Sexual health risk assessment in adolescents and young people

Adolescent health
Undertaking a sexual health assessment in adolescents and young people remains a daunting task for many GPs. Being prepared and having a clear framework for assessment helps GPs to be effective in supporting young people to achieve optimal sexual health.
Note
A comment on this article was published in the April 2019 issue of Medicine Today. The online full text and PDF versions (see link above) of this article have been updated.
- Good sexual health includes freedom from sexually transmitted infections, unplanned pregnancies, sexual coercion and discomfort (physical or psychological) related to a person’s sexuality.
- Adolescents and young people are the group most at risk of poor sexual health.
- Good access for testing and treatment, with appropriate education and health literacy and support are important factors in improving the sexual health of young people.
- GPs are well placed to provide adolescents and young people support with regard to their sexual health.
- Effective sexual history taking is the first essential step in helping adolescents and young people achieve optimal sexual health.
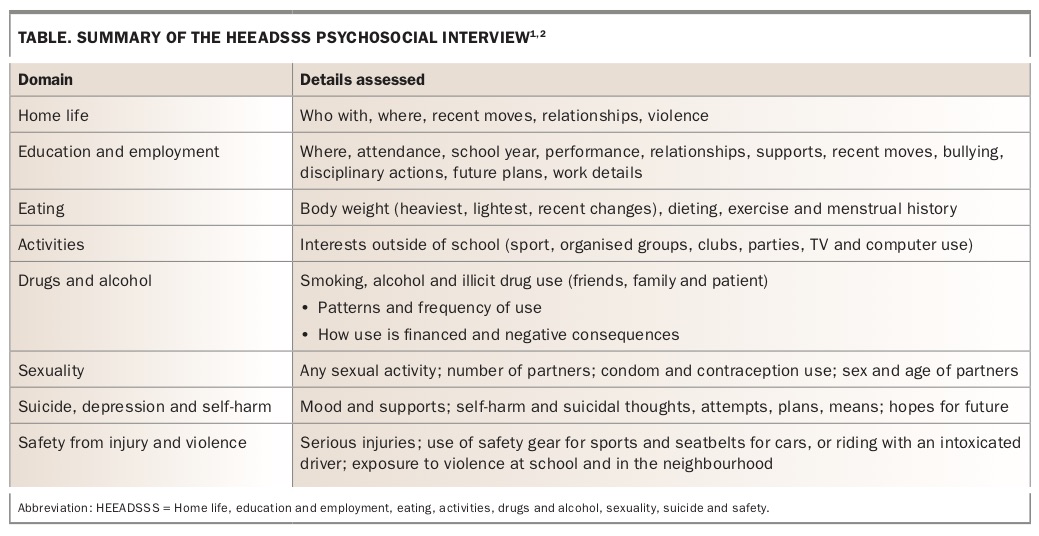
A sexual health risk assessment is a crucial part of assessing the overall health and wellbeing of a young person. It is designed to identify sexual and other risk-taking behaviours and psychosocial issues. Such an assessment assists in determining the risks of sexually transmitted infections (STIs), unplanned pregnancy, sexual coercion and discomfort (physical or psychological) related to the person’s sexuality. In essence, it involves taking a thorough sexual history and using an adolescent screening tool known as the HEEADSSS assessment that covers home life, education and employment, eating, activities, drugs and alcohol, sexuality, suicide and safety (Table) and is available in full at www.contemporarypediatrics.com/modern-medicine-feature-articles/heeadsss-30-psychosocial-interview-adolescents-updated-new-century-fueled-media.1,2 However, this essential assessment is not always performed because of many barriers. In this article, we aim to provide an overview of the essential components of a sexual health risk assessment for young people aged 12 to 24 years.
{kind=link}
Why it is important to speak to young people about sex
Adolescents and young people have quite limited access to reliable resources related to sexual health. Despite apparent health literacy and ready access to information online, many young people remain ill-informed regarding both pregnancy and the risks of contracting STIs. Adolescents and young people are often more inclined to engage in sexual risk-taking behaviours than other age groups. Accordingly, they remain vulnerable to STIs, unplanned pregnancies, unwanted or regrettable sex and the potential mental health impacts related to sexuality. GPs are well placed to provide both trusted information and practical assistance.
The sexual health assessment: getting the basics right
The setting
GP’s rooms that are adolescent friendly can help young people feel more comfortable. One way to do this is simply by displaying health education posters and pamphlets that are relevant to them. It may help to find out when young people are likely to use the clinic, such as on the way to school or university, and make convenient appointment times available to them.
A young person will better engage if the GP uses open, clear communication, avoids medical jargon and uses common day-to-day language. GPs could make it routine to see adolescents and young people initially with parents or guardians present and then tactfully ask to see the young person alone. Practice helps, so if this is done for less-confronting consultations such as sore throats it will begin to feel natural to the doctor and the patient.
Establish confidentiality
How confidentiality applies in this context should be established early on, including the limitations to confidentiality. Young people are often particularly concerned that their parents will be told about the consultation. It is worth addressing this concern directly (a more detailed discussion of ‘Gillick competence’ can be found below).
Preparing an example of what to say and practising so that it comes naturally and in a nonconfronting manner is helpful. An example of what to say is: ‘Everything that we talk about here today is confidential, that means that I won’t speak to anyone else, like your parents, about the stuff we talk about unless you want me to. There are three exceptions to that rule. Firstly, if I think that you are at risk of hurting yourself; secondly, if I think there is a risk that you will hurt someone else; or thirdly, if I think you are at risk of being harmed by another person. Even if I do have to tell another person about what we’ve talked about, I’ll always talk to you first and try to come up with a plan that we are both happy with. Is that ok?’
Phrase questions carefully
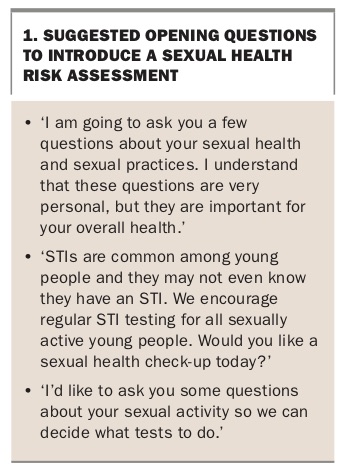
Bridging questions can be helpful. For example, the more general lifestyle questions in the HEEADSSS assessment could be used first. Box 1 provides some suggested ways of introducing questions about sexual health. When moving on to sexual history, first ask the less confronting questions, such as ‘How long have you been sexually active for?’. Normalise without making assumptions, using questions such as ‘Are you seeing anyone at the moment?’, ‘Are you sexually active with this person?’, ‘Is this the only person you are seeing at the moment?’.
{kind=link}
Try to establish the young person’s sexual orientation. We advise keeping this question simple, such as: ‘Do you have sex with men or women or both?’ Keep in mind that some young people may be feeling confused, embarrassed or guilty about their sexuality. It is best never to assume you have correctly identified a young patient’s sexuality. An innocent question such as ‘So, do you have a girlfriend?’ asked of a young man who is attracted to men may make it difficult to establish an effective relationship. Further, it is helpful to avoid the assumption that everyone means the same thing by ‘sex’. We recommend keeping terminology open, such as ‘any form of sexual contact’, as some people may consider oral sex or mutual masturbation to be sex.
When and how often to talk about sex
The realities of a busy general practice preclude undertaking sexual health risk assessments with all adolescents and young people at each consultation. It is, however, a must for patients presenting for contraceptive needs, STI screening, urogynaecological problems and mental health problems. Travel consultations may also be opportune times to raise the issue of sexual risk-taking behaviour.
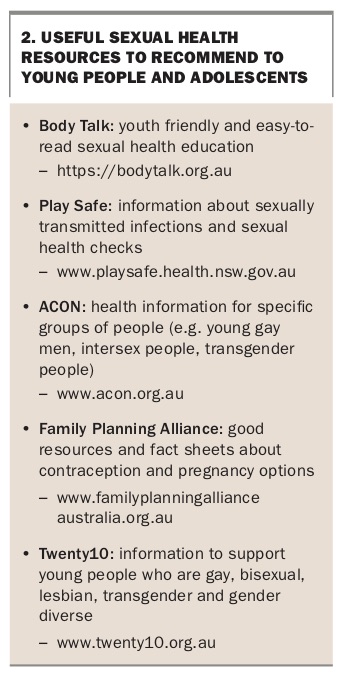
In a busy clinic setting it is useful to be able to refer patients to reliable, youth-friendly and informative websites. A list of resources that could be recommended to a young person can be found in Box 2.
{kind=link}
Common barriers to taking an appropriate sexual history include time restraints, lack of confidence, not wanting to embarrass the patient and fear of intrusion. Age, sex and cultural background of the patient relative to that of the GP may also present a barrier to the patient disclosing their sexual history. Lines of enquiry regarding sexual coercion, unwanted sex or assault may often be avoided because of a GP’s lack of confidence in managing the outcomes of such enquiries.
It might be advisable for GPs to first examine their own comfort levels, beliefs and biases. If, for example, the GP feels uncomfortable taking a sexual history then the patient is unlikely to feel comfortable either. A useful strategy is to keep questions matter-of-fact and in simple language, and practice them. Rehearsing in a mirror or role playing with a colleague or supervisor can help normalise the issues that need to be discussed with the patient. Due to their cultural or religious background, a doctor may hold beliefs about sex, pregnancy or sexuality that preclude a nonjudgemental and helpful sexual health consultation. In such instances, referral to another GP or health professional is advisable.
Consent and the GP’s responsibilities
It is important to know and understand the relevant state laws governing consent. Information about the age of consent to sexual activity in each state and territory of Australia is available on the Australian Institute of Family Studies website (https://aifs.gov.au/cfca/publications/age-consent-laws) as well as comprehensive information about mandatory reporting of suspected sexual abuse of a minor, which also varies slightly from state to state (https://aifs.gov.au/cfca/publications/mandatory-reporting-child-abuse-and-neglect).
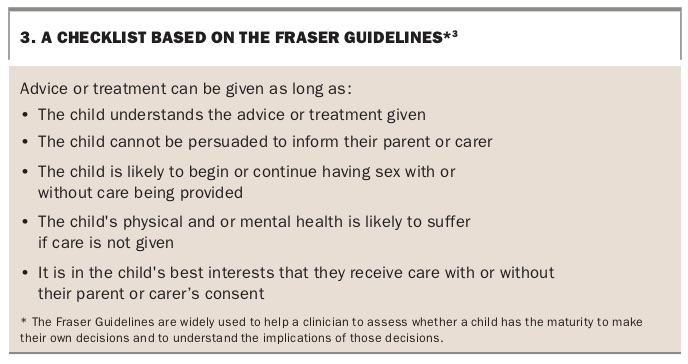
When providing sexual health advice to a person under 16 years of age, be it providing contraception advice or advising on STI management, it is best practice to follow the Fraser guidelines (which classify the young person as ‘Gillick competent’ or not).3 A useful checklist derived from the guidelines is provided in Box 3. It can be helpful to keep a record of the responses to this checklist in the patient’s clinical notes. As long as it has been assessed and recorded that the young person is ‘Gillick competent’, the doctor can, for example, prescribe an oral contraceptive pill.
{kind=link}
Screening young people for STIs
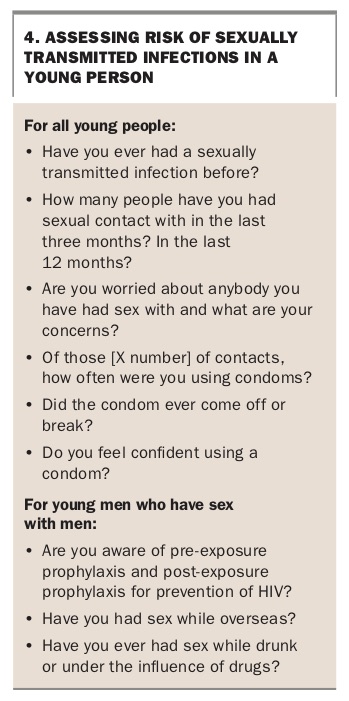
Important questions to ask when assessing the risk of STIs in a young person are listed in Box 4. These include questions about frequency of sexual contacts and condom use. Young people may feel embarrassed to admit that they do not feel confident using condoms. A helpful website to refer young people to is Body Talk (https://bodytalk.org.au). Often young people are frightened of what is involved in an STI screen, but a simple explanation can quickly allay this fear.
{kind=link}
The NSW Sexually Transmissible Infections Program Unit (STIPU) Testing Tool provides a clear summary of what to test for, how to test, the required frequency of testing and how to trace contacts.4 This testing tool is consistent with the Australian STI Management Guidelines, and although designed by NSW Health it can be adapted for clinicians nationwide.
All sexually active young people should have annual chlamydia testing. In young women testing of a self-collected vaginal swab or a first-void urine sample is preferable. In young men a first-void urine should be collected. It is important to determine a young person’s immunity to hepatitis B if their immunisation history is unclear. HIV and syphilis serology should be performed according to the young person’s risk and the local HIV and STI prevalence. Additional testing is required in young men who have sex with men. This includes testing for gonorrhoea, chlamydia, syphilis and HIV at least annually, with the frequency based on the person’s risk. Testing involves collecting swabs for polymerase chain reaction testing for rectal gonorrhoea and chlamydia, urine chlamydia and throat gonorrhoea. It is also important to establish the person’s immune status with regard to hepatitis A and hepatitis B viruses.
Underuse of effective contraception
Many young people continue to use either no contraception or unreliable means of contraception including the withdrawal method (used by 10% of Australian young people).5 Most pregnancies in adolescents in Australia are unintended, and about half of these pregnancies are terminated.6 Teenage pregnancy is of significant concern due to the associated poorer health, educational and socioeconomic outcomes in the mothers and children.5
Appropriate contraceptive and sexual health counselling can reduce these poor health outcomes by identifying those at risk and reducing the rate of unplanned pregnancy. Provision of brief, simple information regarding effective contraception methods, correct condom use and where to access condoms and emergency contraception can help reduce unplanned pregnancies. Family Planning Alliance Australia (http://familyplanningallianceaustralia.org.au) has excellent online resources for GPs and patients.
Defining sexual coercion
The term sexual coercion encompasses a range of scenarios where one person feels uncomfortable or uncertain about what they are doing. It occurs when a person feels pressured into not using a condom, or ‘stealthing’, where one person removes a condom without the other person’s knowledge, right through to sexual assault. Sexual coercion often results from an imbalance of power between the two people, for example due to a significant age gap.
About 20% of Australian women over 15 years of age have experienced sexual violence. The number of people in Australia experiencing sexual coercion over the past few years has remained static, as has the number of people seeking help for this.7 Drug and alcohol use and inexperience are risk factors for sexual risk-taking behaviour. Alarmingly, unwanted sex is reported by almost one-third of sexually active young women in year 12.5
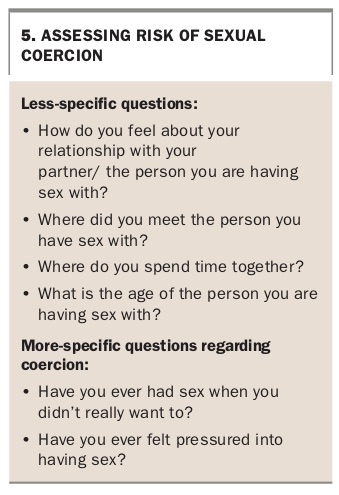
Identifying and assisting young people who have experienced sexual coercion can be challenging. Box 5 gives some examples of questions to ask to identify risk of sexual coercion.
{kind=link}
What to do when a young person discloses nonconsensual sex
Discovering that a young person is or has been coerced into unwanted sexual activities can be a confronting and at times frightening experience for many GPs. It is important for the GP to remember they are not alone and that in most situations they do not need to come up with all the answers in one consultation. It is important to establish what the young person wants to happen and what their main concerns are.
Familiarity with the relevant state laws is important as they may vary from one state to another. The following services offer further assistance:
- local sexual health centres
- Family Planning Australia
- child protection units
- local sexual assault teams.
The Flowchart summarises the above steps for assessing sexual health in adolescents and young people.
Awareness of same-sex attracted young people
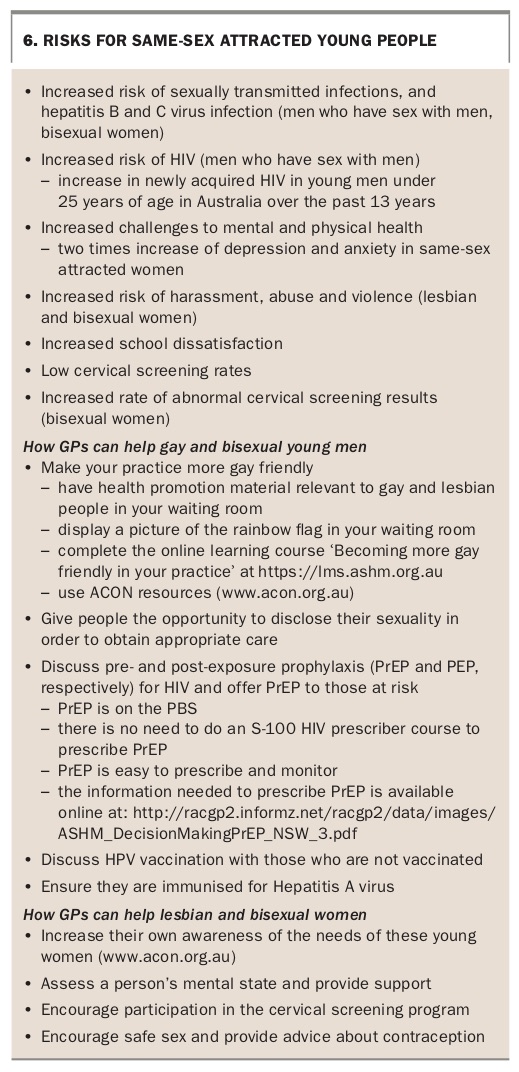
Same-sex attracted young people often face additional challenges, including increased rates of mental illness and attempted suicide. Discrimination can lead to higher rates of anxiety, depression and sexual risk-taking behaviour. Same-sex attracted young people are more likely to commence sexual activity at a younger age and have sex without a condom, and hence are more likely to acquire STIs.7 Pregnancy is twice as likely in same-sex attracted women who have sex with men then in heterosexual women. Discrimination and feelings of isolation and lack of support are higher among those who are same-sex attracted and living in regional and remote areas. Extra consideration needs to be given to these groups of young people. Box 6 gives a brief summary of additional important considerations and ways in which GPs can assist same-sex attracted young people.
{kind=link}
Conclusion
Overall, undertaking a sexual health risk assessment of a young person is essential to ensure optimal health care. Engaging with a young person is key, and developing competence in this in general practice is essential. Being open and comfortable with questioning will help the young person feel comfortable and be honest with their responses. Although the assessment outlined above may appear time-consuming, with practice it can be completed in just a few minutes for most patients and more complex cases can be managed over several consultations. MT