Recognising and responding to domestic violence during COVID-19: how telehealth can help

The COVID-19 pandemic has seen an unprecedented shift to telehealth in general practice in Australia. At the same time, there are concerns of a likely increase in the risk of domestic violence. GPs need to be aware of the benefits and risks of telehealth consultations and be equipped to recognise and respond to patients affected by or at risk of domestic violence.
Domestic violence (DV) involves a pattern of aggressive, coercive, controlling behaviour towards an intimate partner or family member or members and includes physical, psychological, sexual, economic and emotional abuse. Such violence and abuse can have serious and lasting effects on mental and physical health. Recent Australian pre-COVID-19 statistics show that one in six people experience DV, with women three times more likely to be victims of DV than men.1 DV is a major cause of morbidity in reproductive-age women, but can also affect men in heterosexual or same-sex relationships, and may manifest as anxiety, depression, alcohol and drug use as well as the more obvious physical injuries.
Recent media coverage of COVID-19 has identified concern around the increased risk of DV during the pandemic. Although research data is lacking, home isolation as a result of COVID-19-related public health measures has led to a global increase in media reports of DV.2 An exacerbation of DV has been reported during and after natural and other disasters, as normal routines and social support networks are disrupted.3 Although the COVID-19 pandemic is very different to other natural disasters such as bushfires, the disruption to everyday life, including an increase in stressors and a decrease in access to services, is a common experience in both types of events and is very likely to affect the experience of interpersonal violence. The mental health implications of living through natural and other disasters can be cumulative and can intensify existing experiences of trauma. People’s complex coping responses to violence, such as alcohol and other drug use, or the impacts on existing mental health issues, may also increase the risk of violence.
The COVID-19 pandemic and associated social and legislative changes have led to a range of domestic stressors that are likely to contribute to an increased risk of DV, including unemployment, financial strains, home schooling children and loss of the usual routines and social supports for both victims and perpetrators of violence. Critically, these stressors, coupled with enforced isolation as a result of the pandemic, are the likely cause of the increased reports of DV, with people who experience DV being in almost constant close proximity with the person who is abusing them.4
With COVID-19 restrictions in place, GPs are increasingly conducting consultations via telehealth, which offer benefits and challenges to both doctor and patient. This article provides practical guidance to GPs on how to recognise and respond to patients who may be affected by or at risk of DV in a telehealth context.
Use of support services during COVID-19
Many Australian domestic violence and assault services have reported an increase in calls and face-to-face presentations during the COVID-19 pandemic; however, some services reported a decrease in activity. According to media reports, in NSW, the 1800Respect Helpline reported an 11% spike in calls and Men’s Line Australia experienced a 15% rise in contact by men experiencing DV or using or at risk of using DV.5,6 A number of COVID-19 related factors may account for the decrease in activity reported by some services, including a lack of access to services due to victims being unable to find a safe space to call from and the lack of usual mandatory reporter interactions such as school or early childhood clinics. Confusion around public health messaging may have also contributed to the reduced use of social services, with reluctance from some people to attend medical and social services for fear of exposure to coronavirus, worry about the legitimacy of their medical needs in a constrained medical system or concerns about being fined for breaking isolation legislation. Unfortunately, the ‘Stay home, stay safe’ public health message is not one that applies to those experiencing DV.
Risks and benefits of telehealth associated with domestic violence
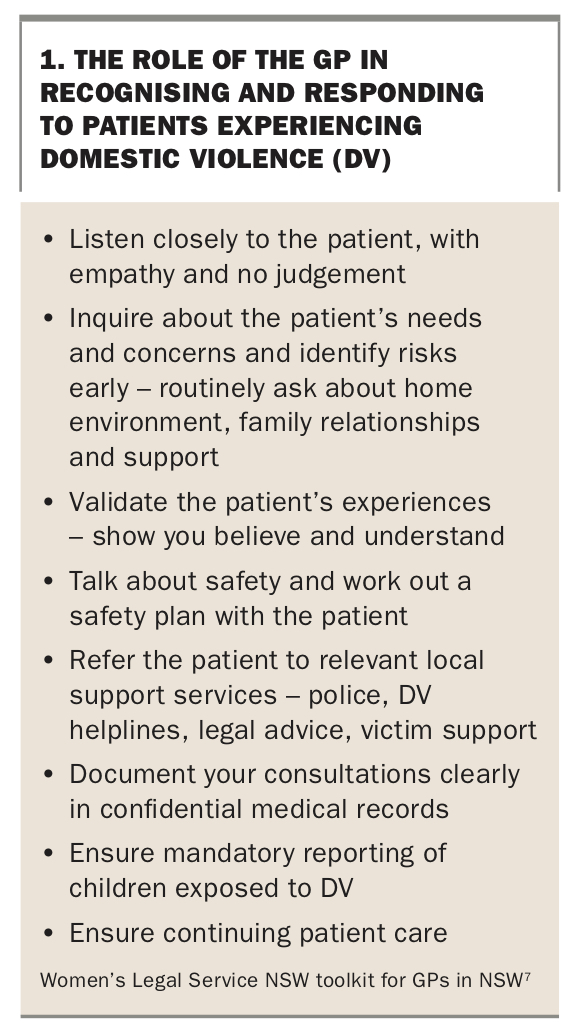
GPs play an essential front-line role in recognising and responding to DV, with data showing that one in five women make their first disclosure of DV to a GP.7,8 Box 1 provides a schema for the role of the GP, taken from the Women’s Legal Service NSW toolkit for GPs in NSW.7
{kind=link}
The COVID-19 crisis has seen an unprecedented shift to telehealth in general practice that will likely be sustained as a part of mainstream practice, given its benefits in enhancing access to health care, especially in rural areas.9 Telehealth is a new space for both clinicians and patients that offers benefits, but also risks for patients affected by or at risk of DV.
Benefits of telehealth
Telehealth may provide a number of benefits to people at risk of DV, the most obvious of these being access to support and health services during the COVID-19 pandemic, when it may be hard to leave home due to economic circumstances, lack of transportation or responsibility for young children. Telehealth can also benefit those who have difficulty getting time away from paid or unpaid work by providing increased access to services. The flexibility of telehealth means that for some people, this is the best way to ensure confidentiality and privacy as they can schedule an appointment at a time when they know they will be alone. The sense of anonymity provided by a telehealth consultation may also encourage victims of DV to disclose abuse and seek help.
Risks of telehealth
Telehealth consultations can also be a risk to those experiencing DV during the COVID-19 pandemic, particularly during lockdown, when victims may be forced into close and constant proximity to their perpetrators, making it difficult for them to find a private space to safely make and receive phone calls or look up information about support. Telehealth can leave a digital footprint and provide increased opportunities for perpetrators of DV to monitor victims’ activities and conversations within the home. It can also increase the risk of technology-facilitated abuse, which includes tracking movements and activities through devices such as phones, tablets and laptops.10 When perpetrators become aware of disclosures of violence and any subsequent interventions as a result of monitoring or tracking, there can be increased risk to the victim.11
An awareness of the safety issues surrounding technology use and developing skills to provide the same nuanced conversations around DV that occur during a face-to-face consultation is therefore essential. It can be helpful to raise awareness of safety apps for people experiencing DV that provide immediate access to help and have an emergency escape function to shut down the screen.
Recognising and responding to domestic violence with telehealth
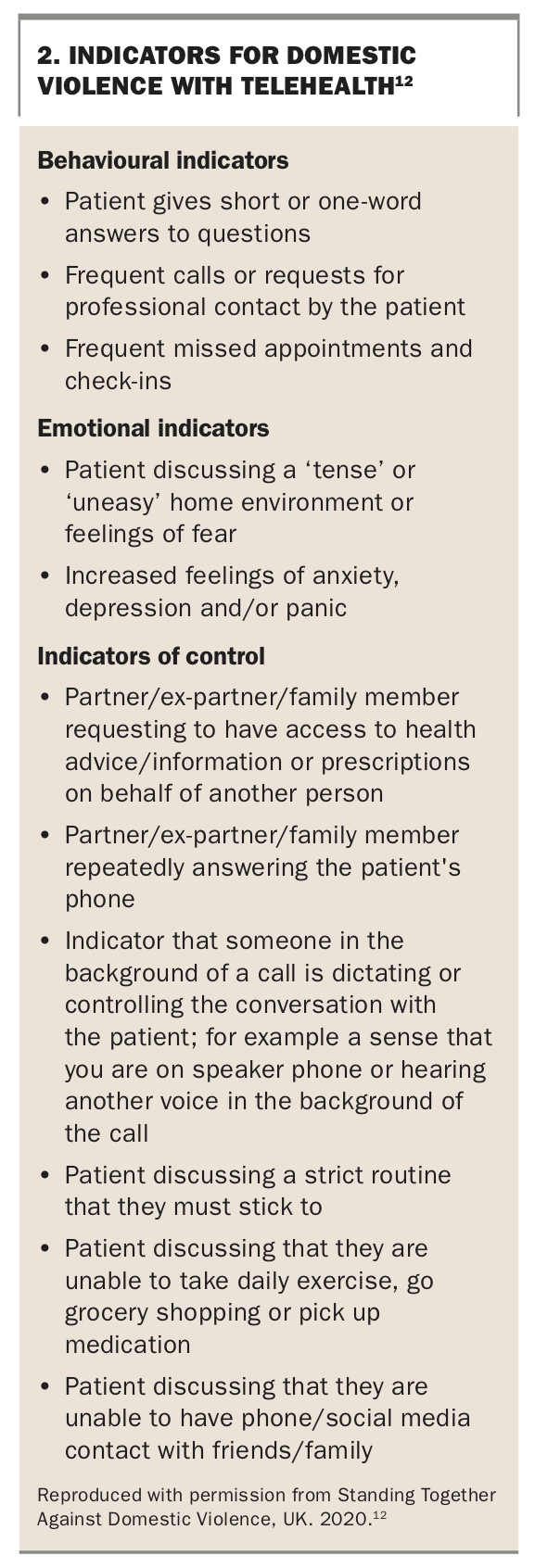
Telehealth can be provided by phone or video call but, even with the latter, the usual body language cues conveying anxiety, distress and fear may be absent. However, there are potential indicators for DV that GPs should be aware of during telehealth consultations, such as short or single word responses from the patient to questions, a partner or ex-partner repeatedly answering the patient’s phone or having a sense someone is controlling the patient’s conversation in the background (Box 2).12
{kind=link}
Establishing a safe space
In a telehealth consultation, it is essential to gain informed consent, communicate the limits to confidentiality from the outset of the call, and to plan for and check that patients are in a position to speak safely and privately. Asking some general questions about how patients are coping with changes due to COVID-19 can be used to start a conversation and to indicate to the patient that help is available. Examples of such questions include ‘How are things at home right now?’ or ‘How are you coping with the extra stress of having children/husband at home?’
If a patient discloses DV or describes behaviours or situations that make you think they may be at risk, then acknowledge the disclosure and check whether they are able to talk further, by saying something like, for example, ‘I’d like to ask you some questions about your safety – it’s important that you are alone – just answer yes or no – is it okay to continue the conversation?’ If the patient is unable to continue the conversation, do not continue to talk about the violence, but do check in whether they are able to talk about other health matters. Try to find a time to call back or arrange a face-to-face appointment. Ask about times that they may be alone, either at home or going out for exercise or shopping. It is helpful to use questions with ‘yes/no’ answers to elicit a safe response.
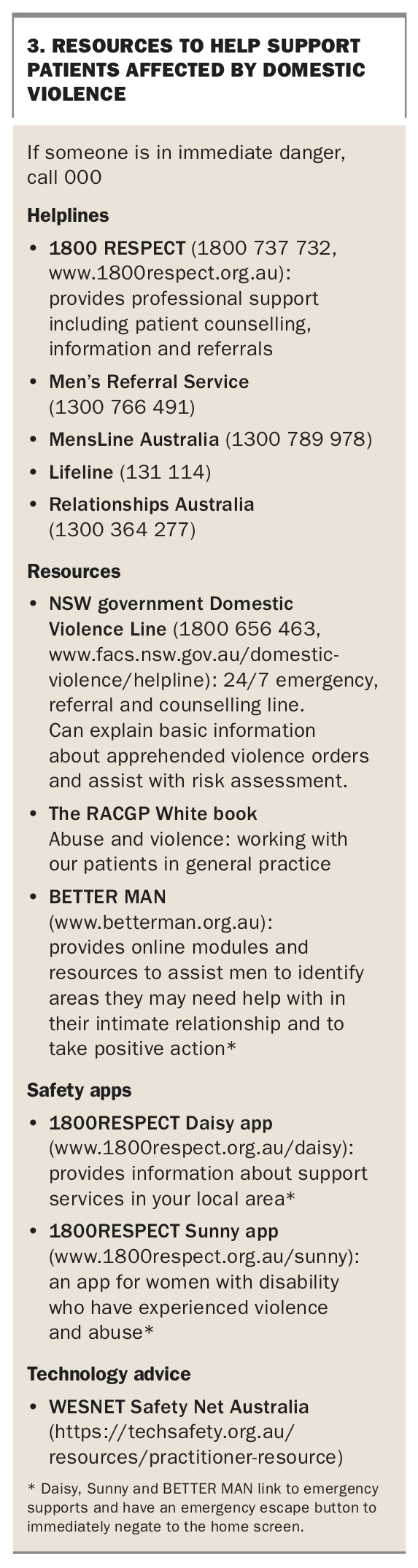
If you have any concerns about the safety of a patient or anyone in the household, remind them they can call 000 at any time, and of local emergency services. GPs can also call police if they feel it is appropriate to do so, as well as specialised services such as 1800Respect and other state- and territory-based DV services to anonymously discuss individual cases with a trained counsellor without naming the patient, either during a consultation or afterwards, depending on the circumstances. Resources to help support patients affected by DV are listed in Box 3.
{kind=link}
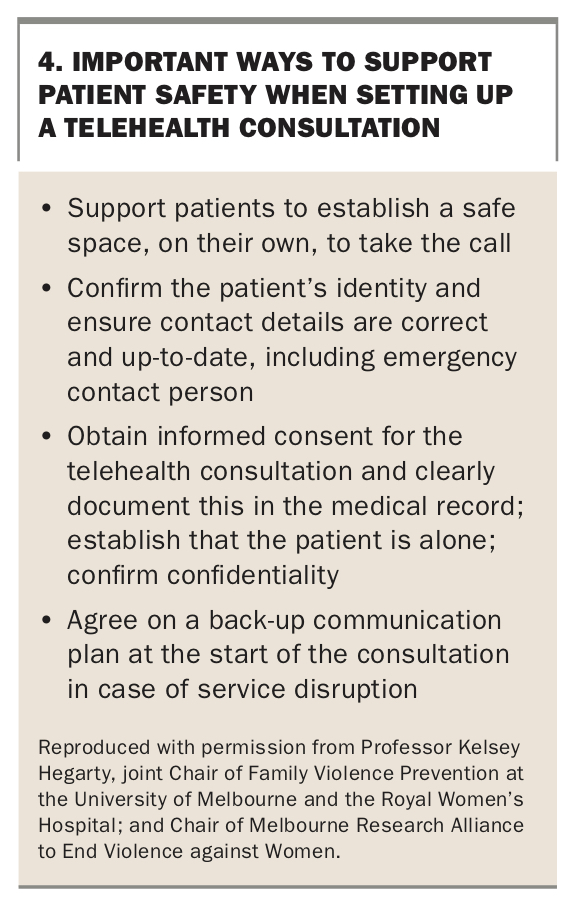
In advance of the next telehealth call, or if the patient is currently alone, it can be helpful to establish a code word or sentence to end the call if needed such as ‘Wrong number’ or ‘Thank you, but I’m not interested’, although both the GP and the patient need to be very clear on its use. Box 4 highlights important ways to support patient safety when setting up a telehealth consultation.
{kind=link}
Assessing risk to patients via telehealth
Once a safe telehealth space has been established with the patient, you can assess their risk of harm in their current situation. Questions to ask to assess risk include the following, noting that a yes response to any of these can indicate a risk of serious harm:13
- Is the patient still living with the perpetrator of the violence, or has the perpetrator been returning to the home?
- Are there children at risk?
- Is there an apprehended domestic violence order in place and have there been breaches of the order by the perpetrator?
- Has the perpetrator physically harmed the patient, or anyone in the patient’s care such as children or elderly parents?
- Has the perpetrator threatened to hurt the patient, children or pets, including threats to cause the patient or the patient’s children to contract COVID-19?
- Is the perpetrator controlling of communications, activities, and access to money and essential items?
- Has the perpetrator threatened to harm themselves or suicide?
- Have any of these abusive behaviours been increasing in frequency and/or severity?
- What is the patient’s own assessment of risk?
If you assess a patient as being at risk of harm, share this concern with them and work with them to make a safety plan. Reassure patients that domestic and family violence services are deemed essential services by all levels of Australian government. Conversations with patients about safety need to include planning about how to stay safe in a violent situation and how to leave if they wish and are able to. Safety plans that pre-date COVID-19 may be impacted by isolation regulations and realities and should be re-established.
- If the patient is planning to leave, some considerations include:
- Is it safe to pack a bag and where can a packed bag be left?
- Does the patient have a safe place to stay?
- Do they have access to an untracked phone?
- Can they access money and documents such as driver’s licence and passport?
These questions are also important for those planning to stay in potentially unsafe situations; it is useful to have a leave plan even if there is no intention to implement it. Safety planning in this situation should include identification of safer spaces within the home such as rooms with easy exits, or rooms that can be seen or heard from outside. Patients can be supported to put emergency numbers into their phones, to stick them on the fridge and to memorise them.14
Explore with your patient whether it is possible to leave the home to attend face-to-face services, or if there is another safe place that they can access on a regular basis, such as the supermarket or the hairdresser, from which they can make or receive calls. If your patient is willing to access specialist DV services, check if they are happy for you to make referrals to local support services and the safest way to communicate with them. Finally, consider your obligations as a mandatory reporter for children at risk of serious harm. If you feel that you do need to make a report about children, discuss this with their carers where possible and consider their point of view and safety as part of your decision-making process.
Conclusion
Although data are still emerging, it seems likely that the COVID-19 crisis has increased the risk of DV. The reasons for this increase include stressors associated with home isolation and reduced access to services for both victims and perpetrators of DV, such as helplines and GPs. The shift to telehealth during the crisis is likely to continue as a part of general practice service provision and presents risks and opportunities for recognising and responding to DV. It is important that GPs recognise the risks associated with telehealth and help patients establish a safe space before continuing assessment. GPs’ skills in listening and asking questions with empathy and lack of judgment are essential for supporting patients experiencing or at risk of DV during these unprecedented times. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.