Eliminating hepatitis C: Part 3. Curing hepatitis C in general practice

Dr Purcell is a Public Health Registrar, Burnet Institute, Melbourne. Dr Wade is an Infectious Diseases Physician at Barwon Health, Geelong, Vic; and Senior Research Fellow, Burnet Institute. Ms Accadia is a Research Nurse in the EC Partnership, Disease Elimination, Burnet Institute. Associate Professor Strasser is a Senior Staff Specialist in Gastroenterology and Hepatology at Royal Prince Alfred Hospital, Sydney; and Clinical Associate Professor at Sydney Medical School, University of Sydney. Dr Read is a Senior Staff Specialist and Director of the Kirketon Road Centre, South Eastern Sydney Local Health District, Sydney. Dr Allard is a GP and Postdoctoral Research Fellow at the WHO Collaborating Centre for Viral Hepatitis, Doherty Institute, Melbourne. Dr Baker is a GP at East Sydney Doctors; and Senior Lecturer at the University of Notre Dame Sydney, Sydney, NSW. Dr Pedrana is Postdoctoral Research Fellow in Disease Elimination, Burnet Institute; and Adjunct Research Fellow in the School of Population Health and Preventive Medicine, Monash University, Melbourne. Dr Doyle is Deputy Program Director of Disease Elimination, Burnet Institute; and Infectious Diseases Physician in the Department of Infectious Diseases, Alfred Hospital and Monash University, Melbourne, Vic.
Liver diseases
Most patients with hepatitis C are treated with pangenotypic direct-acting antivirals (DAAs) such as sofosbuvir/velpatasvir and glecaprevir/pibrentasvir. GPs experienced in the management of hepatitis C can prescribe DAAs independently. Others must consult with a specialist before prescribing; online resources can streamline this process. Important considerations before prescribing include barriers to adherence and drug interactions.
- Most people with hepatitis C can be treated with direct-acting antiviral (DAA) therapy in primary care.
- Pangenotypic DAA regimens that are well tolerated and effective against all hepatitis C genotypes include sofosbuvir/velpatasvir and glecaprevir/pibrentasvir.
- GPs who are experienced in the management of hepatitis C can prescribe DAAs independently, whereas others must consult with a specialist by phone, fax or email before DAA prescribing; online resources are available to facilitate this process.
- Considerations before prescribing DAAs include barriers to adherence and interactions between DAAs and prescribed medications and other drugs the patient takes.
- Clinical support, tools and resources to help GPs treat hepatitis C are available online.
GPs can treat most people living with hepatitis C using direct-acting antivirals (DAAs). These medications are highly effective, with few side effects, and can cure more than 95% of individuals. Curing an individual’s infection can significantly reduce their risk of developing liver disease and liver cancer, and reduce onward transmission, moving Australia towards the WHO goal of hepatitis C elimination.
This is the third article in a series on eliminating hepatitis C. Previous articles discussed how to identify your patients with hepatitis C and how to assess them in preparation for DAA treatment.1,2 This article focuses on initiating treatment in general practice.
Why treat hepatitis C in general practice?
More than 70,000 people with hepatitis C in Australia have been treated and cured since DAAs became available in this country. However, an estimated 165,000 people in Australia are still living with hepatitis C (projections based on a published model and updated MBS and PBS data).3 Most of these people are considered suitable for treatment in primary care.4 To eliminate hepatitis C as a public health threat in Australia, it is crucial that GPs engage in hepatitis C management for all people living with hepatitis C, including people who inject drugs. Providing hepatitis C treatment in general practice promotes treatment uptake, especially among marginalised populations.5
What treatments are available?
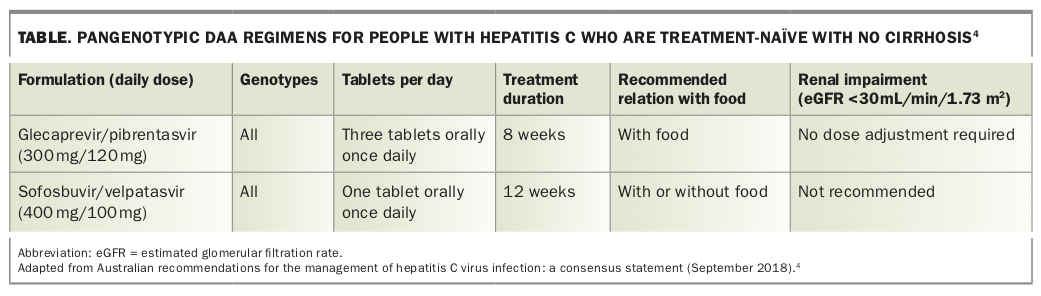
Although multiple DAAs are approved in Australia, 85% of all patients are now treated with pangenotypic DAA regimens that are effective against all hepatitis C genotypes.6 This article focuses on two pangenotypic DAA regimens:
- fixed-dose combination sofosbuvir/velpatasvir
- fixed-dose combination glecaprevir/pibrentasvir.
Both sofosbuvir/velpatasvir and glecaprevir/pibrentasvir have cure rates higher than 95%.4 These two pangenotypic DAA treatment regimens are well tolerated. Side effects may include mild fatigue, headache or nausea.4 The two regimens are compared in the Table.4
{kind=link}
Who can treat chronic hepatitis C?
Any medical practitioner or authorised nurse practitioner can prescribe DAAs for treatment of chronic hepatitis C.7 However, there are some provisos:
- Medical practitioners who are not experienced in the management of hepatitis C must consult with a specialist (gastroenterologist, hepatologist or infectious diseases physician) before prescribing DAAs.
- Medical practitioners and authorised nurse practitioners experienced in the management of hepatitis C can prescribe DAAs independently.
- Although most people with hepatitis C can be treated by nonspecialists, a selected minority need specialist treatment, as described below.
How do you consult with a specialist?
If GPs are not experienced in hepatitis management then they are required to consult with an experienced specialist. GPs can do this directly by phone, fax or email. This consultation process is one of the ways GPs can gain enough experience to prescribe independently.
Local HealthPathways have been created by Primary Health Networks to support GPs and authorised nurse practitioners to consult with specialists. The HealthPathways websites include key clinical information and details of local referral pathways, designed for use in primary care. GPs can access their local HealthPathways website via their Primary Health Network.
Some practitioners use the Gastroenterological Society of Australia (GESA) consultation request form (http://cart.gesa.org.au/membes/files/Resources/Hepatitis%20C/
Remote_consultation_form_updated_Sep_2018.pdf), which can be sent to the local specialist team. As the recommended DAA regimens have changed over time, it is important to ensure prescribers use the most current version of the consultation form.
An online portal, Reach-C, can also be used to obtain a response from a specialist within 24 hours (https://reach-c.ashm.org.au).
Important considerations before prescribing DAAs
Is the patient suitable for treatment in primary care?
The overwhelming majority of patients with hepatitis C can be treated in general practice. Patient populations who require referral for specialist management were discussed in the previous article in this series.2 They include people with advanced fibrosis or cirrhosis, hepatitis B or HIV coinfection, complex comorbidities, renal impairment, failed first-line DAA treatment or complex drug interactions.8
DAA treatment is not recommended for women who are pregnant or breastfeeding.9,10 Women should also be advised to wait four weeks after the end of DAA treatment before becoming pregnant.4 If a woman who has started DAA treatment becomes aware that she is pregnant, it is recommended that treatment is stopped.
Are there any barriers to adherence?
To maximise the likelihood of achieving a cure, it is important that the patient adheres to the treatment course. It is crucial to consider psychosocial issues that may pose barriers to medication adherence and to develop a collaborative plan to support treatment adherence. Ongoing drug and alcohol use is not a contraindication to DAA treatment. People with hepatitis C who are suitable for treatment in primary care can continue to consume alcohol as per NHMRC guidelines (no more than two standard drinks on any day) while receiving DAA treatment.11 It may be helpful to offer treatment such as opioid substitution therapy (OST) before DAA treatment.
The Australasian Hepatology Association (AHA) consensus guidelines provide recommendations about adherence support for people with hepatitis C who are receiving DAA treatment.12 The AHA guidelines describe 24 recommendations that encourage a patient-centred approach. Further information about supporting adherence can be found in the EC Partnership Practice Support Toolkit (https://ecpartnership.org.au/system/resource/80/file/EC_Partnership_Toolkit.pdf).8
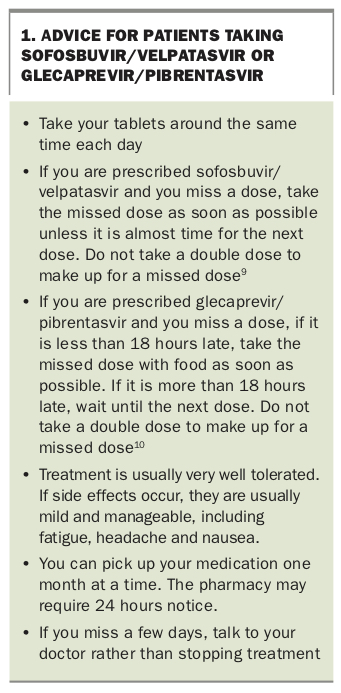
In addition to adherence strategies, it can be helpful to provide advice about taking DAA medications (Box 1).9,10
{kind=link}
Are there any drug interactions?
Interactions between DAAs and other drugs that the patient takes must be assessed before DAAs are prescribed.4 Other drugs include prescribed medications, over-the-counter preparations, complementary and alternative medicines and recreational drugs.
Drug interactions can be easily checked using the free University of Liverpool HEP Drug Interactions website and app (www.hep-druginteractions.org).13 Pangenotypic DAA regimens should never be dose adjusted; however, patient medications for other medical conditions may need to be adjusted in the presence of DAAs, as directed by the University of Liverpool website. The website offers detailed advice about options, including dose reduction, switching or stopping the interacting drug. DAA selection may also be influenced by potential drug interactions. The website includes some complementary medications and recreational drugs.
Problematic drug interactions are an indication for specialist referral or consultation.
The DAA prescription
PBS authority is required for hepatitis C treatment. Patients must be aged over 18 years.7 The telephone number to obtain an authority is 1800 888 333. The PBS operator will ask for the patient’s hepatitis C genotype and cirrhosis status. Authority will be given for the entire treatment course. Requirements for prescribing may change, so prescribers should ensure their knowledge is up to date.
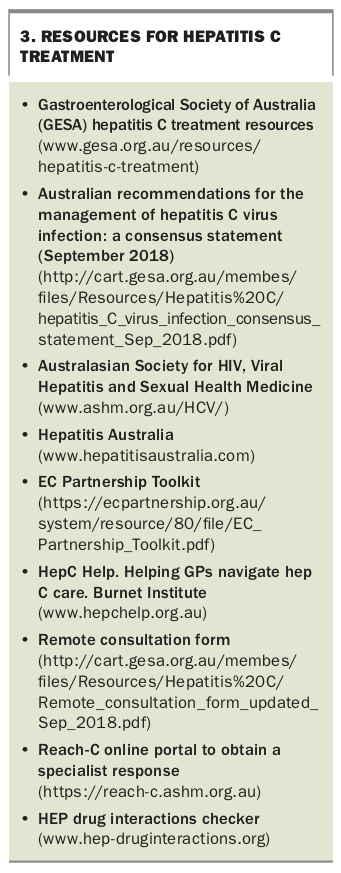
A case study that illustrates treatment of a patient with hepatitis C in general practice is shown in Box 2. Useful resources for hepatitis C treatment are shown in Box 3.2,13
{kind=link}
{kind=link}
Monitoring during treatment
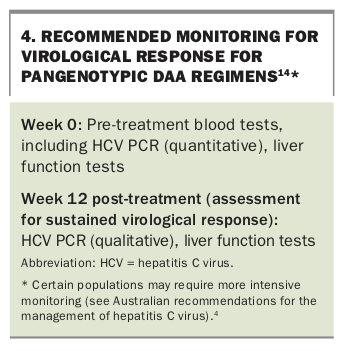
It is not necessary to order routine investigations during the course of DAA treatment.3 However, many doctors see their patient after the first month to review treatment adherence, side effects and patient concerns. The current recommendations for investigations before and after DAA treatment are shown in Box 4.14
{kind=link}
End of treatment - what next?
Hepatitis C cure is assessed 12 weeks after completion of DAA treatment. This involves a repeat hepatitis C PCR (to test for HCV RNA) and liver function tests. If the HCV PCR is negative then the patient is cured. It is not essential for the HCV PCR to be performed exactly 12 weeks after treatment – any PCR after this point is reliable at proving treatment has been successful; however, a test any earlier may occasionally be inaccurate as relapse can occur for up to 12 weeks after treatment. If liver function test results remain abnormal despite cure of hepatitis C, the patient should be evaluated for another cause of liver disease.
Nobody is immune to hepatitis C; the patient can be reinfected if re-exposed. People at risk of reinfection should be screened at least annually with an HCV PCR test (as they will remain positive for HCV antibodies indefinitely). They should also be provided with access to harm reduction, such as a needle and syringe program or opioid substitution therapy.4 Any HCV RNA detected after a confirmed successful hepatitis treatment course (ie, a negative HCV PCR result at least 12 weeks after treatment) is consistent with reinfection in a person with ongoing risks.
Some individuals will require ongoing care following DAA treatment. In addition, all patients who have not been cured by first-line DAA treatment should be referred to a specialist. Post-treatment care will be discussed in the next article in this series.
Conclusion
GPs can treat and cure most people living with hepatitis C. Treatment options can be tailored for the individual patient, and clinical support resources are available for GPs. Curing hepatitis C can be life-changing for patients and rewarding for GPs. Treating patients with hepatitis C in general practice is also crucial to achieving the WHO’s hepatitis C elimination goals. MT