A case of left-sided facial swelling. A benign or serious cause?

Facial injuries and disorders
Although a swollen parotid represents a diagnostic challenge, with thorough investigation it is possible to differentiate the benign from the serious causes.
As a GP working in your own practice and the local emergency department, you are frequently asked by patients to look at various lumps and bumps.
The case
It has been a busy Saturday afternoon in the emergency department when you pick up the next waiting patient: a 75-year-old man who presents with left-sided facial swelling. The patient reports three days of gradually increasing swelling and worsening pain on the left side of his face. He denies any hot or cold sweats, recent illnesses, trauma, travel or dental issues and there is no evidence of immunocompromise.
He recalls a similar episode that occurred about 10 years ago while overseas, and on that occasion he was admitted to hospital for five days. He is currently able to tolerate soft food and fluids, as long as he chews on the unaffected side. He has no difficulty swallowing, no change in his voice and no shortness of breath. He was seen by his GP two days ago and started on flucloxacillin, with no improvement. He tells you that it is becoming increasingly painful.
The history
The patient has a past history of hypothyroidism; lung cancer treated with pneumonectomy and local radiotherapy; and hypertension and hypercholesterolaemia, which are well controlled with irbesartan and simvastatin. He was previously diagnosed with prediabetes but has since lost some weight. He is an ex-smoker with a 10-pack-year history (he quit 20 years ago). He has no unwell contacts and lives with his wife.
Physical examination
On examination, the patient is afebrile and his vital signs are stable. He looks generally well apart from a grossly enlarged left parotid gland from 1cm anterior to the junction of the ear lobe to 2cm lateral to the nasolabial sulcus. There is no overlying redness or heat but the swelling is very tender. It feels firm, but it is difficult to isolate the layers involved and any attachments due to the patient’s discomfort. On bimanual examination there is a small area of fluctuance in the buccal tissue, but no pus or discharge from the Stensen’s duct. He has left-sided submandibular lymphadenopathy. He has good dentition, and there are no abnormalities on examination of the ears or nose. He is able to open his mouth but not to its full width due to pain. He has no vocal change, no tenderness on swallowing and no drooling. No other glands are enlarged, and he has no other lymphadenopathy. His cranial nerves are intact.
Provisional diagnosis and test results
You think it is likely that this man has suppurative parotitis, but you are concerned about possible abscess development, underlying salivary stone or malignancy. Although less likely, you are also aware that nonsuppurative parotitis is a concern. You order a CT scan of the soft tissue of the face; a full blood count; tests for urea, electrolytes and creatinine, liver function and C-reactive protein (CRP); a comprehensive metabolic panel; and blood cultures. You also ask the patient to swab inside his cheek if he feels anything ‘coming out’ of the duct.
His blood test results show inflammatory marker levels are mostly normal. His white cell count is within normal limits (8 x 109/L). He has mild lymphocytopenia (1.2 x 109/L) but with an elevated CRP level of 39mg/L. Electrolyte levels and liver function, renal function and thyroid function test results are all within normal ranges.
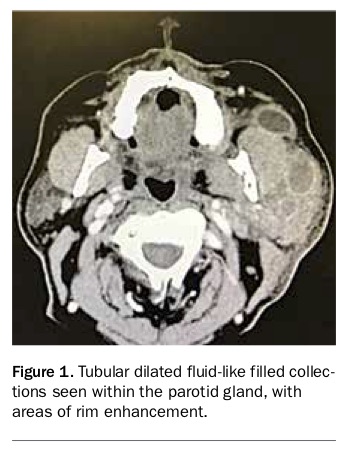
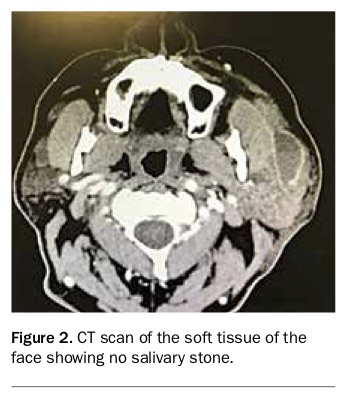
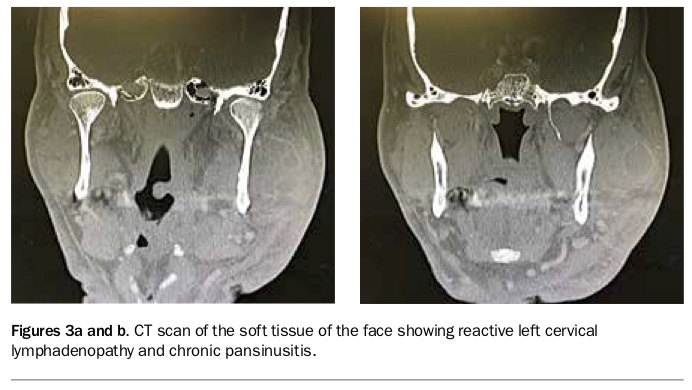
The CT scan shows diffuse thickening of the left parotid gland. There is a series of communicating tubular dilated fluid- like filled collections seen within the parotid, with areas of rim enhancement (Figure 1). There is no salivary stone visible (Figure 2). This is consistent with left-sided parotitis with underlying Stensen’s duct obstruction.1 There is an indeterminate mass-like focus measuring 12 x 11mm within the left parapharyngeal space protruding into the left lateral pharyngeal recess, which is suspicious of an underlying lesion. There is reactive left cervical lymphadenopathy and chronic pansinusitis (Figures 3a and b).
{kind=link}
{kind=link}
{kind=link}
Discussion
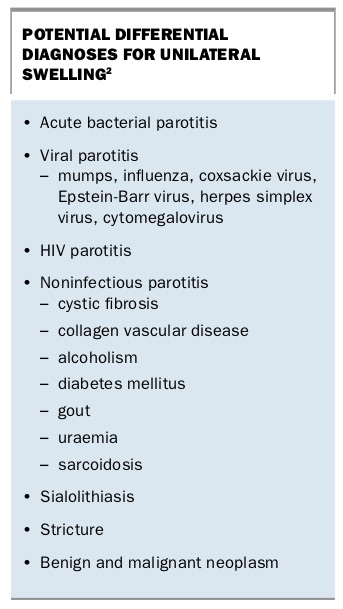
Acute swelling of the parotid gland usually represents either a partial or complete obstruction of the Stensen’s duct by a stone or stricture, or as a result of global infection. Occasionally the obstruction can be caused by a salivary gland tumour. Differentiating between the two can present a diagnostic challenge (Box).2
{kind=link}
Risk factors for developing bacterial parotitis include sialolithiasis, medications that dry the mouth such as anticholinergic drugs, recent dental intervention including aggressive teeth cleaning, malnutrition and salivary gland tumours.3 However, these risk factors are not strong predictors of disease, as evidenced by this patient who had none of these risk factors, other than a previous episode of parotitis.
The common clinical presentation of acute bacterial parotitis is a patient with a unilateral erythematous, swollen, tender parotid gland, from the preauricular area to the angle of the mandible that has developed over several days. There is often associated trismus, dysphagia and systemic symptoms such as fevers, rigors, chills and malaise. Pus can often be expressed from the Stensen’s duct by gentle massage from the preauricular area in an anterior direction to the os (which lies adjacent to the upper second molar). Given the extent of the infection in this patient, it is interesting that he had no dysphagia or signs of systemic illness. It is also noted that his white cell count was within normal limits, which is a good reminder of the importance of clinical suspicion in detecting abscesses.
Acute bacterial parotitis is usually polymicrobial. Staphylococcus aureus is the most frequently cultured pathogen; however, anaerobes and Gram-negative organisms are frequently present, including Enterobacteriaceae and Eikenella corrodens.3 It is important to consider the possibility of methicillin-resistant S. aureus in patients who have recently been admitted to hospital and Pseudomonas aeruginosa in immunocompromised patients. Culture of purulent material is useful to determine sensitivities of organisms in difficult- to-treat case of bacterial parotitis.
Imaging is important in identifying sinister or reversible causes of parotid swelling, parotitis and complications such as abscess formation. CT of the soft tissue is the most frequently used and is useful to visualise rim-enhanced abscesses (as seen in this case), solid tumours and for detecting salivary stones. Ultrasound is useful for detecting abscesses and stones in the duct or parenchyma. Magnetic resonance sialography can be used but is not usually the investigation of choice in the acute period.
Case outcome
The patient was admitted to hospital under the care of the ear, nose and throat surgeon and treated with intravenous flucloxacillin, clindamycin and analgesia. He had hourly parotid massages and was commenced on two-hourly sialogogues (lemon wedges). Two days after admission he had an ultrasound-guided percutaneous drainage of the left parotid abscess. There was no drainage from the Stensen’s duct and the parotid swelling recurred. The patient was booked for an elective left parotid ductoplasty in three days’ time. He was discharged home the same day on oral flucloxacillin (for five days) and analgesia. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.