‘He grabbed my neck and choked me’. Another case of nonfatal strangulation

Patients injured in domestic violence incidents sometimes receive care in an emergency department; however, often abuse is not reported because it does not occur in public and also often leaves no obvious signs of injury. It is recommended that GPs screen patients for unsafe relationships.
As a GP in Australia, you are aware of the significant level of domestic violence that occurs, particularly against women, with one in five women disclosing family or domestic violence for the first time to a GP.1,2 You are aware that the COVID-19 pandemic stressors are increasing alcohol and mental health problems and domestic violence.
Case study
One evening during a shift in the local emergency department (ED) a distraught and crying 43-year-old woman is brought in by ambulance paramedics on a stretcher, accompanied by her sister.
The patient is triaged as a trauma patient, triage category 2 (to be seen within 10 minutes). She is brought into the resuscitation cubicle, and you are part of the trauma team that will attend her, assigned as the ‘procedures doctor’ and responsible for intravenous lines and similar.
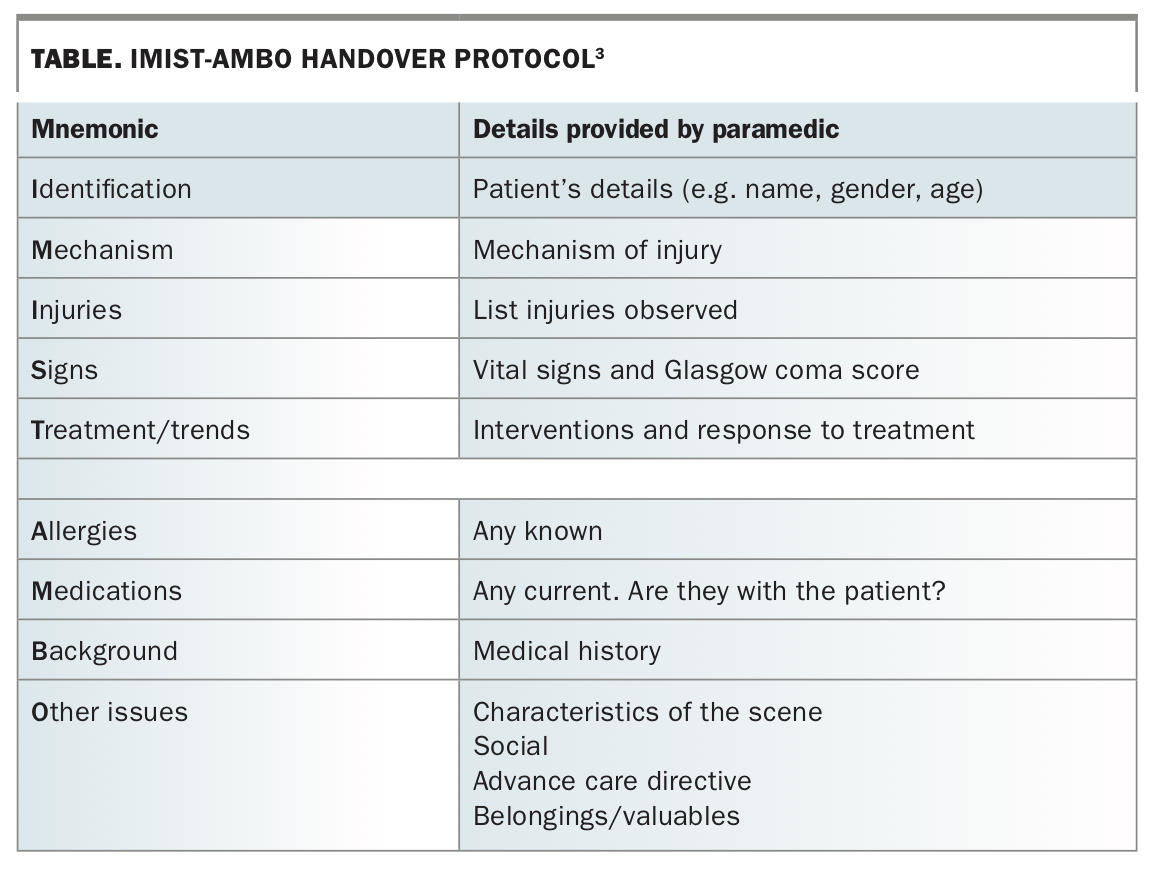
The trauma team leader, the ED consultant, calls for quiet so the paramedics can give the essential handover using the ‘IMIST-AMBO’ mnemonic (Table).3
{kind=link}
The paramedics report the patient had been assaulted at a party by her intoxicated defacto partner, who had grabbed her with both hands tightly around her neck, choking her, pushing her to the ground and repeatedly shaking her head, with it striking the floor. Bystanders at the party had tackled and restrained the assailant and called the police and an ambulance.
The paramedics’ major concerns are regarding the patient’s airway, as she is hoarse and there is redness and developing bruising visible on her neck and a palpable posterior scalp haematoma. Her respiratory rate is 26 breaths per minute, oximetry 98%, pulse 118 beats per minute and blood pressure 152/96 mmHg. She had briefly lost consciousness (for 30 to 60 seconds), although her Glasgow Coma Scale score is now 15/15. Treatment included a cervical collar, spine board, intravenous line and oxygen by a nonrebreather mask.
The patient has no known allergies, is not taking any medications and has no background medical history. She has three children from a prior relationship.
The scene of the assault was a ‘wild’ party with high alcohol consumption and probably drug taking. The patient was in an abusive relationship with her defacto partner and they had been arguing loudly before the assault. Her partner had recently lost his job. He was taken into police custody.
Examination and investigations
There may be few obvious signs of any injury in cases of domestic violence. Even nonfatal strangulation (NFS) is reported to have no signs in 50 to 70% of cases. Often it leaves no obvious signs of the injury, explaining why it often goes unreported.2
In this patient, however, there are signs, leading to several serious concerns:
- airway, compressing haematoma, larynx injury
- vascular injury, especially carotid artery dissection
- head injury, intracranial bleeding
- possible cervical spine injury, hyperextension.
On examination, secondary survey, there is unexplained bruising of the limbs and abdomen at varying stages of healing, consistent with physical violence. Consultations with the relevant specialty teams are organised, as well as investigations, including head and neck CT and cervical angiogram (MRI is not available).
Management and outcome
Further distress for the patient is minimised by the senior ED clinician and urgently attending social worker taking over her care. Also, the patient’s sister, with the patient’s permission, is constantly by her side.
The patient is admitted and reassured repeatedly about the safety of her children, who are now with another relative. No significant abnormality is found on imaging. She is discharged two days later, after safe accommodation has been ensured and detailed and active follow-up arrangements have been made, including written information and support regarding what to do next and further police, legal and court processes (e.g. VWCCS [Victims and Witnesses of Crime Court Support]).
Debriefing and education
This case is upsetting to many of the hospital staff. A debriefing and education session is held, which you attend and find helpful.
Discussion
The pathophysiological effects of strangulation have not been well studied.4 There are several mechanisms, including cerebral hypoxia and arterial and venous obstruction. Also, there can be compression of the carotid arteries against the transverse processes of C1 to C3.5
The extent and severity of domestic violence and nonfatal strangulation (choking) are significant:
- one in four women in Australia experience domestic violence1
- nonfatal strangulation is a strong predictor of a high rate of future death2
- if a person survives nonfatal strangulation, they are then
– over six times more likely to become an attempted homicide victim
– around seven-and-a-half times more likely to die at the hands of the perpetrator.2
Of people with a blunt cerebrovascular injury, 25 to 50% first develop signs (e.g. strokes, seizures) more than 12 hours after the injury and some develop signs even later.4 Brain injury overall is poorly recognised and underreported.6 Anger, oppositional behaviour or forgetfulness are commonly due to brain injury rather than personality or other causes.7
The psychological consequences of domestic violence include anxiety, depression, substance abuse, eating disorders, post-traumatic stress disorder, sleep disorders, low self-esteem, fear of intimacy and family and social problems.7
A sensitive approach to the patient in the acute setting is vital. Judgemental phrases such as ‘domestic violence’ should be avoided, and open-ended questions should be used, for example, in asking the patient about being hurt. Repeated medical ‘interrogation’ by numerous health professionals, which is distressing, can be avoided by appointing one or two senior people to oversee the patient’s care
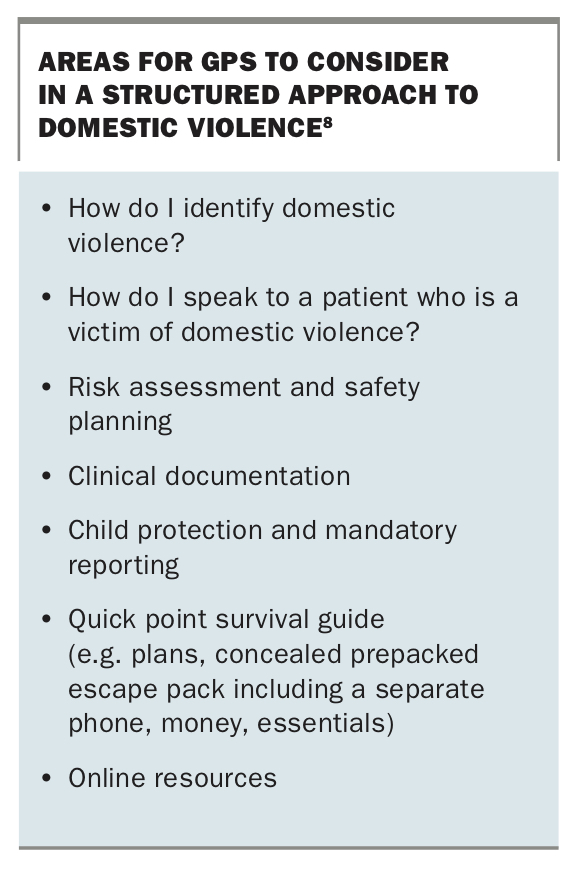
In the ED, GPs are crucial points of contact for people who have experienced domestic violence, and being prepared with a structured and practical approach is essential (Box).8 GPs can provide support; refer for psychological support; ensure the patient has safe places to be, supporting people and shelter contact details; and advise about support for children.
{kind=link}
The presence and assistance of a social worker, especially one with domestic violence skills, is also invaluable. Most important is that the woman leaves the department feeling validated, supported and with active follow-up services in place.8 It is important to allow time to achieve this, and ED medical and nursing staff are generally too time-poor for this.
Screening is recommended; mandatory screening has variable effectiveness.9
There are many screening tools available. The ‘SAFE’ mnemonic is a reminder for a simple set of questions:
- Stress/Safety – Do you feel safe in your relationship?
- Afraid/Abused – Have you ever been in a relationship where you were threatened, hurt or afraid?
- Friends/Family – If you were hurt, would your friends and family be aware of it and able to provide support?
- Emergency – Do you have a safe place to go and the resources you need in an emergency?
Conclusion
Understanding the prevalent extent and severity of domestic violence, and in particular nonfatal strangulation, in the community alerts GPs to the importance of screening patients for unsafe relationships and being prepared with strategies for providing immediate support and active follow up for those who report abuse. Familiarity with the short and long-term signs of brain injury and psychological trauma helps guide effective treatment and referral. Skill and compassion in approaching patients who have been harmed by someone close to them minimises further risk and distress. MT
If this article raises issues for you, help is available by calling:
1800RESPECT
Aboriginal Family Domestic Violence Hotline 1800 019 123
Kids Helpline 1800 55 1800
Lifeline 13 11 14
Men’s Referral Service 1300 766 491
Relationships Australia 1300 364 277
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.