Analgesia in home-based rehabilitation. Managing pain for functional gain

Rehabilitation
Increasing pressure on healthcare costs and the availability of hospital beds means that more patients are being referred for community-based ambulatory rehabilitation. GPs will increasingly manage the out-of-hospital rehabilitation of a cohort of patients with mild-to-moderate disability, including their analgesia requirements during the rehabilitation process.
- Increasingly, patients will be referred for home-based rehabilitation after discharge from hospital.
- GPs may be required to manage a patient’s analgesia during the rehabilitation process.
- Collaboration with a rehabilitation physician may be useful to establish a multidisciplinary treatment plan.
- Conditions need to be managed according to their likely causes and local resources, and management should always include analgesia, exercise and education.
Several conditions treated with rehabilitation-in-the-home (RITH) have been shown to achieve comparable outcomes to inpatient rehabilitation with acceptable safety profiles in selected populations. RITH is appropriate for patients recovering from joint arthroplasty (in particular total knee replacement), mild stroke and hip fracture and those in whom falls need to be prevented.1-4
The role of analgesia in rehabilitation
Performance enhancement
The role of analgesia in the rehabilitation population is different to its role in acute pain states in emergency departments or general practice. Analgesia in rehabilitation is considered for its performance-enhancing role in managing rest pain and allowing the patient to exercise, despite background pain.
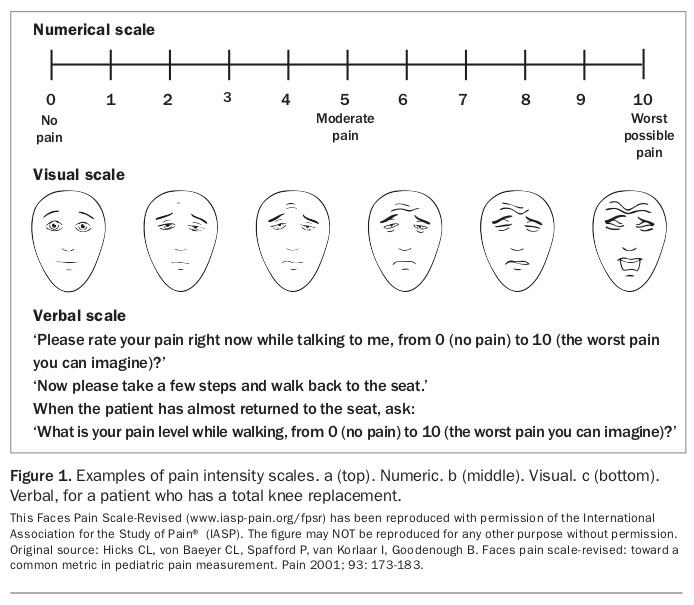
Titrating analgesia for rehabilitation is dependent on two parameters: pain level reduction at rest and movement. Using a visual pain rating scale is ideal, but a numerical or verbal rating scale can also be of benefit (Figure 1). It is not uncommon after total knee replacement for a patient’s pain rating to be 30% higher when walking, particularly for the first 20 to 30 seconds when anticipation and anxiety levels may be high. On commencement of moving, stiffness due to immobility is at its peak, leading to an increased need for proprioception from the missing native joint. At this point, proprioception from the neighbouring joints (ankle and hip) is relied on to maintain balance.
{kind=link}
Dual action
Analgesia includes medications that have dual effects such as pain relief and reduction in spasticity (e.g. pregabalin in spinal cord and multiple sclerosis), pain relief and management of anxiety or depression (e.g. serotonin and noradrenaline reuptake inhibitors [SNRIs] and tricyclic antidepressants [TCAs] in chronic nonmalignant pain) and pain relief and improved bladder management (e.g. TCAs in stroke).5 Some analgesics have side effects that may benefit particular patients. For example, tapentadol may minimise respiratory depression and is preferred for those with lung disease, and an oxycodone and naloxone combination minimises constipation in patients with diverticular disease in particular.
Assisting in functional outcomes
In cases of oversedation, analgesia reduction is often required to help patients to understand information or counselling delivered by therapists, such as therapeutic exercise or cognitive behavioural strategies for pain management, dietary advice to prevent further stroke or ischaemic heart disease and education on falls prevention. These nondrug techniques play a large role in helping patients to manage acute pain and any associated distress. Minimising sedation and optimising pain relief allows the patient to concentrate more easily so that therapy effectiveness is maximised.
Because co-ordinated multidisciplinary treatment is best practice in community-based ambulatory rehabilitation, GPs and rehabilitation therapists are encouraged to undertake multidisciplinary case conferences (supported by Medicare). These improve co-ordination of care and target analgesia in a more integrated way.6
Furthermore, better acute pain management prevents the risk of the development of chronic or persistent pain states. Education regarding catastrophisation, anxiety and fear associated with the pain, together with keeping pain levels at a minimum, can help in preventing the transformation of acute pain to chronic or persistent pain.7
Total knee replacement rehabilitation in the home
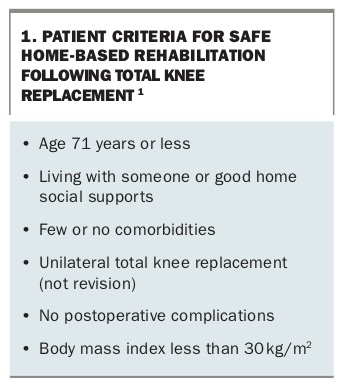
The population most likely to be referred for RITH comprises patients who have had a unilateral total knee replacement and who meet the other criteria in Box 1.1
{kind=link}
After total knee replacement, patients are often discharged on day five to eight, as soon as the surgeon is happy with the wound, has excluded venous thromboembolism and noted adequate range of movement for car travel. Discharge from hospital can only occur once the patient is able to transfer and walk independently to the toilet (and, if living alone, the front door) and the necessary safety criteria for RITH are met (social supports assessed, furniture heights assessed, toilet access safe and stairs able to be negotiated). The knee joint range should be at least 15 to 75° so the patient can sit on the toilet comfortably. A physiotherapist, occupational therapist and nurse should visit the patient at least three to five days a week for at least two weeks. The therapists and nurse will encourage mobility and safe transfers and monitor wound healing, analgesia and comorbidities.
Studies have shown that the use of NSAIDs and COX-2 inhibitors in the postoperative period speed the time for the joint to achieve a range of movement of 90° and decrease the need for opioids by 30% in the perioperative period.7,8 After joint replacement, patients have acute pain; therefore, the use of opioids for pain management in addition to nonopioids is appropriate. It is essential that a patient commenced on opioids is weaned safely within two to six weeks. It is the prescriber’s responsibility to ensure this is done.
Side effects of medications need to be monitored and correct patient selection is integral. Knee replacement surgery is mostly indicated for mobility, yet 25% of patients fail to make minimally important clinical gains by six months after surgery, 15% report moderate-to-severe pain and 20% report moderate-to-severe activity limitations at 24 months.9,10
Pain on movement
Pain on movement in rehabilitation requires an educational approach. Patients must be made aware that opioids are best at treating pain at rest and that pain on movement or ‘incident pain’ comes and goes so quickly that it is impossible to treat effectively within that time window. For example, the patient’s pain score might be four out of 10 at rest but increase to seven out of 10 during the two to three seconds taken to stand from a seated position. It might then settle back to four out of 10 once walking, but it is not possible to treat the increased pain during that activity. The best approach is to teach the patient to use distraction and to reassure them that the pain will be over quickly. Cognitive behavioural therapy techniques to prevent catastrophisation, distress and anxiety may also be beneficial. As the joint becomes more flexible, less swollen and less adherent to surrounding soft tissues, the momentary pain on rising is likely to lessen in intensity and duration. If opioids are titrated to the pain on movement, the patient’s pain on movement is not likely to be managed with medication alone and they may be mostly drowsy when at rest. A common practice is to give analgesia pre-emptively before movement such as a physiotherapy session or a walk to the shops, but there will still be pain on movement.
Patients also need to be made aware that because the joint has been removed proprioceptive information to the brain from the joint will be forever changed. Over six months, a knee-joint replacement will become so integrated that patients will not be conscious of the feeling of ‘otherness’ of that joint compared with their native knee joint.11 This is particularly important information for patients with peripheral neuropathy which occurs in about 25 to 50% of older patients; therefore, many are at high risk of falls before the arthroplasty.12 Therapy must focus on strengthening the quadriceps, an occupational home visit to minimise obstacles in the home and balance training to minimise falls risk.
Personalising analgesia
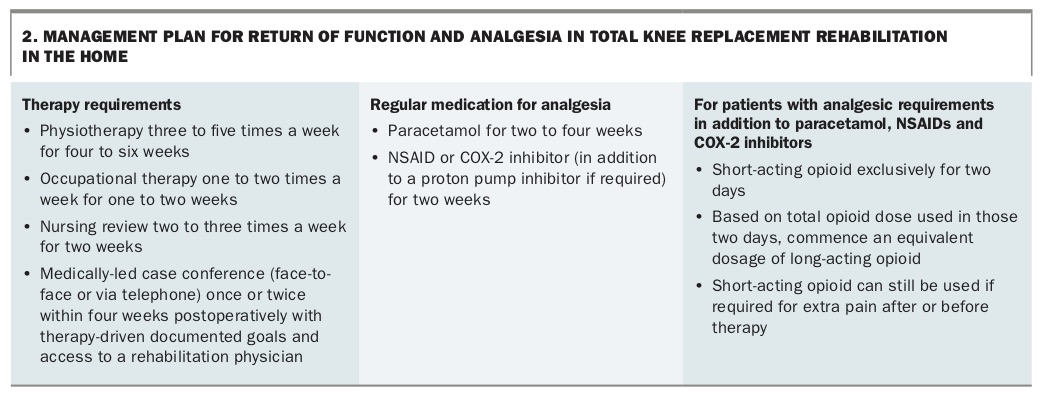
A typical personalised management plan for RITH for a patient with a total hip replacement is provided in Box 2. Paracetamol is the bedrock of acute pain management but the optimal dosage is still unclear. Best practice is to start patients with acute pain on paracetamol 1000mg four times daily or paracetamol modified release 1330mg three times daily. Patients with liver disease or renal disease need to have their doses modified. Paracetamol is not appropriate for patients with liver failure. Dose-for-dose, paracetamol in combination with an NSAID or COX-2 inhibitor confers better analgesia in the postoperative period than paracetamol alone and it is therefore often prescribed in combination.13
{kind=link}
A short-acting NSAID or COX-2 inhibitor is best (ibuprofen, celecoxib or diclofenac) so it can be used regularly over a one- to two-week period and as necessary for painful episodes in the future. Only patients with normal renal function and who have not had asthma or gastrointestinal bleeding should be considered for NSAIDs or COX-2 inhibitors. Renal function tests should be checked before commencing NSAIDs, and aspirin prophylaxis for ischaemia should be suspended while the NSAID or COX-2 inhibitor is used. For patients with previous symptoms of gastro-oesophageal reflux, proton pump inhibitors may be increased or commenced for the period of NSAID use, although the evidence for their continued use as protection may be minimal. If NSAIDs are used, aspirin needs to be stopped. If anticoagulants are used for venous thromboembolism prophylaxis then doses need to be small and a proton pump inhibitor should be used until the anticoagulant is ceased.
Opioids are the mainstay of medication in the acute postoperative period. Shorter-acting opioids are preferred for acute pain because their time of onset is faster than that of long-acting or sustained-release opioids. Long-acting opioids may have the advantage of offering patients a more convenient dosing regimen and fewer side effects such as constipation, nausea and drowsiness. Long-acting oxycodone with naloxone has the advantage of a limited risk of constipation and comes in low-dose preparations from 2.5/1.25mg (oxycodone/naloxone). Tapentadol causes less constipation and less respiratory depression. Buprenorphine can be used as a transdermal patch, delivering steady-state levels of opioid analgesia 24 hours a day for one week.
Some opioids, such as tramadol and tapentadol, are marketed for their profile in neuropathic pain. These drugs work on mu-opioid receptor agonists and noradrenaline reuptake inhibitors (this is a mode of action of TCAs and SNRIs) at the same time. Neuropathic pain is likely to be a contributor to the postsurgical pain state because nerve endings are affected by surgery. Tramadol and tapentadol are likely to have similar risks of side effects as other opioids; however, tramadol has an increased seizure risk and is relatively contraindicated in people with epilepsy.14,15 The oral morphine equivalent of 50mg of tapentadol is 20mg of morphine and of 50mg of tramadol is 10mg of morphine. These dual-acting opioids (like all others) may cause cognitive side effects. They also have fewer low-dose preparations, which means that careful dose titration in the elderly is required.
Best practice involves using a short-acting opioid within a multimodal analgesic plan. After two days, the short-acting opioid is often replaced by an equivalent dosage of a long-acting opioid for two to three weeks and then ceased or weaned over one to two weeks. A typical treatment plan is provided in Box 2.
Deprescribing
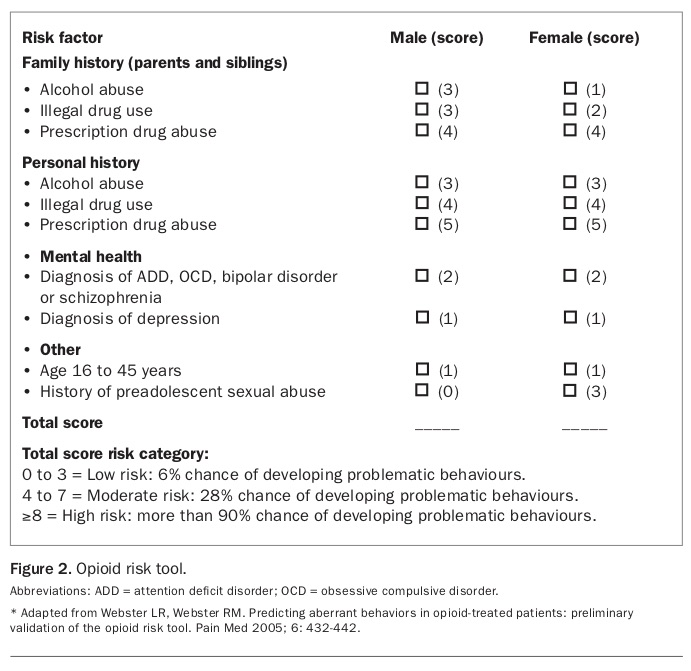
Short-acting opioids confer rapid-onset analgesia and anxiolysis, making them suitable for patients with acute pain. Dependence is unlikely to occur within a three-week period but caution must be exercised if prescribing them to patients with previous or current drug or alcohol misuse. A dependency risk tool, such as the Opioid Risk Tool, should be used to aid decision making regarding opioids for this population (Figure 2). For patients scoring seven or more, opioids should be avoided and alternative analgesia prescribed.
{kind=link}
For any condition, prescribing and deprescribing has now replaced the simple provision of a prescription for opioids. Evidence is clear that the long-term use of high-dose opioids is detrimental and harmful. It is conceivable that some may argue that prescribing opioids in the community setting without evidence of a deprescription plan may be considered inappropriate, unethical and poor practice. It is imperative that patients are followed up and opioids are reviewed and deprescribed appropriately. A suggested approach to deprescribing is provided in Box 3.
{kind=link}
Neurological rehabilitation in the home
Over the past 10 years, early discharge programs have become part of the discharge planning for mild stroke. Evidence shows that early discharge programs that incorporate co-ordinated RITH improve function, decrease mortality and improve quality of life.16,17 Nursing-only services do not confer these benefits. Furthermore, many of those under 65 years living with degenerative neurological conditions such as multiple sclerosis, Parkinson’s disease, traumatic brain injury or spinal cord injury will be supported in the home by the National Disability Insurance Scheme. This scheme often requires therapists and carers to visit the home and undertake home-based rehabilitation to encourage exercise or flexibility so that function can be maintained and return-to-work facilitated.
Stroke
Stroke patients with a Modified Rankin Scale score of zero to three may be discharged for RITH.17 Patients with moderate-to-severe stroke will usually be referred for inpatient or intensive outpatient rehabilitation. Pain in stroke survivors is usually associated with one of a number of conditions, including central poststroke pain, chronic nonmalignant pain that predates the stroke but is exacerbated by the disability, and hemiplegic shoulder pain.
The Modified Rankin Scale (available online at www.mdcalc.com/modified-rankin-scale-neurologic-disability) is a gross measure of disability but an inadequate measure of function; however, it is an accepted stroke outcome measure used internationally.18 It is simple to score and widely understood by neurologists, GPs and physicians. Patients who have no symptoms at all score zero. Patients who score one (‘no significant disability despite symptoms; able to perform all usual duties and activities’) often have nonvisible disabilities such as hemianopia, neglect, dysphasia, depression or cognitive decline, or very mild disability such as a poorly functioning upper limb and/or a foot drop. They are able to manage their affairs (social, leisure and work activities apart from driving). Those who score two (‘slight disability; unable to perform all previous activities, but able to look after own affairs without assistance’) are able to complete all activities of daily living but are unable to return to work and/or their leisure and social activities. This may occur with unilateral arm weakness, foot drop or cognitive impairment. Those scoring three (‘moderate disability; requires some help, but able to walk without assistance’) need some assistance with activities of daily living, and typically this is provided by family members or support workers.
Central poststroke pain
Central poststroke pain occurs in 8 to 55% of all stroke patients, depending on the definition of the pain syndrome.19 It is often associated with thalamic or insular cortex infarction or haemorrhage. Diagnosis relies on the distribution of the pain (hemianaesthesia and/or hemifacial) and the presence of allodynia or hyperalgesia.20 Evidence supports the use of education, cognitive behavioural therapy and TCAs (off-label) or pregabalin, gabapentin and other anticonvulsants. The anticholinergic side effects of TCAs (hypotension and urinary retention) should be considered, and both anticonvulsants and TCAs can cause fatigue, drowsiness and memory loss.
The PBS does not subsidise or offer free access to gabapentin or pregabalin, so in the first instance the GP can prescribe a night-time dose of amitriptyline 10mg, nortriptyline 10mg, imipramine 10mg or doxepin 10mg. The dose can be titrated every five to seven days with the aim of reducing the pain syndrome by 30 to 50%. Abolition of neuropathic pain is aspirational and most drug studies have shown significance only against placebo with a small or moderate effect size at best.21 Therefore it is unlikely that any drug will completely abolish neuropathic pain, and patient expectation should be adjusted accordingly. Other TCAs such as dothiepin can be considered. TCAs have a number of benefits for poststroke patients as they can assist in sleep, bladder storage overnight and anxiety management. Nortriptyline (the least anticholinergic), imipramine (the most anticholinergic), amitriptyline (the most sedative) and doxepin all have low-dose preparations (10mg) that allow careful dose titration, particularly in patients more than 75 years of age. The usual daily dose of a TCA for analgesic purposes should not exceed 50mg.
Seizures can occur after stroke in 7 to 14% of patients, with more severe strokes and haemorrhagic strokes conferring higher risk. For this reason, gabapentin or pregabalin might be the better first choice because TCAs marginally decrease seizure threshold. It is best to use the low doses of either drug (gabapentin 100 mg three times daily or pregabalin 25mg twice daily) and slowly titrate up to effect or side effect. The most concerning side effects are drowsiness, weight gain and memory impairment.
Pregabalin works within 72 hours, and gabapentin can take a week. For these reasons it is important not to increase dosage increments too quickly.
Chronic nonmalignant pain
Chronic pain that pre-existed the stroke, such as chronic lower back pain or neck pain, may be exacerbated by the change in gait brought on by the stroke. This type of pain often responds to psychoeducation, exercise and simple analgesia such as paracetamol or brief periods (up to two weeks) of opioids. NSAIDs and COX-2 inhibitors are relatively contraindicated in cases of cerebral haemorrhage (particularly in the first six weeks) and interact with warfarin, the nonvitamin K antagonist oral anticoagulants and antiplatelet agents. Again, the responsibility for deprescribing remains important for the prescriber. The effectiveness of physiotherapy and occupational therapy in these cases cannot be underestimated.
Hemiplegic shoulder pain
Hemiplegic shoulder pain occurs in about 10 to 30% of stroke patients and is most commonly reported at four months poststroke.22 It is complex to assess and may be associated with either a shoulder subluxation (weak shoulder girdle muscles letting the humerus hang down from the glenoid fossa and putting the biceps tendon on stretch and/or tonic contraction) or spasticity of the pectoralis, levator scapulae and/or subscapularis muscles.
If the shoulder is noted to be weak and subluxed without any pain then preventive treatment before the development of pain may be instituted. This includes functional electrical stimulation for four to six hours a day, which may be commenced in association with physiotherapy-supervised strengthening exercises. The physiotherapist or occupational therapist needs to show the patient how to use the functional electrical stimulation device, including where to place the electrodes. Firm supports and shoulder strapping may be used to protect the shoulder, and physiotherapy or occupational therapy may be commenced to improve or maintain function.
Patients with pain are assessed to determine whether there is a painful arc or pain on external rotation in adduction, or both. During active and passive abduction, note the degree of abduction when the patient reports pain and whether this is associated with facial grimacing. Then assess pain in external rotation in adduction and abduction by passively ranging the joint and noting the degree of external rotation when pain is reported associated with facial grimacing. Pain only on abduction may be associated with a rotator cuff tear, and pain on both abduction and external rotation is likely to be due in part to an adhesive capsulitis (frozen shoulder). However, if the shoulder is difficult to move due to tightness of the pectoralis muscle and pain occurs at the start of the movement, then testing arm tone or the presence of clonus in the upper limb will help diagnose whether the pain is also associated with spasticity.
An assessment and treatment plan for hemiplegic shoulder pain is outlined in the Flowchart, and detailed management according to the clinical findings is as follows.23
- Weak, subluxed and painful on external rotation. Shoulder pain that is due to adhesive capsulitis can be diagnosed by ultrasound or MRI. Education regarding the prognosis (which can be between one and four years, with most improving early) and a trial of paracetamol, an NSAID and/or opiate with an ultrasound-guided corticosteroid injection into the glenohumeral joint may be of assistance.
- Weak, subluxed and a painful arc. Once pain has commenced in abduction associated with weakness, paracetamol, an NSAID or a COX-2 inhibitor (contraindicated in cerebral haemorrhage and for those on anticoagulants) could be commenced for a short period (one to two weeks) with the suspension of the use of aspirin during this period. Alternatively, brief periods of opioid use may be appropriate. In patients who are in severe pain and unable to take NSAIDs or opioids, an ultrasound-guided suprascapular nerve block may be undertaken. If the pain does not settle within one to two weeks an ultrasound of the shoulder will help in the diagnosis of any associated rotator cuff tear or subachromial bursitis. In these cases, the addition of an ultrasound-guided subachromial injection of local anaesthetic with or without a corticosteroid may be of assistance.
- Spastic shoulder. If the upper limb has increased tone, with or without clonus, lioresal (5 to 10mg three times daily) or dantrolene (25mg twice daily only when liver function tests are normal) may be suitable. Best practice is referral to a spasticity management clinic where botulinum toxin may be used to manage pain and stiffness, followed by outpatient rehabilitation for stretching of the limb and training function.
Conclusion
Increasing numbers of patients will be referred for RITH, and GPs may be required to manage a patient’s analgesia during the rehabilitation process. Collaboration with a rehabilitation physician may be useful to establish a multidisciplinary treatment plan and undertake case conferences. Pain related to stroke and knee replacement should be managed according to its likely causes, the course of the pain syndrome and available resources. Management should always include analgesia, exercise and education. MT