Idiopathic (Bell’s) palsy – diagnosis and management

Idiopathic, or Bell’s, palsy is a sudden facial paralysis without a clearly defined cause, which can have severe physical and emotional consequences. By recognising key features of the condition and making an early diagnosis, GPs can instigate best-practice management with good clinical outcomes.
Bell’s palsy refers to a sudden-onset, unilateral, peripheral facial nerve palsy. Although considered to be idiopathic, a presumed aetiology is an inflammatory response to a recent or previous viral illness. The estimated annual incidence of Bell’s palsy is between 11 and 40/100,000, conferring a lifetime risk of one in 60. GPs are estimated to encounter an acute presentation once every two years.1 There appears to be no predisposition to Bell’s palsy based on sex, ethnicity or geographic location; however, pregnancy, diabetes and immunocompromised status increase the risk of occurrence.2 This article presents key clinical features and evidence to support the assessment and management of Bell’s palsy in general practice.
Aetiology
The pathophysiology of Bell’s palsy likely involves an inflammatory response to a viral infection, characterised by vascular distension, oedema of the nerve sheath and compression and ischaemia of the facial nerve.3
The predominant hypothesis about the pathogenesis of this condition involves a reactivation of herpes simplex virus (HSV-1), suggested by the presence of HSV-1 DNA in the geniculate ganglion, endoneurial fluid and saliva of affected patients.3 However, the evidence from studies is circumstantial, in part because of difficulties in recruiting patients with acute presentations of Bell’s palsy, which most often self-resolve and do not require additional investigation. Furthermore, the low frequency of recurrence of Bell’s palsy, compared with the viral reactivation more often seen with genital and oral herpes, is inconsistent with this explanation.
Another proposed aetiology is a cell-mediated autoimmune inflammatory response, characterising Bell’s palsy as a mono-neuritic variant of Guillain-Barré syndrome. This view is supported by findings of elevated concentrations of interleukin-1, interleukin-6, tumour necrosis factor alpha and B-cells, along with lower levels of suppressor T-cells, in affected patients.3
Clinical features
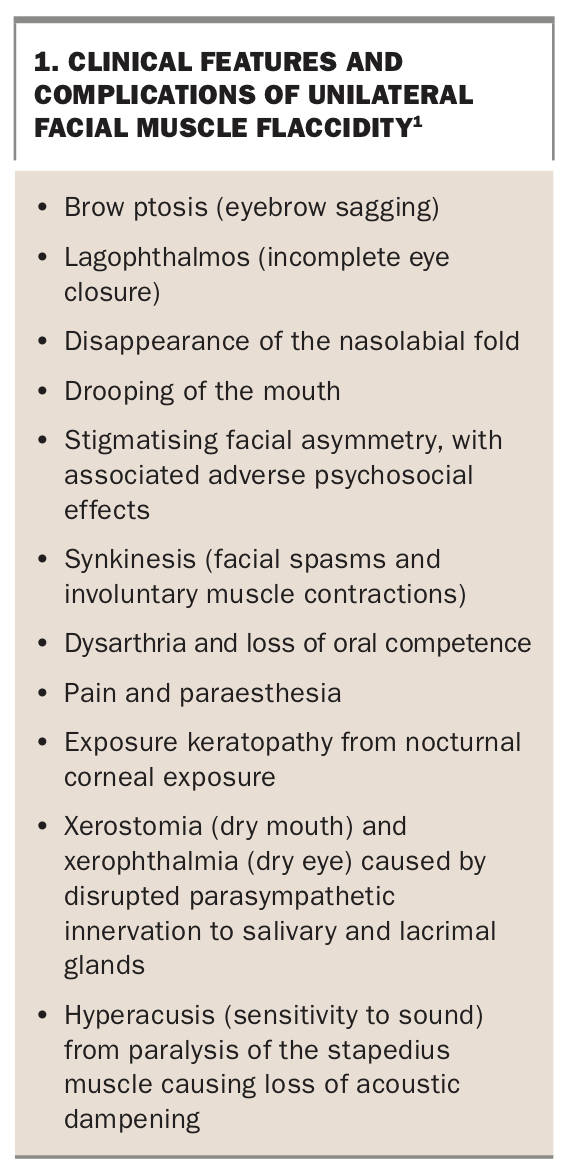
Patients with Bell’s palsy present with clinical signs that illustrate a unilateral flaccidity of facial muscles, including eyebrow sagging, inability to close the eye, disappearance of the nasolabial fold and drooping of the mouth.4 Hyperacusis (sensitivity to sound) caused by paralysis of the stapedius muscle, decreased taste sensation and dryness of the mouth and eye may also occur, providing some information about the location of the lesion; however, these findings have limited clinical significance for diagnosis or management.5 Additional cranial neuropathies, although uncommon, have been reported in patients diagnosed with Bell’s palsy. These include contralateral trigeminal, glossopharyngeal and hypoglossal neuropathies; ipsilateral facial sensory impairment; and bilateral facial palsy.6 Box 1 summarises the clinical features and complications of unilateral facial muscle flaccidity.1
{kind=link}
The onset of Bell’s palsy is acute and progressive over 48 to 72 hours, and most cases self-resolve gradually over three to twelve weeks. Even without any treatment, 70% of patients will have complete recovery, and a further 15% achieve near complete recovery.7
For the remaining 15% of patients, incomplete recovery has significant physical and psychological consequences. It can be devastating for patients’ quality of life, causing considerable distress and restriction in social activities.8,9
Diagnosis
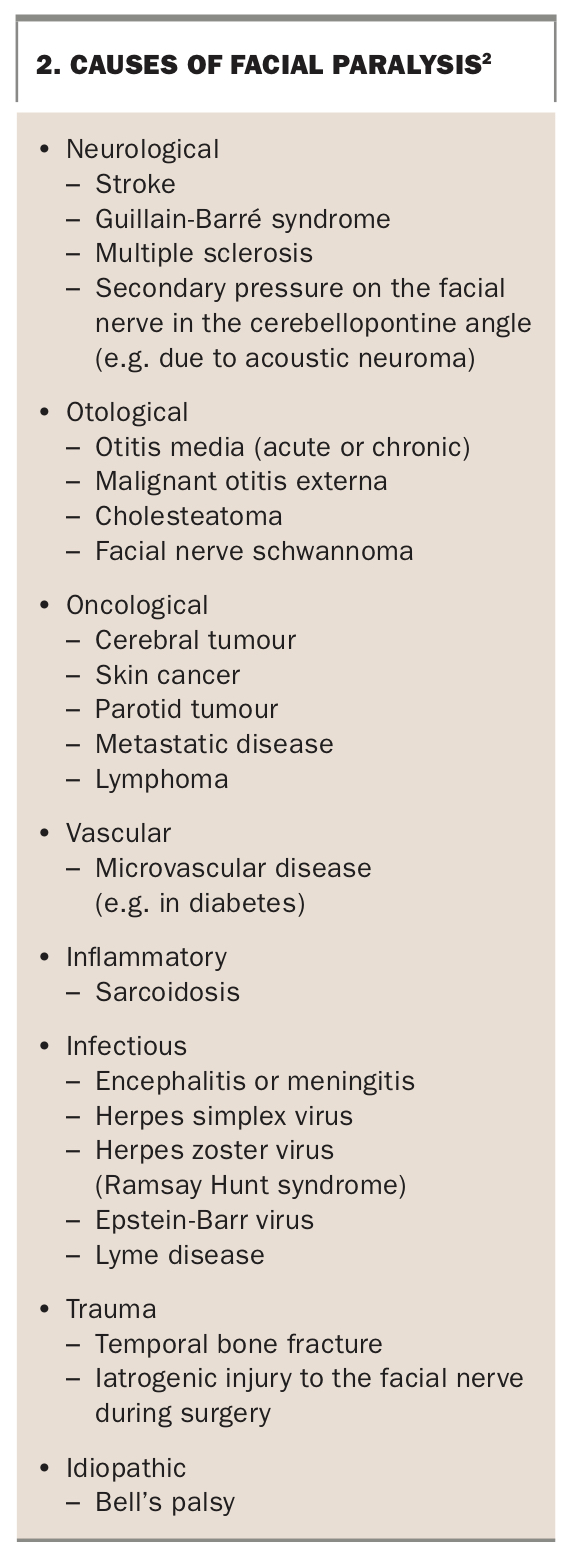
About 70% of all facial nerve palsies are considered Bell’s palsy.7 A comprehensive clinical assessment should seek to exclude other neurological, otological, oncological, vascular, inflammatory, infectious or traumatic causes for a patient’s symptoms (Box 2), including identifying any abnormality in the cerebellopontine angle.2 Bell’s palsy is a clinical diagnosis based on a history of acute, progressive symptoms of facial muscle weakness, with or without a viral prodrome, and examination findings of a lower motor neuron facial nerve palsy.
{kind=link}
It is important to confirm that symptoms are rapid in onset and consistent with unilateral facial muscle weakness. Patients should be screened for relevant risk factors for Bell’s palsy, including pregnancy, severe pre-eclampsia, hypertension, diabetes, immunocompromise, obesity, recent upper respiratory illness and a personal or family history of Bell’s palsy.2 Features such as dizziness, diplopia, dysphagia or facial numbness suggest a central neurological problem. A medical history of stroke, brain tumour, cutaneous head or neck cancer, parotid tumour, face or head trauma or local infection also predisposes patients to facial paralysis not in keeping with Bell’s palsy.2
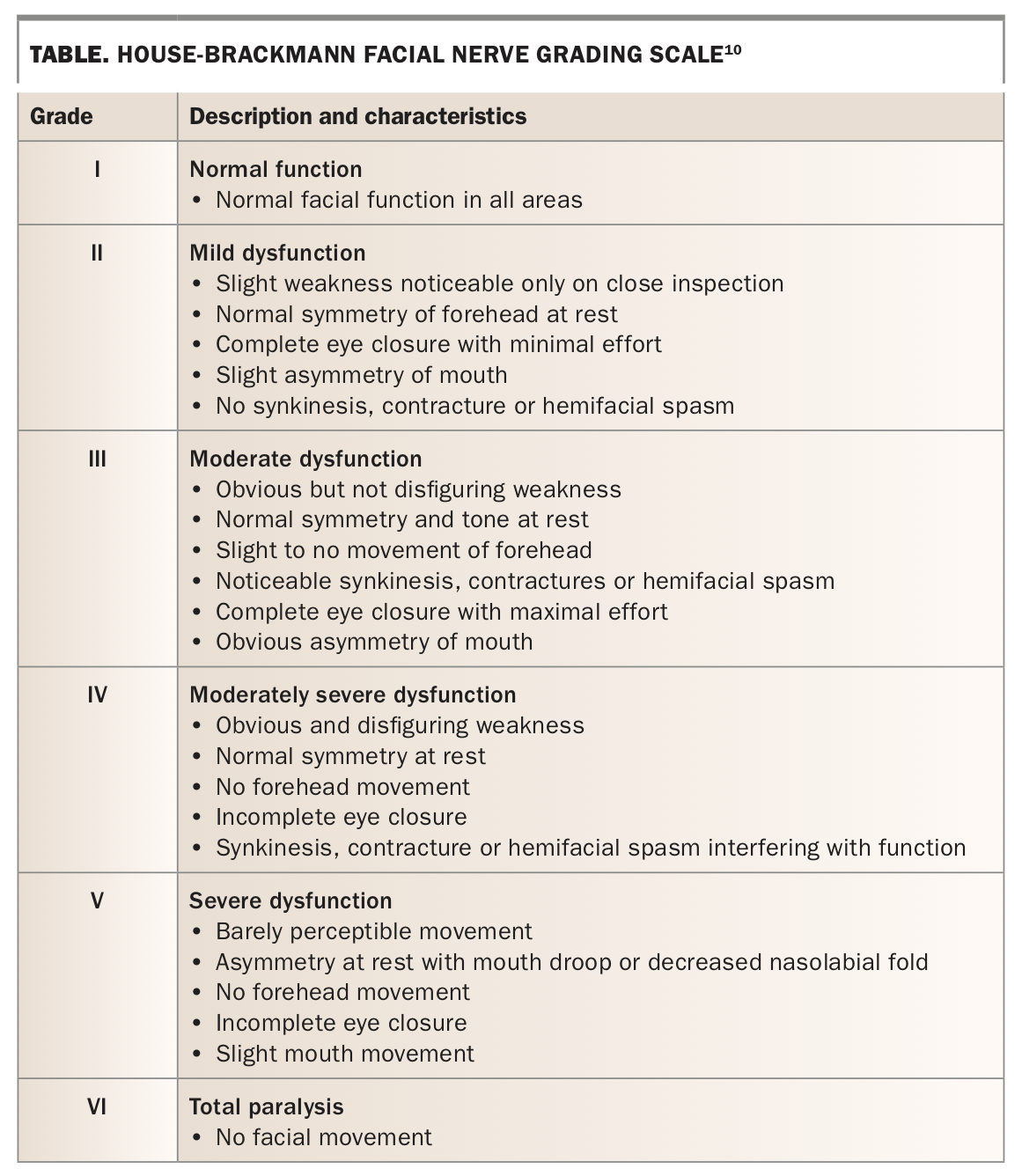
Careful examination of the cranial nerves, with a focus on the facial nerve, should be followed by a full neurological and general physical examination. This includes inspection of the ears and parotid glands, as well as the skin of the face, head and neck. The severity of a facial nerve palsy can be assessed using the House Brackmann grading scale (Table), which may be useful in monitoring long-term recovery.10
{kind=link}
A peripheral (lower motor neuron) facial nerve palsy, such as Bell’s palsy, will present with unilateral flaccid paralysis of facial muscles, including the frontalis muscle of the forehead. Patients are thus unable to raise their eyebrow or furrow their forehead. In contrast, a central (upper motor neuron) lesion, such as a middle cerebral artery stroke, will typically spare the forehead muscles and present with paralysis of the lower two-thirds of the face.
Examination of the ears, including the skin, auditory canal and tympanic membrane, is essential to exclude otitis media, otitis externa and cholesteatoma, which may be complicated by facial paralysis. Pain around the ear, deafness and a vesicular rash in the external auditory canal indicate herpes zoster infection, which, in the context of facial paralysis, suggests Ramsay Hunt syndrome.11
Benign or malignant tumours of the head and neck, especially the parotid gland, should be considered and appropriately excluded. Bilateral facial nerve paralysis is rare in Bell’s palsy and should prompt assessment for Guillain-Barré syndrome, Sjögren syndrome, sarcoidosis and Lyme disease in returned travellers from endemic areas.2,7
Investigations
Electrodiagnostic testing procedures have been used to define severity of damage to the facial nerve and to quantify improvements over time.2 Electroneurography (ENOG) involves surface electrodes measuring depolarisation of facial muscles after electrical stimulation of the facial nerve, while electromyography (EMG) uses needle electrodes inserted into facial muscles to record depolarisations after voluntary facial contractions. However, most patients presenting with Bell’s palsy will be diagnosed clinically, without requiring ENOG or EMG.7
Patients presenting with incomplete facial paralysis are highly likely to have a complete return to function, and there is no strong evidence that electrodiagnostic tests successfully predict which patients are more or less likely to recover.2,12
For patients who present with complete facial paralysis, ENOG testing performed seven to 14 days after onset may provide useful prognostic information. A response amplitude on the affected side exceeding 10% of the amplitude on the contralateral side is associated with a favourable prognosis.2,12 Further EMG testing may provide additional information for these patients, by demonstrating the presence of intact axons and thus indicating a possible recovery.2
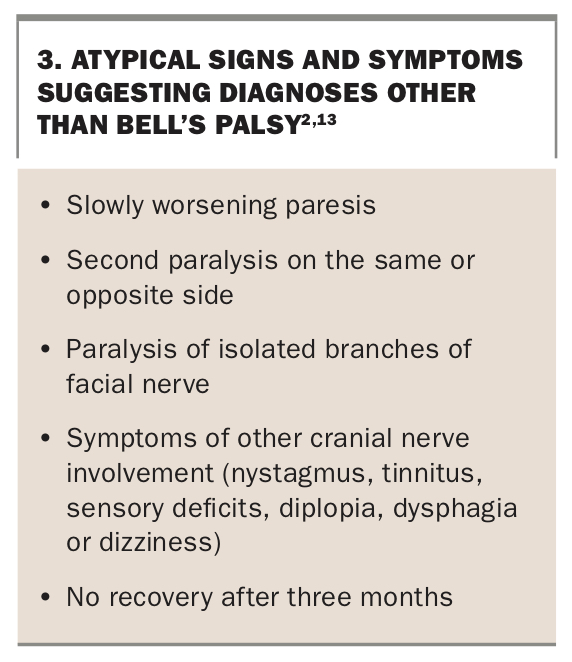
Although routine imaging at the time of diagnosis is not recommended, recent guidelines recommend contrast-enhanced MRI within one month of symptom onset (even if symptoms have resolved) to study the course of the facial nerve and exclude alternative diagnoses, including malignancy.13 Additionally, any patients with symptoms that persist beyond three months or with other red flag features atypical for Bell’s palsy (Box 3) should be further evaluated with MRI (with and without contrast) to visualise the entire course of the facial nerve.2,13
{kind=link}
If there is any concern about hearing loss, urgent audiology referral is required to rule out sudden sensorineural hearing loss.
Treatment
Medical management of Bell’s palsy aims to reduce the recovery time and improve long-term functional recovery. Oral cortico-steroids, which target the local inflammation and oedema that cause facial nerve compression in the fallopian canal, are the mainstay of acute treatment. There is evidence to suggest that corticosteroid treatment results in lower rates of facial dysfunction six months after onset of Bell’s palsy.14
American Academy of Otolaryngology–Head and Neck Surgery guidelines -recommend starting a 10-day course of oral corticosteroids within 72 hours of symptom onset in patients aged over 16 years: either 50 mg prednisolone daily for 10 days; or 60 mg prednisone daily for five days, then tapered for a further five days.2 Children have higher rates of spontaneous recovery than adults, and there is limited compelling evidence for corticosteroid use in children.15 Nevertheless, given the disease process is likely similar, oral cortico-steroids may be considered for children, with due consideration given to their side effects and risks. In pregnant patients, historical concerns about corticosteroid use presenting a risk to the fetus have not been supported by recent data.16,17 Pregnant patients should therefore be offered corticosteroid therapy, along with individualised advice that takes into consideration any comorbidities that may be affected, including diabetes, hypertension or mental illness.18
On its own, oral antiviral therapy is no better than placebo for improving facial nerve function, so, given the proven benefit of corticosteroids, antiviral monotherapy is strongly recommended against.2 Combination therapy with an oral antiviral agent and a corticosteroid has also not been convincingly shown to improve outcomes. However, in the absence of significant antiviral side effects, and with some lower quality evidence suggesting improvements in long-term recovery with the addition of an antiviral, patients may be offered combination therapy if treated within 72 hours of symptom onset.2,13 -Suggested antiviral regimens include valaciclovir 1000 mg three times daily for one week or aciclovir 400 mg five times daily for 10 days.19 In Australia, Bell's palsy is not a TGA-approved indication for either of these antiviral medications, so a private or off-label prescription is required.
Patients with impaired eye closure (lagophthalmos) must be appropriately managed with prophylactic eye protection measures to prevent ophthalmic complications, such as corneal abrasions or ulcerations, exposure keratitis and foreign body deposition.13,20 Supportive measures include lubrication with preservative-free eye drops during the day and ointment at night, moisture chamber glasses and eye closure techniques, such as eye patching or taping, which should be carefully explained to the patient. Patients should be counselled on the importance of preventive measures and advised to immediately report any visual disturbance, eye pain or irritation.21
Facial muscle rehabilitation (by appropriately trained physiotherapists) improves function in patients whose symptoms have not resolved, but its role in patients with new diagnoses is uncertain.22,23
Surgical decompression of the facial nerve may play a role for patients who show no clinical recovery despite two weeks of maximal medical therapy and with electrodiagnostic testing that shows more than 90% degeneration of the facial nerve.2,13
Referral
Most patients with Bell’s palsy can be appropriately managed and monitored by their GP, with re-evaluation within three months. Patients with any new or worsen-ing neurological symptoms warrant specialist neurologist review, while patients with any suspicion of head or neck malignancy may be more appropriately referred to an otolaryngologist or head and neck surgeon.2
Patients who experience severe lagophthalmos or who have no improvement with supportive eye care may be considered for surgical intervention after specialist ophthalmological referral.13
Over the medium to long term, some patients who have recovered will go on to develop unwanted contractions of the muscles of the eye or mouth with normal facial movements, known as synkinesis. Patients will often complain of eye closure when smiling or eating or of having muscular spasms. This can significantly affect their quality of life and only abates with neuromuscular training (facial physiotherapy) and, in refractory cases, with botulinum toxin injections to the muscles. Referral to a specialist in facial nerve disorders is warranted for any cases of incomplete recovery, residual flaccidity or synkinesis and spasm at three months after onset. These patients may benefit from surgery to improve both functional and aesthetic outcomes.
Long-term facial weakness can also have significant psychological impli-cations, including distress, depression, anxiety, poor self-confidence, social isolation and decreased quality of life.8,9 Referral to a psychologist for counselling or support may help patients manage the psychological consequences of their condition.
Conclusion
Bell’s palsy is a clinical diagnosis of idiopathic facial nerve palsy that requires careful consideration and exclusion of alternative causes. Although debate about the underlying aetiology continues, good evidence now informs the standard of care of oral corticosteroids for 10 days, with diligent eye care. The possible benefit of added antiviral therapy, although less definitive, outweighs its risks. Most patients recover completely, and medical management is effective for those who do not. Patients with Bell’s palsy can be largely managed in general practice. A team-based approach, involving an otolaryngologist, neurologist or ophthalmologist, as appropriate, is recommended for patients with unusual or prolonged symptoms. Due consideration must also be given to the significant psychosocial impacts of this condition. MT
COMPETING INTERESTS: None.
References
(549): 4-30.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.