Domestic violence. What is the role of the GP?

Family, domestic and sexual violence is a major health and welfare issue in Australia. By being responsive to patient presentation and behaviour, GPs can play a pivotal role in the health response to domestic violence. An awareness of how to respond appropriately can help GPs provide the best support and advice for patients affected by domestic violence.
Family, domestic and sexual violence is a major health and welfare issue that occurs across all ages, and socioeconomic and demographic groups worldwide. It can affect people in heterosexual or same sex relationships and predominantly affects women and children.
Extensive research indicates that violence, abuse and neglect have serious impacts on health.1 These include physical impacts such as acquired brain injury, disability, chronic disease and, in some cases, death. Mental health impacts are also common, with abused women suffering from high rates of depression, anxiety and PTSD.2 The primary care sector plays an important role in violence prevention by providing universal services, interventions and initiatives aimed at the general population or specific groups in the population, which help to reduce vulnerability and risk.
GPs also have an important role in responding to people and families who have experienced violence, abuse and neglect. However, many GPs do not feel skilled in responding to violence and do not report seeing many patients who experience violence.2 This article offers practical information to GPs on recognising and responding to presentations of violence. For the purpose of this article, female pronouns have largely been used, but the principles described apply to all victims regardless of gender or sexuality.
Types of domestic and family violence
There are many names and subtly different definitions for domestic violence (DV) depending on the relationship between the perpetrator and the victim. The central element is aggressive, controlling and intimidating behaviour that causes physical, sexual or psychological harm. Domestic and family violence (DFV) involves any family members, including partners, ex-partners, parents, carers, children and anyone in a familial relationship. Intimate partner violence (IPV) refers to behaviour by an intimate partner or ex-partner. This article uses DV to describe the spectrum of abuse that GPs are most likely to come across in daily practice.
Who is most vulnerable?
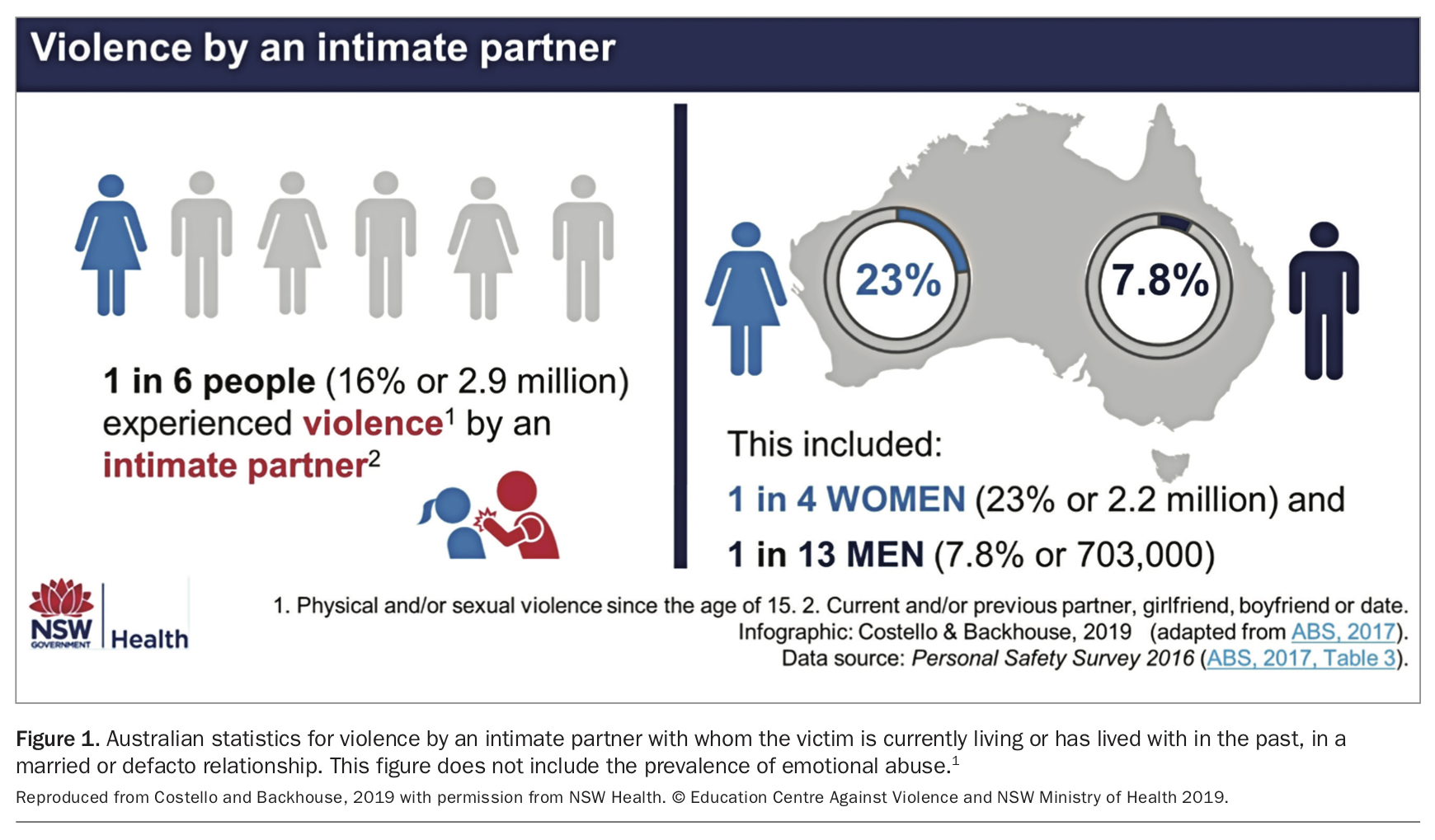
In Australia, one in six people experience DV (16%; one in four women and one in 13 men; Figure 1)1 and there is significant evidence that specific groups of people are more vulnerable to domestic violence, including Aboriginal and Torres Strait Islanders, people with a disability, gender-diverse people, people with a mental illness, culturally linguistically diverse people, migrants and refugees.3 However, women still remain the most vulnerable group, with violent behaviour in most cases of DV used to exercise power and control over women and their children. Women often feel compelled to stay in these violent relationships because of the challenges and barriers to leaving, including serious threat from their partner if they attempt to leave, financial insecurity, homelessness, family and social pressures, and traditional beliefs regarding the importance of keeping the family intact.
{kind=link}
According to the Australian Bureau of Statistics’ Personal Safety Survey, the proportion of women who experienced partner violence in the previous 12 months has remained relatively stable over the past decade.4 However, this figure has increased slightly since 2005, when around 1.5% of women aged 18 years and over disclosed partner violence in the previous 12 months, compared with 1.7% in 2016.4 Additionally, women who experience sexual assault as part of abuse are seven times more likely to be killed than other abused women.5 Sexual violence in the context of DV remains under-reported because of stigma and shame. A number of evidence-based risk factors that can indicate severe or lethal violence by men against their female partners are summarised in Figure 2. Identification and therapeutic work with perpetrators of violence may also fall into the clinical remit of the GP. However, this work is beyond the scope of this article. Men’s Referral Service (www.ntv.org.au/get-help) can provide referral information for men who are perpetrators of violence.
{kind=link}
Identifying patients affected by domestic violence
The primary care setting is a common place for initial presentations of DV. Fulltime GPs are estimated to see up to five women per week who have experienced some form of intimate partner abuse (physical, emotional or sexual) in the past 12 months,2 and it is estimated that over one in five women make their first disclosure of DV to their GP.6
Presentation
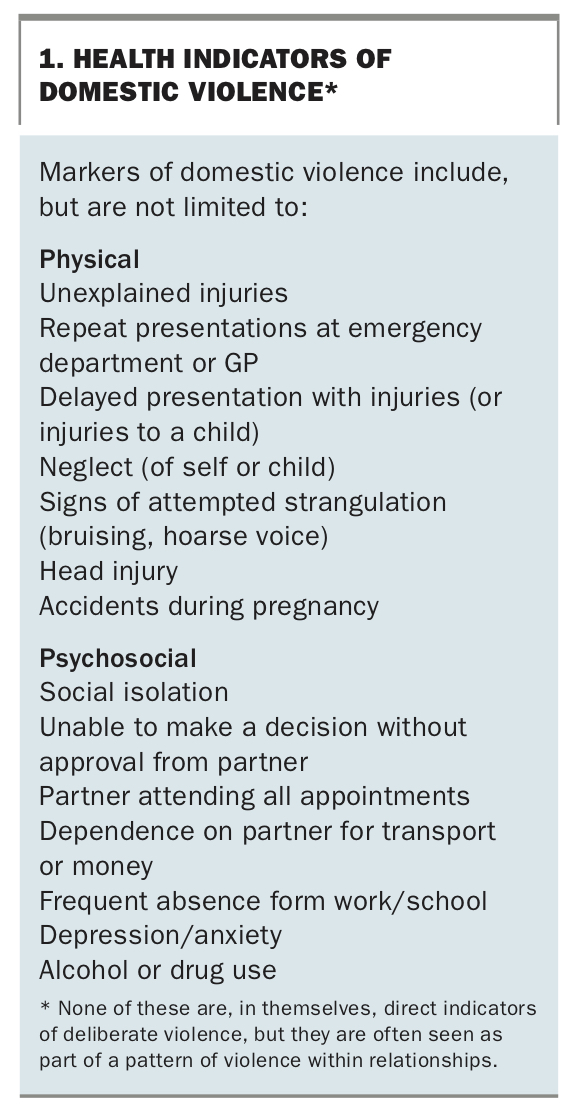
Indicators of violence can range from the obvious unexplained injury to subtler psychological symptoms (Box 1). When a patient presents with acute physical signs that are clearly the result of violence, the cause of the violence may still remain unclear and patients are not likely to disclose without prompting. More commonly though, patients will present with anxiety, depression and non-specific pain syndromes, or present frequently without a clear underlying pathology. There is no clear pattern to this presentation which flags domestic violence as a cause, however as violence and abuse are common causes of psychological stress, this diagnosis should be considered as a possibility when there is no clear precipitating factor for a patient’s presentation.
{kind=link}
Patients may also present after sexual violence. Forced sexual activity within an intimate partner setting is a strong indicator of the severity of violence. Sexual violence in a relationship is rarely an isolated form of abuse, so it is important to ask about other forms of ongoing abuse if sexual violence is disclosed or presented.
In the clinic
Within the healthcare profession, there are moves towards ‘screening’ for DV to identify and assess at-risk patients by asking routine questions to all patients in a range of healthcare settings, such as mental health or maternity care.7 This strategy has not been widely adopted in general practice because most patients are seen on a regular basis and the doctor–patient relationship provides a structure within which an assessment of risk can be made in a less formal way.
GPs can play a role in identifying patients who might be affected by DV by being aware of possible signs and symptoms of abuse, and addressing issues such as family safety within routine consultations. Additionally, GPs can indicate that their clinic or office is a safe place for disclosure by putting up violence prevention posters and making leaflets available in the waiting room. These are useful resources that can be accessed reasonably anonymously by patients, particularly women, while they attend to other routine medical care.
Most patients experiencing violence would like to be asked about it by their healthcare providers and are more likely to disclose if the issue is addressed directly.7-9 If a GP suspects that DV is occurring, they can enquire further in some of the following ways:
- direct questioning (‘Has your partner ever hurt or threatened you?’, ‘Are you scared or frightened of your partner?’)
- asking about specific symptoms (‘When I see injuries like this, I wonder if someone could have hurt you?’)
- simply alluding to the prevalence of DV.6
Even if a patient does not disclose DV on direct questioning, the act of asking indicates to them that this is a serious health problem and that the GP clinic is a supportive environment in which to disclose. Patients who are not experiencing violence or abuse are rarely distressed or offended by being asked these questions.
Responding to patients affected by domestic violence
An initial response to a disclosure of violence needs to be non-judgemental, compassionate and supportive. It is important to support the patient’s decision making, recognising that many women would like to stay in their current relationship, but would like the violence to stop. In some cases, it may be useful to formally assess and document a women’s experience of violence. It is important to reflect back to women that the violence that they have disclosed puts them at risk and that they should consider leaving the relationship in the future, even if they are not ready to do so at this moment in time.
Safety assessment
It is important to assist patients in evaluating their immediate and future safety, and that of any children. Often, information gathering for such an assessment can be done in a conversational manner as part of a medical or social history. Check for immediate concerns; for example, by asking ‘Do you feel safe to go home today?’, and assess the risk of ongoing and serious harm. There are a range of DV safety assessment tools available, based on the predictors of serious harm. If a patient discloses any of the high-risk factors for DFV (Figure 2), then this is an indicator that your concerns need to be escalated to a specialist service or to police.2
Safety planning
Safety planning should be an ongoing process, and should be informed by the woman’s preferences and choices. This should include a discussion about how to stay safe while in a relationship with a violent partner and information on how to leave, if she wishes to do so. It is important to remember that women are at highest risk of serious violence when leaving a violent relationship as the perpetrator may escalate in response to the victim's actions.
Things to consider as part of a safety plan for women affected by DV include:
- Accommodation – where would a woman go if she had to leave?
- Transport – how would she get there?
- Protecting children – is the school aware of a violent partner who may be a threat to the safety of the children? Are there other carers for the children (e.g. grandparents or babysitters) and are they aware of the threat to the children and woman?
- Financial planning – does the woman have access to her own bank account?
- Technology – is she being tracked? Can she get access to her devices?
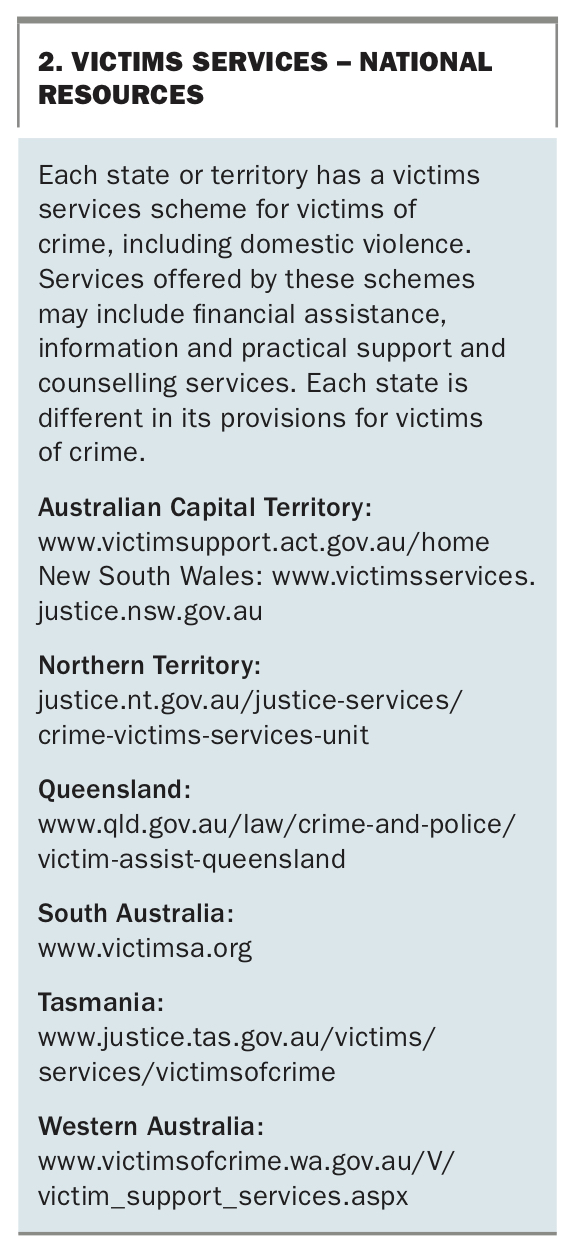
Free counselling and immediate financial assistance may be available. A list of state and territory services for victims of crime, including DV, are listed in Box 2.
{kind=link}
Referral services
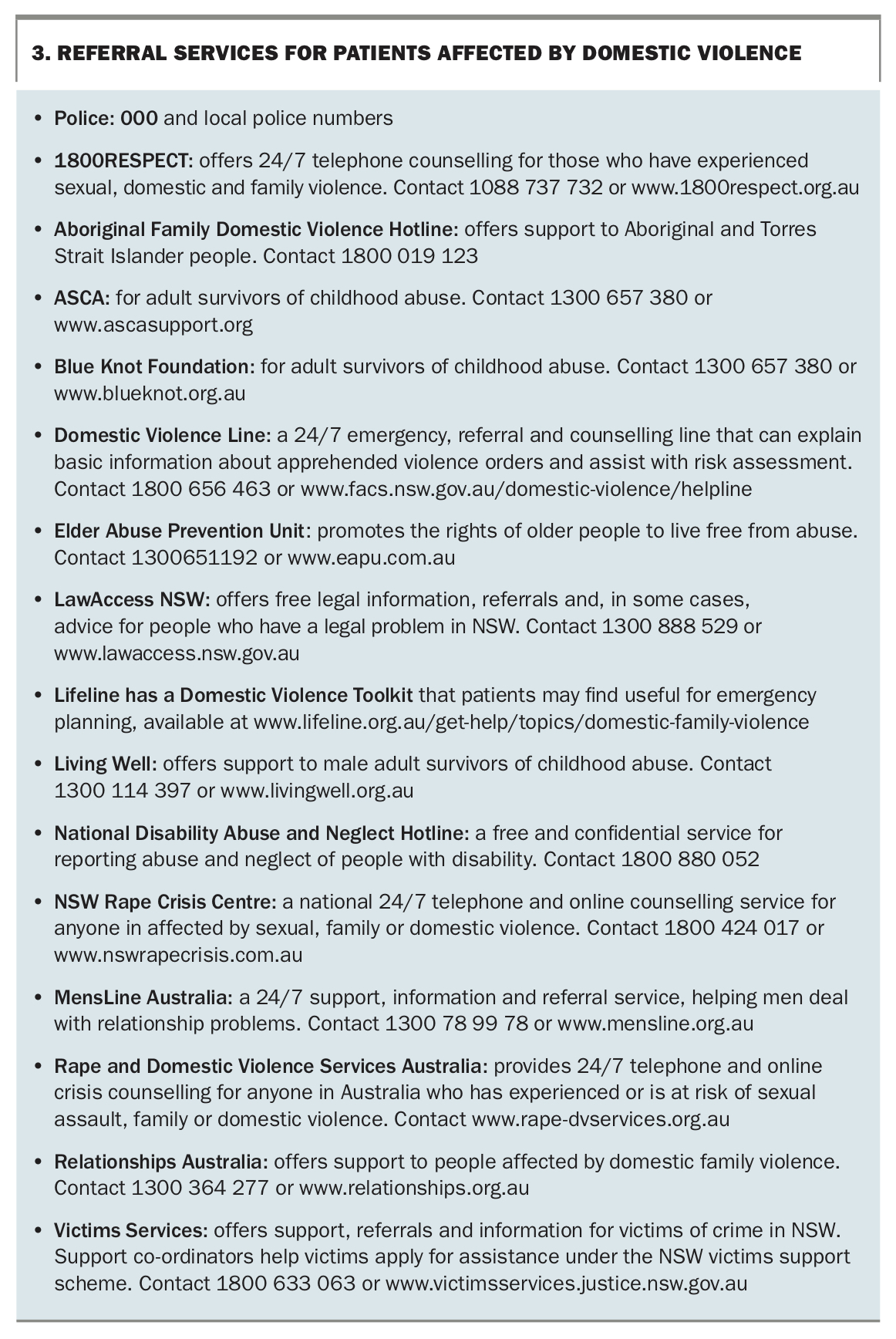
An important step in responding to a patient affected by domestic violence is to ensure that the contact details of relevant emergency services are provided, regardless of whether the patient has openly disclosed or has refused further assistance. Relevant emergency services are outlined in Box 3.
{kind=link}
The case study in Box 4 illustrates a scenario of how a patient may present for and disclose DV, and how the attending GP can offer support and guidance.
{kind=link}
Sexual assault services
Patients experiencing a sexual assault should be offered the option of a referral to a sexual assault service. Patients who present with signs of recent sexual assault (within 7 days) can access forensic examination services, and all sexual assault services can provide specialist counselling to victims of recent and past sexual assault. Sexual assault services are located in all Australian states (Box 5) and most provide a 24-hour service including medical and forensic examination.
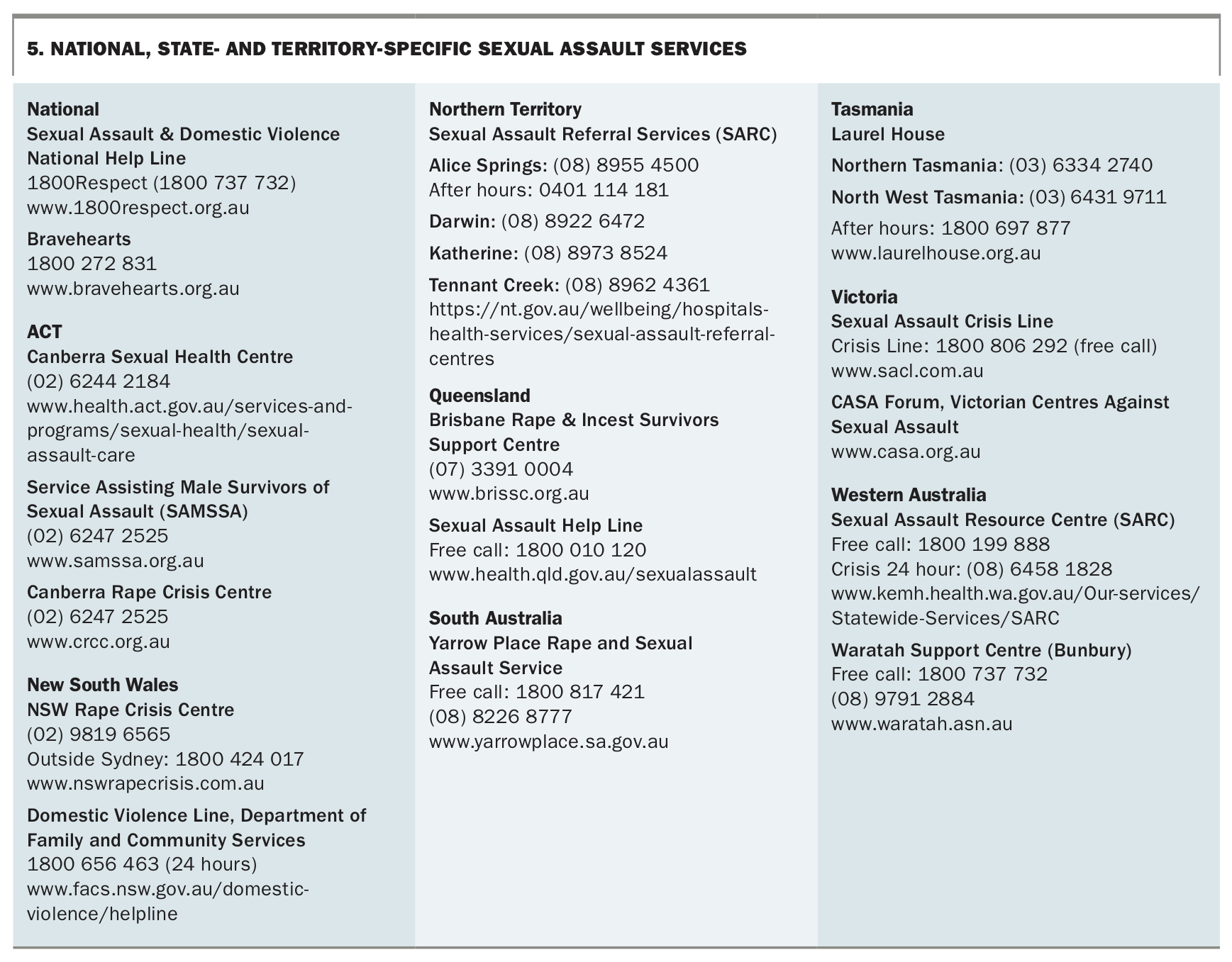{kind=link}
Immigration family violence provisions
A patient who has disclosed DV may have concerns about her visa status if she leaves her partner. There are provisions in immigration law that can protect women who leave abusive relationships where a relationship with an Australian sponsor has broken down. Further state- and territory-based information is available at www.1800respect.org.au/service-support/.
Documentation and privacy
Confidentiality is a legally enshrined principle of healthcare records and should be respected unless there is a good reason to breach privacy. Information should not be disclosed to a third party, including to the police or the courts, without the patient’s consent unless there are mandated reasons for doing so. Be aware that the records taken at the initial disclosure of an assault, including notes taken in the nonspecialist setting, may subsequently be subpoenaed.
Documentation relating to a disclosure of DV should be clear and specific. In certain circumstances, such as disclosure of a threat, it is important to record as much of the patient’s own words as possible; for example, ‘he said he would kill me if I told anyone’. It is not recommended to put the alleged perpetrators name in the notes, as this can lead to breaches of confidentiality and privacy, especially if the alleged perpetrator is also a patient of the service.
Naming the perpetrator may be seen as a means of protecting a woman’s safety, by alerting services and other healthcare providers to the source of a threat; however, this can have the opposite effect as it may lead the perpetrator to discover that she has made a report or disclosed the abuse. The decision to disclose the name of the perpetrator should be made on a case-by-case basis, and if the GP feels that a woman’s safety is best maintained by naming the alleged perpetrator, this can be done in a separate ‘locked’ set of notes. These notes would be kept separate from the patient's main medical records in a password-protected or physically separate location, so that only services who need to know this information would have access. All notes can be subpoenaed including these ‘locked’ notes, in a criminal investigation.
Mandatory reporting
The decision to report an assault to police is the victim’s alone, unless safety risks make a report mandatory.
Children
There is a requirement to report children at risk of significant harm, although the legislative and practical framework varies across states in Australia. In the context of a disclosure of DV, circumstances include experiencing physical or sexual violence or directly witnessing violence to a parent or carer in a domestic setting. Each state and territory have different legal requirements and local advice can be found in the Royal Australian College of General Practitioners publication Abuse and violence: working with our patients in general practice.2
Under Chapter 16A of the Children and Young Persons (Care and Protection) Act 1998, the legal framework for information exchange allows organisations such as schools, health departments and social services to share information relating to the safety, welfare or wellbeing of children or young people without parental consent.10 It takes precedence over the protection of confidentiality or of an individual’s privacy because the safety, welfare and wellbeing of children and young people is considered to be paramount. However, although consent is not necessary, it should be sought where possible.11
Adults
In NSW, under Part 13A of the Crimes (Domestic and Personal Violence) Act 2007, health workers are able to share information about victims and perpetrators to facilitate a victim’s access to support services and to prevent and reduce serious threats.12 Equivalent legislation on information sharing in the context of DFV also exists in Victoria, Queensland and in the Northern Territory. Additionally, AVO (apprehended violence order) issues in one state are recognised by police and legislative organisations in the others.
Sexual assault is not a reason for mandatory reporting to police or other services unless there are other risks identified such as serious injury to the victim or ongoing risk of serious harm by the perpetrator. It is the victim’s decision whether they report a sexual assault to police and there is no statute of limitations on reporting, i.e. the crime can be reported at any time even years after the assault.
Conclusion
There is still a great deal of stigma and shame attached to being a victim of DV, and many patients hide the true cause of an injury resulting from DV. Presentation of DV is not always obvious, and it may take time and trust within the doctor–patient relationship for violence to present or for a patient to disclose DV. The GP has a central role in identifying DV, providing a supportive response and referring patients to local support services. MT
References
Features~Prevalence%20of%20partner%20violence%20over%20time~19 (accessed November 2019).
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.