Estetrol, a new oestrogen for contraception

The first new combined oral contraceptive pill to be approved in Australia in more than 10 years is now available on private prescription. The pill contains a novel oestrogen (estetrol), combined with drospirenone.
A new combined oral contraceptive pill containing estetrol in combination with drospirenone has been approved for use in Australia. This new pill contains 14.2 mg estetrol (equivalent to 15 mg of estetrol monohydrate) and 3 mg drospirenone in a 24/4 regimen. Estetrol, a synthetically manufactured hormone, is naturally produced in the human fetal liver. Like pills containing estradiol and estradiol valerate, which have been available in Australia for over 10 years, it has been developed with the theoretical aim of a lower risk of venous thromboembolism (VTE) than the widely available ethinylestradiol combined hormonal methods of contraception. Although studies have shown the estetrol/drospirenone pill has minimal impact on haemostatic factors compared with combined pills containing ethinylestradiol and drospirenone, there is no current evidence of a lower risk of VTE and contraindications remain the same as for other combined pills.
The combined estetrol/drospirenone pill has been shown to be highly efficacious and acceptable to users. It is safe to use in all medically eligible people until the age of 50 years. It is not listed on the PBS and is similar in cost to other non-PBS-subsidised combined hormonal methods.
What is the new estetrol/drospirenone pill?
The estetrol 14.2 mg/drospirenone 3 mg pill is packaged with 24 identical hormone tablets followed by four inactive tablets. It is packaged so that users always begin with an active pill. The estetrol monohydrate dose of 15 mg is used as the descriptor in most studies and is equivalent to estetrol 14.2 mg in the commercial product.
Estetrol
In nature, estetrol is produced in the fetal liver and small amounts can be detected in the maternal circulation during pregnancy. Estetrol differs in a number of ways from ethinylestradiol, which may confer benefits to pill users. Compared with ethinylestradiol, it has a limited impact on the metabolic profile, the renin-angiotensin aldosterone system, carbohydrate metabolism, triglyceride levels, sex hormone binding globulin and haemostatic factors. It has a weak affinity to breast tissue and limited impact on the liver.1,2
Current use of the combined contraceptive pill may be associated with a small increase in the risk of breast cancer.3 Both ethinylestradiol and estradiol have strong affinity to breast tissue, causing proliferation.4 In contrast, estetrol appears to act as a weak oestrogen in breast tissue, causing little proliferation, even at high doses.5 In vitro cancer proliferation models have shown that an estetrol/drospirenone combination is neutral on breast cancer development.6 However, it is unknown if this will translate to benefits in relation to breast cancer risk, and use in those with past or current breast cancer is generally contraindicated.
A novel potential point of difference to other combined hormonal contraceptives containing ethinylestradiol is a possible environmental benefit of estetrol. The exposure to marine life from contraceptive oestrogens is considered harmful. It is predicted that human use of estetrol is unlikely to result in detrimental aquatic exposure levels.7 Further research on aquatic models is ongoing to determine the environmental impact of this new oestrogen.
Drospirenone
Drospirenone is a fourth-generation progestogen derived from spironolactone. It closely matches the pharmacological profile of progesterone and has antigonadotropic, antiandrogenic and antimineralocorticoid properties.8 These are thought to contribute to a more favourable side effect profile.
Why drospirenone?
To assist with the choice of a suitable progestogen to pair with estetrol, a Phase 2 trial compared combinations of 15 mg or 20 mg estetrol with either drospirenone 3 mg or levonorgestrel 150 mg. A commercially available multiphasic estradiol valerate/dienogest pill was used as a comparator. At the end of six cycles, participants using estetrol/drospirenone had higher satisfaction and continuation rates compared with those using estetrol/levonorgestrel.9 The estetrol/drospirenone combinations also had the most favourable bleeding patterns, with a low incidence of both unscheduled bleeding and amenorrhoea, and were thus chosen for further trial.10
Ethinylestradiol/drospirenone pills appear to be associated with a higher rate of deep venous thrombosis than ethinylestradiol pills containing levonorgestrel or norethisterone, estradiol/nomegestrol pills and estradiol valerate/dienogest pills.11-14 However, in vitro studies show that the estetrol/drospirenone combination has a lower impact on haemostatic parameters than the ethinylestradiol/drospirenone combination and either a lower or equivalent effect, depending on the parameter, compared with an estradiol 30 mcg/levonorgestrel 150 mg pill.15,16 This gives some reassurance that the new estetrol/drospirenone pill is not expected to have a higher rate of deep venous thrombosis than existing pills and gives some hope that its use might be associated with a lower increased risk. However, results of long-term post-marketing surveillance studies to determine the VTE risk to allow for comparison with other combined pills will not be available for several years.
How does the estetrol/drospirenone pill work?
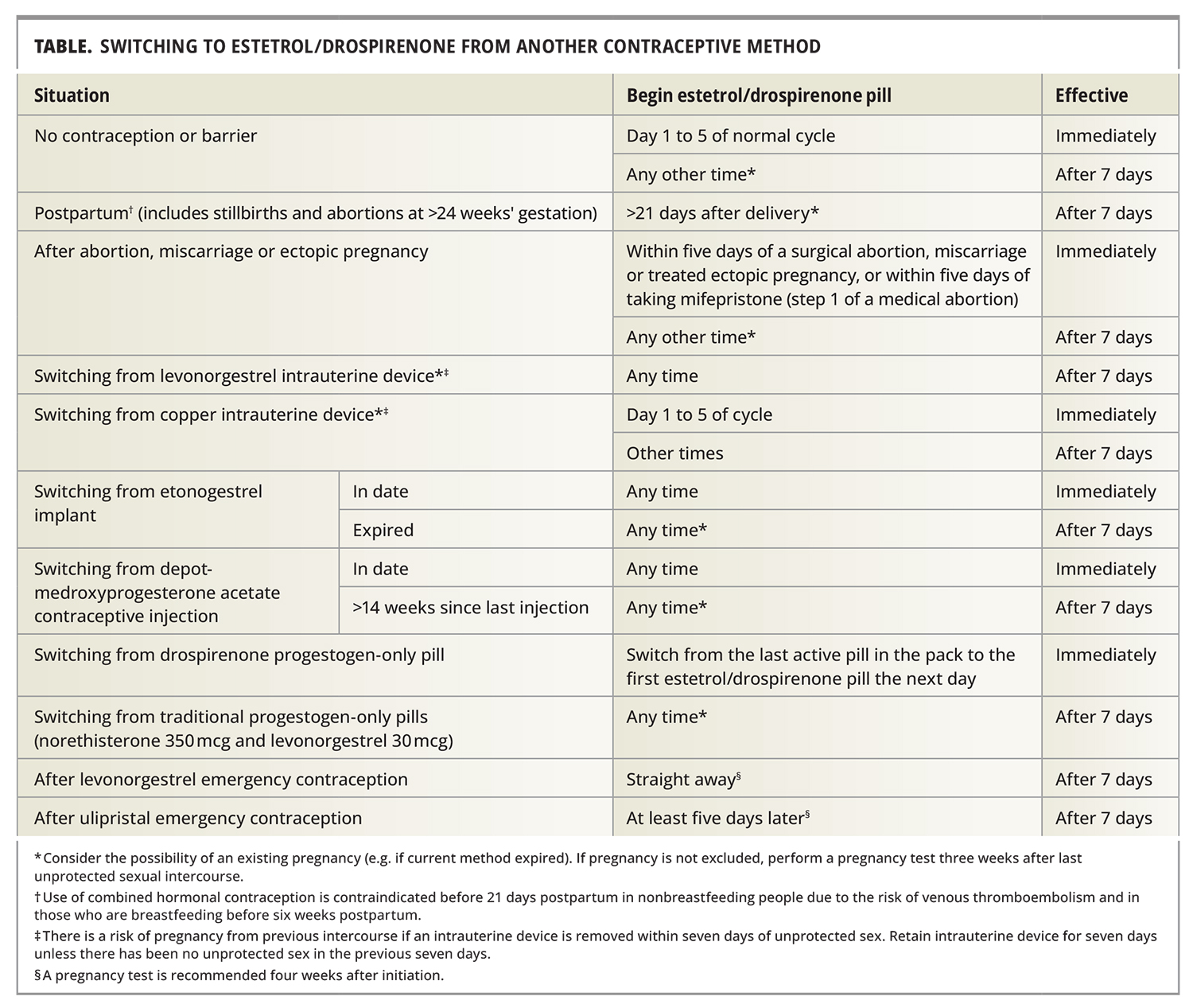
As with other combined hormonal contraceptives, the estetrol/drospirenone pill acts primarily to inhibit ovulation and thicken the cervical mucus.17 The four days of inactive tablets allow for a withdrawal bleed. Rules for pill initiation, switching from other methods of contraception and for managing missed pills are the same as for other combined hormonal methods (Table). The ‘missed pill window’ is 24 hours, similar to other combined pills.
{kind=link}
How effective is the new combined pill?
The estetrol/drospirenone pill appears to have an efficacy similar to that of other combined hormonal methods. The Pearl Index indicates the number of unintended pregnancies per 100 person-years of exposure. Combined hormonal methods are estimated to have a Pearl Index of around 0.5% effective in perfect use and 7% in typical use.18
Two large, multicentre, open label, Phase 3 trials recruited participants aged 18 to 50 years in Europe and 16 to 50 years in North America; the Pearl Index, based only on method failures, was 0.29 and 1.43 for the European and North America trials, respectively. The European trial showed no significant change in the Pearl Index when only those aged 18 to 35 years were included. The North American trial showed a difference in efficacy by age when all pregnancies (including those due to factors such as drug interactions and nonadherence were included. The Pearl Index was 3.07 in those aged 16 to 25 years, compared with 2.29 in those aged 26 to 35 years.19,20 The higher failure rate in the North American trial compared with that in the European trial is consistent with higher failure rates seen in trials of other oral contraceptive methods in these two settings.21,22
There was no significant difference in efficacy in participants with a body mass index (BMI) of 30 kg/m2 or higher, compared with those with a BMI of less than 30 kg/m2. However, only about one in five participants had a BMI greater than 30 kg/m2 and, as the trial protocols excluded those with a relatively strong contraindication to combined pill use, none had a BMI of 35 kg/m2 or greater.19
Return to fertility
A rapid return to previous fertility is expected, similar to other combined hormonal methods. Ovulation occurred at an average of 15.5 days after stopping estetrol/drospirenone after three cycles of use.23
Safety profile
Three serious adverse events considered to be treatment-related were reported in the two Phase 3 studies: a lower extremity VTE, an episode of depression requiring hospitalisation and an ectopic pregnancy.19,20
Serious risks
Venous thromboembolism
The main serious risk associated with combined pill use is VTE. The background risk of VTE for those of reproductive age is around two per 10,000 users per year and increases to five to 12 per 10,000 per year for combined hormonal contraception users, depending on the oestrogen and progestogen formulation.24 Until further information is available, the estetrol/drospirenone pill is considered to have a similar risk to levonorgestrel-containing combined pills.
Arterial disease
There is a small increase in the risk of stroke and myocardial infarction with combined hormonal contraception use but the absolute risk of these conditions is extremely low in patients with no additional risk factors. The risk decreases with a decrease in the dose of ethinylestradiol; however, no change in risk is seen in relation to progestogen type.25 The risk with estradiol and estradiol valerate pill use is similar to that of ethinylestradiol pills.11,26 Currently the risk of arterial disease for the the estetrol/drospirenone pill is unknown and considered to be similar to that for combined pills containing 20 to 30 mcg of ethinylestradiol.
Hyperkalaemia
There is a theoretical concern that the antimineralocorticoid activity of drospirenone could result in hyperkalaemia. However, although there were two cases of raised potassium levels, no clinically significant cases were reported in any of the clinical trials.19,20 There is no recommendation to measure the serum potassium level before initiation of the estetrol/drospirenone pill.27
Tolerability and side effects
Continuation rate
In the two large Phase 3 studies conducted in Europe and North America, of those who started the trial medication, 78% and 55% completed all 13 treatment cycles, respectively.19,20 Loss to follow up and consent withdrawal was much higher in the North American trial than the European trial, accounting for more than half of those who discontinued the study, which is typical of other contraceptive trials in this region.28,29
Bleeding patterns
Bleeding was generally predictable. In the European Phase 3 trial, scheduled bleeding or spotting occurred in over 92 to 94% of cycles and with a medium duration of four to five days. No scheduled bleeding occurred in 6 to 8% of cycles. Unscheduled episodes of bleeding or spotting lasting a mean of three days, of which around 72% were spotting only, occurred in 19.2% in cycle 1 and dropped to a low of 12.8% by cycle 11. The percentage of participants with amenorrhoea ranged from 5.6 to 8.1% in all cycles. Only around 3% of participants withdrew from the trial for reasons related to bleeding.20 The figures for unscheduled bleeding and absence of scheduled bleeding were slightly higher in the North American trial, but discontinuation for reasons related to bleeding were also uncommon (about 2.2%).19
Other side effects
About 10% of participants withdrew from each trial because of an adverse event. About 30% of these were due to bleeding problems. Other reasons for withdrawal included acne, decreased libido, mood changes and weight gain, but rates were low.19,20 Adverse events, excluding bleeding difficulties, occurred in more than 2% of participants and included acne, headache, breast pain, decreased libido and dysmenorrhoea in both large Phase 3 trials. Weight gain and nausea were also reported in the North American trial.
Noncontraceptive benefits
The estetrol/drospirenone pill is expected to reduce dysmenorrhoea, menstrual bleeding and acne in the same way as other combined hormonal methods. Theoretically, drospirenone-containing combined pills may have a beneficial effect on acne compared with formulations containing more androgenic progestogens, such as levonorgestrel. However, the oestrogen-related rise in sex hormone binding globulin and consequent reduction in free testosterone, considered to be a major driver of the beneficial effect of combined hormonal methods with ethinylestradiol and estradiol on acne, does not occur with estetrol and a beneficial effect on acne may not occur.1,30
The estetrol/drospirenone pill may have some benefits for metabolic parameters. Compared with ethinylestradiol 30 mcg/levonorgestrel 150 mcg and ethinylestradiol 20 mcg/drospirenone 3 mg, the estetrol/ drospirenone combination showed a lower increase in triglyceride levels in a small randomised, open label, Phase 2 trial of 98 participants.1
Unlike ethinylestradiol-containing pills, the estetrol/drospirenone combination demonstrated limited stimulation of the renin-angiotensin aldosterone system in the small Phase 2 trial, which theoretically could have a long-term benefit on blood pressure.2 Additionally, drospirenone can result in a drop in blood pressure due to its antimineralocorticoid effect. However, the two large Phase 3 trials have not published data on blood pressure, so the effect is unknown.
Another small trial of estetrol 15 mg/drospirenone 3 mg use over six cycles showed a greater proportion of participants lost more than 2 kg compared with those who gained more than 2 kg of body weight (36% vs 20%).9 However, it is unknown whether there was a change in mean body weight for participants overall. Moreover, the large European Phase 3 trial showed a mean increase in body weight of 0.68 kg compared with baseline weight, suggesting no clinically significant longer-term impact on weight.20
Continuous use
Although no studies have examined continuous use of estetrol/drospirenone pills to skip withdrawal bleeds, patients can be advised that there is no harm in trialling this approach. Active pills can be taken continuously until troublesome unscheduled bleeding occurs. A hormone-free break of four days can then be initiated if at least 21 active pills have been taken consecutively before the break.
Practical considerations
Contraindications
The Medical Eligibility Criteria (MEC) system of the UK Faculty of Sexual and Reproductive Health (FSRH) guides safe choice of contraceptive options in Australia. This system assigns a category of 1 to 4 to a variety of risk factors for use of the reversible ongoing, nonbarrier methods of contraception. The four categories range from MEC 1 (no contraindication) to MEC 4 (absolute contraindication).32
The estetrol/drospirenone pill has the same contraindications as other currently available combined hormonal methods. A personal, medical and family history is important to determine patients who are medically ineligible for this pill. Contraindications are mostly related to risk factors for, or a history of, arterial or venous disease. Some important MEC 3 or 4 contraindications include a history of migraine with aura, smoking from the age of 35 years, a BMI of 35 kg/m2 or greater, hypertension, severe liver disease, lactation if the infant is less than six weeks old, a personal history of breast cancer or carriers of gene mutations associated with breast cancer. A full list can be found at https://www.fsrh.org/standards-and-guidance/documents/ukmec-2016-summary-sheets/.
Other important considerations for the use of combined hormonal pills include patients who have difficulties taking pills on a regular basis at the correct time (e.g. shift workers), and patients who may have difficulty accessing ongoing contraceptive prescriptions and supply.32
Drug interactions
As the cytochrome P450 enzymes do not play a major role in the metabolism of estetrol, there may be fewer drug interactions than with ethinylestradiol or estradiol pills.2 However, drospirenone is metabolised by this pathway and will be affected by drug interactions. The estetrol/drospirenone pill is considered to have a similarly lower efficacy to other combined hormonal contraceptives with concomitant use of medications that induce the cytochrome P450 enzymes, including a number of antiepileptics, rifampicin and rifabutin.31 Switching to a hormonal or copper intrauterine device or a depot medroxyprogesterone injectable is recommended for people taking liver enzyme inducers long term.
Use of the estetrol/drospirenone pill across the reproductive life course
Adolescents
Although the North American Phase 3 trial included people aged 16 and 17 years, the number of adolescent participants is not specified and any difference in efficacy in this age group is unknown.19 The estetrol/ drospirenone pill is expected to have no adverse effects on bone density. Mouse models indicate estetrol has a strong estrogenic effect on bones.33 A Phase 2 trial of 111 participants showed no significant imbalance in biomarkers of bone degradation and bone formation with varying doses of estetrol combined with either drospirenone or levonorgestrel.34 Although it would not be a first-choice pill for patients with acne, and cost may be an issue for some adolescents, it a suitable contraceptive choice for adolescents wanting an oral method.
Postpartum and postabortion
As with other combined hormonal pills, the estetrol/drospirenone pill cannot be used during lactation for the first six weeks. After that, in breastfeeding women, its use is MEC 2 until six months, after which its use is MEC 1. For patients not breastfeeding, its use is MEC 3 to 4 until three weeks postpartum and then MEC 2 to 3 from three to six weeks postpartum, depending on risk factors for VTE. It can be used immediately after first trimester medical or surgical abortion and is immediately effective if initiated within the first five days of the procedure.
Perimenopause
The estetrol/drospirenone pill can, like other combined hormonal methods, be used until the age of 50 years, after which a switch to a nonhormonal or progestogen-only method is recommended.35 There are very few studies of combined hormonal preparations at contraceptive doses used to control menopausal symptoms.36 Estetrol 15 mg has been preliminarily trialled and found to be effective in reducing menopausal symptoms, so the combined preparation is likely to be suitable for use in patients aged under 50 years who suffer from hot flushes but still require contraception.37 Larger Phase 3 trials are underway to assess safety in postmenopausal women.
Initiation of the estetrol/drospirenone pill
The estetrol/drospirenone pill is designed to start with an active pill. It is immediately effective if it is:
- started on day 1 to 5 of a regular menstrual cycle. It is important to note that this recommendation is based on FSRH guidance for all combined hormonal methods; the product information advises starting on day one of a natural cycle for immediate effectiveness with the additional use of condoms at all other times27,31
- started less than 21 days postpartum (contraindicated due to risk of VTE)
- started within five days of an abortion.
The estetrol/drospirenone pill can be initiated using the ‘Quick Start’ method at any time: advise patients to start with the first pill of the pack (active pill) and use condoms until seven active pills have been taken. If pregnancy cannot be excluded before initiation, a pregnancy test is recommended four weeks after starting, regardless of bleeding experienced.
The Table provides advice on switching to the estetrol/drospirenone pill from other methods of contraception.
Missed pill advice
The missed pill advice is the same as for the other combined oral contraceptives on the market (Flowchart).
Conclusion
The estetrol/drospirenone pill is a new choice of combined hormonal contraception that has high user satisfaction and a low level of side effects. It has a number of theoretical benefits, including a potentially low environmental impact, low metabolic profile, a limited effect on haemostasis and a low impact on hepatic and breast tissue. It has potential benefit as a contraceptive in patients aged under 50 years who are experiencing menopausal symptoms. The performance of the estetrol/drospirenone pill in relation to other currently available combined hormonal methods is yet to be determined; however, this pill increases the range of options for patients who prefer an oral method and increases the opportunity for an individual patient to find a pill that suits their needs. MT
COMPETING INTERESTS: Professor Bateson has presented on Nexstellis at educational events for doctors sponsored by Mayne Pharma and attended an Advisory Board for Mayne Pharma but has not been personally remunerated for these services. Dr McNamee’s employer Sexual Health Victoria receives funding from Bayer Australia and New Zealand and Organon Australia to provide educational activities to doctors and nurses and has been paid for consultative advice given by Dr McNamee to Mayne Pharma.
This article is for general information purposes only, and the full product information should be consulted before prescribing any of the mentioned medications.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.