Practitioner obligations to follow up recommended tests and referrals

Medicolegal medicine
This series highlights common medicolegal issues in general practice. Written by a team from medical defence organisation Avant, the scenarios are based on a range of previous cases with details changed for privacy and some issues summarised for discussion. In this scenario, a medical clinic is sued by the family of a patient who died after a failure to follow up pathology testing and specialist referral.
A medical practitioner’s obligation to follow up on a patient’s care may continue after the patient leaves the consultation. When doctors order tests because they are concerned about a potentially serious clinical condition, they should monitor whether the patient has had the test. If failure to follow up clinically significant tests leads to patient harm, the medical practitioner may be found negligent or guilty of unsatisfactory professional conduct.
However, medical practitioners are often unsure how far they need to go in following up patients for return appointments, review of test results and specialist referrals. They may also be concerned whether the need to ensure patient privacy limits what they can do to follow up patients.
The following scenario, based on a case with details changed for privacy, describes a patient who died after failing to return to a GP clinic for a pathology test and specialist appointment. The patient’s family brought an action against the medical clinic and GP for negligence. The outcome of the case and recommended systems for patient follow up, recall and reminders are discussed.
Case scenario
Patient history
Mr Green presented to a regional GP clinic in early March complaining of chest pains. Dr Jones examined the patient and satisfied himself this was not an acute problem. Mr Green had a significant family history of myocardial infarction in his father and brother at ages 42 and 40 years, respectively. He was also a smoker and had hypertension. Dr Jones therefore arranged for him to see a visiting cardiologist at the clinic three weeks later and to undergo a fasting cholesterol test in the interim.
Mr Green did not return for the test or the specialist appointment. He subsequently saw several other doctors at the clinic for other complaints but did not mention the original issue. The practice management system relied on the next practitioner seeing the patient to pick up any nonattendance. Patients who failed to attend a specialist appointment would usually have a new appointment made for them and a new appointment card sent out. Because of an administrative error, this process was not followed for Mr Green. As no-one at the clinic noticed that the test and specialist appointment had been missed, they were not followed up.
The following January, Mr Green had a heart attack and died. His family claimed that the clinic was negligent in failing to ensure that Mr Green’s treatment was followed up.
Legal issues
Both the GP and the clinic owed a duty of care to Mr Green to exercise reasonable care and skill in the provision of services to him. In the case of the clinic, that duty included a requirement to exercise care and skill in the administration and management of treatment provided by the medical practitioners who worked there.
In deciding whether that duty was breached, the court has to consider whether a reasonable person in the position of the defendant (in this case the GP and the clinic) would have foreseen that their conduct involved a risk of injury to a person in the patient’s position. If so, the question then becomes what a reasonable person would have done by way of response to the risk.
Discussion
As Justice Forrest of the Victorian Supreme Court explained in a 2012 decision on the issue of patient follow up the court needs to consider ‘what was reasonable in the circumstances, not what might be the perfect medical practice, particularly when viewed with the advantage of hindsight’.1 For example, a standard of perfection might require a practice to have a system that recalls any patient who fails to re-attend for any results, undertake an ordered test or follow up on a referral. However, this would not be reasonable.
In determining what is reasonable, the court will rely on expert testimony and will be guided by any applicable standards or guidelines. For example, guidelines from the Australian Medical Association (AMA) and the Royal Australian College of General Practitioners (RACGP) provide important evidence of the appropriate standards.2,3
The AMA position statement on Patient follow-up, recall and reminder systems - 2013 states that ‘to facilitate safe, good quality care, appropriate systems must be in place to ensure that pathology, radiology, and any other investigative tests and/or referrals are properly initiated, acted upon, and the results communicated in a timely manner’.2
The AMA position statement also states that ‘while not every test or referral needs to be confirmed, if there is a reasonable suspicion of a clinically significant outcome, then the doctor has a duty to attempt to follow up and recall the patient’.2
The RACGP standards for general practices outline the expectation that practices will have processes for appropriately managing results, recalls and reminders.3 Recommendations on systems to manage test results are shown in Box 1.3,4 The key question in determining what level of response is appropriate is whether the results are ‘clinically significant’, which the AMA position statement explains as a situation where the patient may be at serious risk of harm if medical advice is not obtained.2
{kind=link}
Setting expectations
Initially, it is important to make sure that the patient understands the reasons for the test or referral appointment, and the importance of attending for it and of following up the results. This is particularly important for new patients as different medical practices may have different systems for notifying results. However, even for regular patients and regular or routine tests such as cervical screening tests, it is important to check that the patient knows whether someone from the practice will call them, whether they will receive a letter, text message or other correspondence telling them whether they need to take any further action, or whether they need to call the practice for their results.
This is also a good time to ask the best way to communicate with the patient about any follow-up care. Even if your practice routinely checks for changes to patient address details, it is a good opportunity for medical practitioners to double check the details and confirm whether the patient is happy for you to leave a message on the phone number provided, particularly if their contact details are a home phone number. It is also prudent to check specifically whether the patient can be contacted via text message.
It is recommended that medical practitioners document in the patient’s clinical record what they agreed with the patient about follow up and the method of contact.
Tracking tests and referrals
It is important that all test results received by the practice are reviewed, actioned where required and incorporated into the patient health record (Box 1).2-4 The practice’s process for tracking tests should also make it clear what happens for clinically significant tests when a patient does not present to undergo the test within a specified timeframe, when results are not received, or when the patient does not attend the practice to discuss results within a specified timeframe.
The process should also allow for tracking of clinically significant referrals. If there are particular circumstances, for example the GP feels the patient needs early review, it may be worthwhile asking the patient if they would like the GP to make the appointment for them. This allows the GP to determine whether the next available appointment is within a suitable timeframe to ensure appropriate assessment.
Problems can arise when results ‘fall through the cracks’, for example because someone was away or failed to follow usual practice. Whatever tracking system is implemented, it is important that everyone working in the practice, including temporary and locum staff, understands the system and also the processes to check results for doctors who are away, on holiday or no longer working in the practice.
How far should you go to contact a patient?
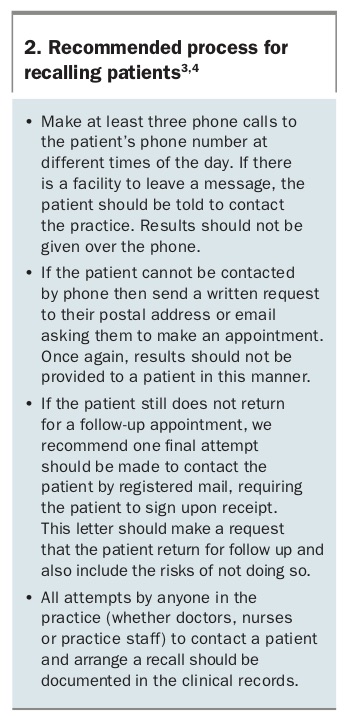
In the case scenario described above, Mr Green did return to the practice, but his missed test and appointment were not raised with him. However, it is also important to have a process for recalling patients who do not return to the practice. A recommended recall process is shown in Box 2.3-4
{kind=link}
Use of text messaging
Although the question whether practices can communicate with patients via text message did not arise in Mr Green’s case, it is increasingly relevant, particularly with younger patients.
Communicating with patients via text message should be treated in the same way as leaving a voicemail or sending an email.3,5,6 The message should be short and should confirm that the patient is to make an appointment with the practice; no results should be provided via text message.
Before sending any text messages to patients, practices should follow the following steps.
- Have a text messaging policy that covers:
— who is authorised to send, receive and respond to text messages
— how messages are included in electronic health records
— what information is to be included in the text message
— how consent is to be obtained and documented
— what checks are made to verify that the mobile number of the patient is up to date. - Obtain and document consent. Just because a patient has provided their mobile number, it does not mean that they consent to receiving text messages from the medical practitioner.
- Limit information that is contained in a text message. Text messages should not contain sensitive information.
It is important to remember that text messages form part of the clinical record. This also extends to text messages that are exchanged between doctors about a patient’s care.
Text messages should ideally be sent from a practice number rather than from a medical practitioner’s personal mobile. Also consider the time of day that text messages are sent, to ensure professional boundaries are maintained between medical practitioners and their patients.
Outcome
In the case of Mr Green, the court considered it was foreseeable that patients would fail to keep appointments or attend for tests and that the practice had a responsibility to put in place administrative procedures to address a situation such as the one that arose with Mr Green. The practice was negligent in failing to have a system in place to flag any nonattendance and to ensure that patients were followed up.
Dr Jones also had a duty of care to the patient. However, in this case the court considered that because of the way the practice administration was set up, Dr Jones was not responsible for following up the tests himself and was not negligent in his treatment.
The court also found that Mr Green’s own failure to follow medical advice had equally contributed to the outcome. The court therefore ordered a 50% reduction in damages for Mr Green’s contributory negligence.
Conclusion
Practices must take all reasonable steps to attempt to recall their patients. It is not enough to rely on patient autonomy. Further, it is important that medical practitioners ensure their patients understand the need for a test that has been ordered and the follow-up procedure at the practice. This will help eliminate any confusion about who is responsible for their recall. MT