs relate to the effect of EE on liver metabolism, in particular on coagulation factors and glucose metabolism, this development offers potential safety benefits and may be a useful choice for perimenopausal and other medically eligible women with raised background risks of arterial and venous disease. Studies have shown that pills containing E2, and to a lesser extent those containing EV, have a reduced effect on lipid and carbohydrate metabolism, haemostatic parameters and markers of endocrine function,8 but evidence for an effect on VTE, MI and ischaemic stroke is not yet available.
These COCs are a useful alternative choice for some women, but are not available on the PBS. Both are associated with a moderately high rate of amenorrhoea9,10 and the pill containing EV has been shown to be associated with fewer oestrogen withdrawal symptoms than a traditional pill with a seven-day hormone break.11,12
Pills with a shortened or absent hormone-free break (extended-cycle regimens)
The benefits of reducing or eliminating the seven-day hormone-free break are now well established.11,12 Two COCs have been formulated with 24 hormone pills and four inactive pills (the COC containing 20 μg EE and 3 mg drospirenone [Yaz] and the COC containing E2 and nomegestrol acetate [Zoely]), whereas the quadriphasic pill containing EV and dienogest (Qlaira) substitutes the hormone-free break with four days of EV only and two days of inactive tablets. Reducing the number of inactive pills provides a greater margin for error if the first hormone pills in the cycle are missed and may provide higher contraceptive effectiveness than the traditional 21 day/seven day regimens.13,14
Extended COC use without a hormone- free break can be used to avoid bleeding at inconvenient times, minimise withdrawal bleeding and avoid symptoms of PMS, withdrawal headaches or pelvic pain in the hormone-free break.15,16 Evidence supports the safety of up to 12 months of continuous active pill use, and breakthrough bleeding with extended use generally improves over time as the endometrium stabilises. Although no studies of continuous use beyond 12 months are available, no safety concerns have been identified.15
Many women have historically self-initiated extended-cycle COC use with support from their GPs. Traditionally, this has involved ‘tricycling’ by running three cycles of hormone pills together and omitting the hormone-free break for two packs out of three. Some women also continue to take active hormone pills without a break for up to 12 months at a time. An electronic dispensing device is available to support the use of a flexible extended-cycle regimen for a COC containing 20 µg EE and drospirenone (Yaz Flex).17 However, women can be instructed how to manage this regimen with any standard COC pack.
Recently, a new pill (Seasonique) has become available in Australia that provides a prepackaged extended cycle of three consecutive months (84 days) of tablets containing 30 μg EE and 150 mg LNG followed by seven days of tablets containing 10 μg EE. Compared with traditional ‘do-it-yourself’ tricycling by taking extended consecutive active pills followed by a seven-day hormone-free interval, there is greater suppression of the pituitary ovarian axis and follicle development due to the reduced, rather than absent, hormone break.18 This is likely to be beneficial for women who experience withdrawal symptoms in the hormone-free break because the EE levels are not reduced to zero. In addition, this new pill provides a lower risk of breakthrough bleeding particularly after the first cycle, and overall blood loss is reduced compared with traditional regimes.18,19 Although Seasonique is not PBS-listed and cost may be a deterrent, it offers a convenient and easy to use alternative for women who can afford it, with additional potential benefits over running together packs of PBS-listed LNG/EE pills followed by a hormone-free interval.
Rather than following a tricycling regimen, some women may prefer a ‘menstrually-signalled’ regimen that involves continuing hormone pills until four days of bleeding or spotting occur and then instituting a four-day hormone-free break.17
Explaining that extended-cycle use is not damaging to health and that ‘blood is not building up inside’ can be reassuring to a patient. However, despite the advantages of either prepackaged or ‘do-it-yourself’ extended-cycle regimens, some women still prefer the predictability and reassurance of a regular withdrawal bleed.
Pills with progestogens other than LNG
Progestogens including cyproterone acetate, gestodene, desogestrel, drospirenone, dienogest and nomegestrol acetate have been developed to avoid androgenic side effects and to have a minimal influence on EE-induced lipid changes. Some studies suggest that pills containing 30 to 35 μg EE and either desogestrel, gestodene, cyproterone acetate or drospirenone increase the risk of VTE compared with pills containing LNG or NET by a factor of about 1.5 to 1.8. However, the absolute risk of VTE associated with any COC remains low.20
Some of these newer formulations offer additional potential benefits for hormonally-dependent conditions such as acne or premenstrual dysphoric disorder (PMDD), and some have TGA-approved indications for these conditions (Table). These indications are largely based on studies that prove superiority against placebo rather than against other COCs. There is insufficient clinical evidence to routinely and preferentially prescribe these progestogens over LNG formulations.
{kind=link}
{kind=link}
However, selecting a COC with a progestogen other than LNG for a pre-existing condition can be considered in the clinical situations described below.
Acne and hirsutism
The oestrogen in any COC may improve acne due to its effect on increasing sex hormone-binding globulin levels, which results in a reduction in free testosterone, even at a low dose or when combined with a relatively androgenic progestogen.
COCs containing an antiandrogenic progestogen (i.e. cyproterone acetate, drospirenone or dienogest) or a less androgenic progestogen (i.e. gestodene, desogestrel or nomegestrol acetate) have a theoretical advantage for the management of patients with androgenic symptoms. However, the older PBS-listed COCs containing NET may confer a potential benefit as NET is partially converted to EE (albeit at a rate of less than 0.5%).21 A beneficial effect can take up to six months and, importantly, a Cochrane review concluded that there is little difference between COC types in treating acne.2
Premenstrual syndrome and premenstrual dysphoric disorder
The 20 μg EE/3 mg drospirenone pill (Yaz) has been shown to be more effective than placebo in treating patients with PMDD over a three-month course.22 The effect is likely to be due to a combination of the shortened hormone-free break and the spironolactone-like properties of drospirenone. It is unknown whether the effect is similar in women with milder symptoms of premenstrual syndrome (PMS), if it persists beyond three months or is superior to other COCs.
Extended-cycle regimens of other COCs have been shown to be beneficial in managing women with PMDD or PMS.9,10
Heavy menstrual bleeding
All COCs are potentially effective in reducing menstrual blood loss through their overall antiproliferative effect on the endometrium. The quadriphasic EV/dienogest pill (Qlaira) and the E2/nomegestrol acetate pill (Zoely) are associated with rates of amenorrhoea up to 20% and 30% in their two-day and four-day hormone-free breaks, respectively.9,10 Qlaira is very effective compared with placebo in the treatment of women with heavy menstrual bleeding,3 but it is unclear whether it is superior to other COCs in this regard. Using an extended-cycle COC, such as Seasonique, or running individual pill packs together in an extended regimen without a hormone-free break may also be helpful. If COCs with E2 or EV are found to confer safety benefits at least equivalent to EE pills, they could potentially become a first-line choice for medically eligible women over 40 years of age with idiopathic heavy menstrual bleeding who prefer not to use a hormonal IUD.
Conclusion
New constituents and extended-cycle regimens for COCs offer potential safety advantages and reduced nuisance side effects and provide non-contraceptive benefits for women with hormonally-dependent conditions. Women preferring a COC over a long-acting reversible contraceptive method need to be made aware of the pros and cons of the different COCs to find the ‘best fit’ for their circumstances and stage of reproductive life. MT
COMPETING INTERESTS: Dr Bateson has received support to present at educational conferences and attend advisory commitees on behalf of Family Planning NSW from Bayer Healthcare and MSD. She has also attended an advisory committee for Teva Pharmaceuticals. Dr McNamee has received support to deliver a conference talk by MSD. Dr Stewart: None. Family Planning NSW and Victoria receive sponsorship for educational courses from Bayer Healthcare and MSD. Family Planning NSW has received funding for research from Bayer Healthcare and MSD.
References
- Richters J, Fitzadam S, Yeung A, et al. Contraceptive practices among women: the second Australian study of health and relationships. Contraception 2016; 94: 548-555.
- Arowojolu AO, Gallo MF, Lopez LM, Grimes DA. Combined oral contraceptive pills for treatment of acne. Cochrane Database Syst Rev 2012; (7): CD004425.
- Jensen JT, Parke S, Mellinger U, Machlitt A, Fraser IS. Effective treatment of heavy menstrual bleeding with estradiol valerate and dienogest: a randomized controlled trial. Obstet Gynecol 2011; 117: 777-787.
- The Faculty of Sexual & Reproductive Healthcare of the Royal College of Obstetricians & Gynaecologists (FSHR). UK medical eligibility criteria for contraceptive use (UKMEC). London; FSHR: 2017. Available online at: http://www.fsrh.org/standards-and-guidance/uk-medical-eligibility-criteria-for-contraceptive-use-ukmec (accessed June 2017).
- Weill A, Dalichampt M, Raguideau F, et al. Low dose oestrogen combined oral contraception and risk of pulmonary embolism, stroke, and myocardial infarction in five million French women: cohort study. BMJ 2016; 353: i2002.
- Lidegaard O, Nielsen LH, Skovlund CW, Skjeldestad FE, Lokkegaard E. Risk of venous thromboembolism from use of oral contraceptives containing different progestogens and oestrogen doses: Danish cohort study, 2001-9. BMJ 2011; 343: d6423.
- Gallo MF, Nanda K, Grimes DA, Lopez LM, Schulz KF. 20 µg versus >20 µg estrogen combined oral contraceptives for contraception. Cochrane Database Syst Rev 2013; (8): CD003989.
- Sitruk-Ware R, Nath A. Metabolic effects of contraceptive steroids. Rev Endocr Metab Disord 2011; 12: 63-75.
- Mansour D, Verhoeven C, Sommer W, et al. Efficacy and tolerability of a monophasic combined oral contraceptive containing nomegestrol acetate and 17b-oestradiol in a 24/4 regimen, in comparison to an oral contraceptive containing ethinylestradiol and drospirenone in a 21/7 regimen. Eur J Contracept Reprod Health Care 2011; 16: 430-443.
- Ahrendt HJ, Makalova D, Parke S, Mellinger U, Mansour D. Bleeding pattern and cycle control with an estradiol-based oral contraceptive: a seven-cycle, randomized comparative trial of estradiol valerate/dienogest and ethinyl estradiol/levonorgestrel. Contraception 2009; 80: 436-444.
- Macias G, Merki-Feld GS, Parke S, Mellinger U, Serrani M. Effects of a combined oral contraceptive containing oestradiol valerate/dienogest on hormone withdrawal-associated symptoms: results from the multicentre, randomised, double-blind, active-controlled HARMONY II study. J Obstet Gynaecol 2013; 33: 591-596.
- Jensen JT, Parke S, Mellinger U, Serrani M, Mabey RG, Jr. Hormone withdrawal-associated symptoms: comparison of oestradiol valerate/dienogest versus ethinylestradiol/norgestimate. Eur J Contracept Reprod Health Care 2013; 18: 274-283.
- Howard B, Trussell J, Grubb E, Lage MJ. Comparison of pregnancy rates in users of extended and cyclic combined oral contraceptive (COC) regimens in the United States: a brief report. Contraception 2014; 89: 25-27.
- Dinger J, Minh TD, Buttmann N, Bardenheuer K. Effectiveness of oral contraceptive pills in a large U.S. cohort comparing progestogen and regimen. Obstet Gynecol 2011; 117: 33-40.
- Edelman A, Micks E, Gallo MF, Jensen JT, Grimes DA. Continuous or extended cycle vs. cyclic use of combined hormonal contraceptives for contraception. Cochrane Database Syst Rev 2014; (7): CD004695.
- Halbreich U, Freeman EW, Rapkin AJ, et al. Continuous oral levonorgestrel/ethinyl estradiol for treating premenstrual dysphoric disorder. Contraception 2012; 85: 19-27.
- Klipping C, Duijkers I, Fortier MP, Marr J, Trummer D, Elliesen J. Contraceptive efficacy and tolerability of ethinylestradiol 20 mug/drospirenone 3 mg in a flexible extended regimen: an open-label, multicentre, randomised, controlled study. J Fam Plann Reprod Health Care 2012; 38: 73-83.
- Vandever MA, Kuehl TJ, Sulak PJ, et al. Evaluation of pituitary-ovarian axis suppression with three oral contraceptive regimens. Contraception 2008; 77: 162-170.
- Anderson FD, Gibbons W, Portman D. Safety and efficacy of an extended-regimen oral contraceptive utilizing continuous low-dose ethinyl estradiol. Contraception 2006; 73: 229-234.
- Therapeutic Goods Administration (TGA). Combined hormonal contraceptives. Safety advisory - updated information about risk of blood clots. Canberra; TGA: 2016. Available online at: https://www.tga.gov.au/alert/combined-hormonal-contraceptives (accessed June 2017).
- Mansour D. Safer prescribing of therapeutic norethisterone for women at risk of venous thromboembolism. J Fam Plann Reprod Health Care 2012; 38: 148-149.
- Lopez LM, Kaptein AA, Helmerhorst FM. Oral contraceptives containing drospirenone for premenstrual syndrome. Cochrane Database Syst Rev 2012; (2): CD006586.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.