To sign or not to sign. Dealing with requests for vaccination exemption


Childhood immunisation
Children's health
There are few valid reasons to sign an Immunisation Medical Exemption form. It is important that GPs understand what these are, and how to manage common vaccine concerns that may contribute to exemption requests.
Anecdotal reports suggest that more parents are presenting to GPs requesting completion of an Australian Immunisation Register (AIR) Immunisation Medical Exemption form since the Federal Government’s ‘no jab, no pay’ policy was introduced on 1 January 2016. The no jab, no pay policy removed the ability for parents to register ‘conscientious objections’ to vaccination, which allowed them to be exempt from the requirement that their children be fully vaccinated to receive certain Federal Government family assistance payments. A new AIR Immunisation Medical Exemption form, which currently only GPs are able to complete, was also introduced on 1 January 2016 and is available online (https://www.humanservices.gov.au/health-professionals/forms/im011).
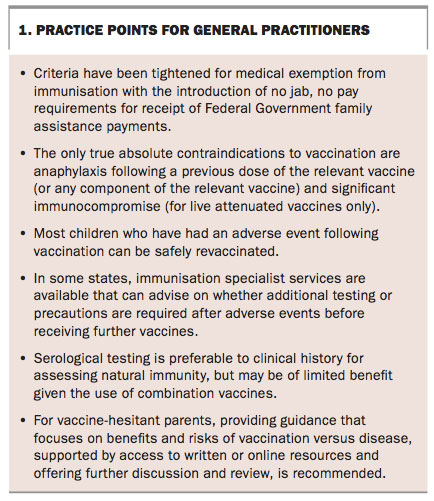
Immunisation is one of the most successful and cost-effective health interventions. Valid immunisation exemptions are medical contraindication according to the Australian Immunisation Handbook guidelines and natural immunity to a disease.1 To ensure that children are not inappropriately denied the benefits of immunisation, it is important that GPs understand what the true medical contraindications are and what constitutes adequate evidence of natural immunity. It is also important that GPs understand how to recognise and manage common concerns, including those about adverse events after vaccination, that may contribute to parents’ requests for completion of exemption forms. Practice points for GPs are listed in Box 1.
{kind=link}
What are the true medical contraindications to vaccination?
The only true absolute contraindications to vaccination are anaphylaxis following a previous dose of the relevant vaccine (or any component of the relevant vaccine) and significant immunocompromise (for live attenuated vaccines only).1 A range of additional false contraindications are listed in the Australian Immunisation Handbook, including family history of adverse events after immunisation, past history of convulsions, neurological conditions and recent or imminent surgery.1
Children with acute febrile illness (temperature ≥38.5°C) should have vaccination temporarily deferred; however, an AIR Immunisation Medical Exemption form is not required for deferrals of this nature, which are likely to be of short duration. The provisions for temporary exemption are likely to be relevant only in the case of acute major medical illness when a child is hospitalised and clinically unstable, during pregnancy or when there is significant immunocompromise anticipated to be of short duration (for live attenuated vaccines only).
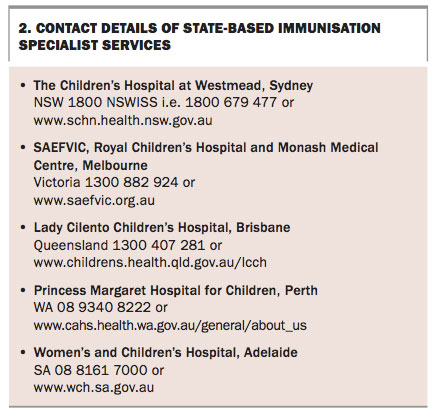
In general, most children who have had an adverse event following vaccination can be safely revaccinated. In some states, immunisation specialist services are available that can advise on whether a particular child requires any additional testing or precautions before receiving further vaccines (see Box 2 for contact details).
{kind=link}
What evidence is required to be confident of natural immunity?
Patient history is often unreliable in terms of assessing natural immunity and physician-based clinical diagnosis is considerably less reliable than laboratory testing (via serology, polymerase chain reaction [PCR] or antigen detection). Vaccine preventable diseases such as measles, mumps, rubella and hepatitis B infection are now uncommon among children in Australia and other infections can have similar clinical presentations.
Testing for natural immunity
The AIR Immunisation Medical Exemption form has provisions for natural immunity to hepatitis B, measles, mumps, rubella and varicella viruses. If there is a history of pertussis or rarer conditions such as diphtheria, tetanus, meningococcal disease and polio, GPs should vaccinate the child rather than test serologically for immunity, because it is unclear if a satisfactory level of immunity is maintained following natural infection from these conditions. It may also be simpler to vaccinate for other conditions such as measles, mumps, rubella and varicella, as exemption to a combination vaccine is only possible if immunity is confirmed for all the antigens in the vaccine.
In some cases parents may request serological testing to see if their child has responded to previous doses of a vaccine. This is not recommended as a routine practice because immunity wanes after vaccination and serology results are dependent on the time post-vaccination that the sample is collected. A negative serology test may reflect waning immunity rather than non-response to the previous dose(s) of vaccine. It is safe to vaccinate a child who has pre-existing vaccine- or natural infection-induced immunity.
Identifying and managing concerns contributing to requests for vaccination exemption
As well as removing exemptions for ‘conscientious objections’, the no jab, no pay policy has also extended immunisation requirements for receipt of Federal Government family assistance payments to age 19 years on an annual basis (previously only at 1, 2 and 5 years of age). Although some parents of incompletely vaccinated children are happy to have them undergo catch-up vaccination, some have concerns, ranging from minor to major. Some parents, rather than having any philosophical opposition
to vaccination, will be concerned about vaccine safety due to previous adverse events in their child or in other family members, or will be concerned about what they have heard or read about vaccine safety. Some parents of incompletely vaccinated children are concerned about vaccine side effects and ‘toxic and harmful’ vaccine ingredients or have concerns that vaccines are ineffective and prefer ‘natural’ preventive approaches.
Leask and colleagues reported that parents can be divided into five different groups based on their vaccine concerns or acceptance.2
These five groups are:
- unquestioning acceptors
- cautious acceptors
- hesitant
- late or selective vaccinators
- refusers.
Determining which of these five groups a parent falls into can assist healthcare providers to tailor their advice and management. In general providing guidance that focuses on benefits and risks of vaccination compared with disease, supported by access to written and online resources and offering further discussion, is recommended.
Refusers are often particularly challenging for GPs to deal with. Potential strategies include keeping the discussion brief but leaving the door open, acknowledging rather than dismissing their concerns, avoiding overt confrontation, and offering another appointment when they are ready or attendance at a specialist immunisation clinic.3 There are a range of resources available to assist healthcare providers and parents.3-5 Good communication with a parent who is worried about vaccinating their child requires patience, empathy, good listening skills and being responsive to specific concerns in an honest, frank and open manner.
In some cases, parents may wish to be selective about which vaccines the child receives. This can have the advantage of building confidence for the parent; if the schedule is started with no adverse events then acceptance of continuing or completing the schedule may increase. The disadvantage is that administering one vaccine at a time requires extra visits, does not significantly reduce the adverse event profile and requires a longer time to complete the recommended vaccine schedule, potentially putting the child at greater risk of acquiring infection. Splitting up vaccines into separate components – for example, giving the Haemophilus influenzae type b (Hib) component only of a multivalent vaccine – is not recommended. Parents should be advised that there is no additional safety benefit to splitting up vaccines and that for some vaccines, such as the measles mumps rubella vaccine, monovalent component vaccines are not available.
The risk of natural infection for individual children differs according to their age and this can be explained to parents. Although for many vaccine preventable diseases the disease risk is low, for others such as pertussis the disease is less well controlled and is particularly an issue for infants who are at highest risk of the more severe consequences of the disease including death. In the case of tetanus, the causative pathogen (Clostridium tetani ) is ubiquitous in the environment and is contracted by injury or wounds rather than person to person. So tetanus is therefore a potential risk to all children once mobile and is only able to be prevented by vaccination.
It is important to explain to parents that the risk of contracting a vaccine preventable disease also increases with travel, although this does depend on the destination of travel. In many countries the risk of infection is substantially higher than in Australia, and access to post-exposure treatment, such as tetanus immunoglobulin, can also be problematic.
Conclusion
There are few valid reasons to sign an Immunisation Medical Exemption form under the tightened requirements introduced in conjunction with the no jab, no pay policy in Australia. Specialist immunisation services are available in some states to assist healthcare providers in determining whether a valid medical exemption exists for individual children and advise on the management of adverse events following immunisation. Sustaining high vaccination coverage is required to control vaccine preventable diseases in Australia. MT
References
- Australian Technical Advisory Group on Immunisation. The Australian immunisation handbook. 10th ed (June 2015 update). Canberra: Australian Government Department of Health; 2015. Available online at: http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/7B28E87511E08905CA257D4D001DB1F8/$File/Aus-Imm-Handbook.pdf (accessed March 2017).
- Leask J, Kinnersley P, Jackson C, Cheater F, Bedford H, Rowles G. Communicating with parents about vaccination: a framework for health professionals. BMC Pediatr 2012; 12: 154.
- Danchin M, Nolan T. A positive approach to parents with concerns about vaccination for the family physician. Aust Fam Physician 2014; 43: 690-694.
- Australian Government Department of Health and Ageing. Myths and realities: responding to arguments against vaccination. A guide for providers. 5th ed. Canberra: Australian Government Department of Health and Ageing; 2013. Available online at: http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/AD34C3D063510C0CCA257D49001E73D4/$File/full-publication-myths-and-realities-5th-ed-2013.pdf(accessed March 2017).
- Australian Academy of Science. The science of immunisation: questions and answers. Canberra: Australian Academy of Science; 2016. Available online at: https://www.science.org.au/learning/general-audience/science-booklets/science-immunisation (accessed March 2017).
COMPETING INTERESTS: Dr Beard and Dr Wood work for the NCIRS, which receives most of its funding from the Australian Government Department of Health. The authors provided advice to the Department of Health on revisions to the Immunisation Medical Exemption form. Dr Wood has received NHMRC project grant and career development fellowship funding to conduct vaccinerelated research. Dr Wood also works for the Sydney Children's Hospital Network, which has received funding from GSK Biologicals to support investigator-initiated industry-supported vaccine trials.