Recurring swelling on finger

What is the probable cause of a recurring cystic swelling on a patient’s finger and how would it best be managed – conservative treatment, cryotherapy or surgical intervention?
Case scenario
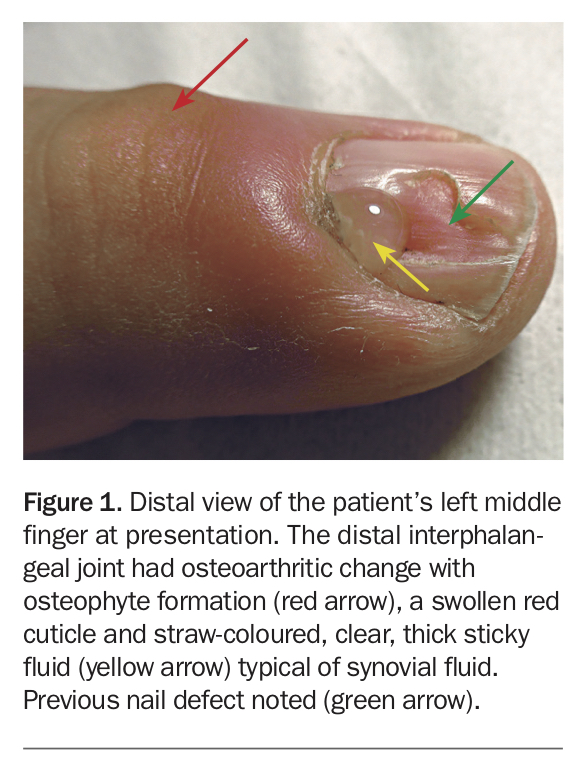
A 66-year-old male office worker presents with a swollen, inflamed cuticle that discharges clear fluid following application of pressure (Figure 1). He had noticed a cystic swelling on the dorsum of his left middle finger over the distal interphalangeal joint (DIPJ) eight weeks earlier, which spontaneously drained, leaving a residual nail defect. Relevant past history includes a DIPJ fracture many years ago, with secondary osteoarthritis (OA) and osteophyte formation. He is treated conservatively.
{kind=link}
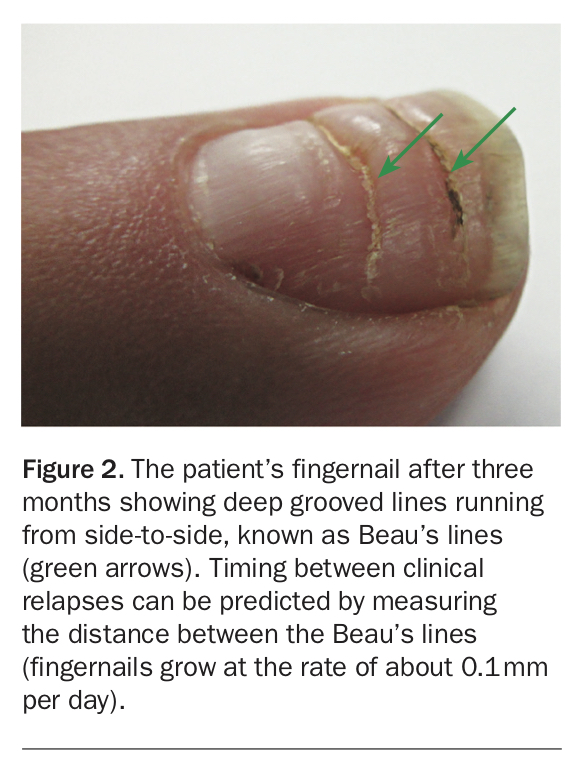
On follow up three months later, he reveals that he has had two other attacks, with progressive nail changes (Figure 2).
{kind=link}
Diagnosis
The diagnosis is digital mucous cyst secondary to DIPJ OA – one of the most common benign ungual tumors.1 The cyst usually has a stalk connected to the DIPJ, which allows repeated growth and episodic drainage of fluid as synovial fluid builds up in the underlying arthritic DIPJ. As it grows, the cyst presses on the nail plate, affecting growth, which can lead to nail deformity and scar formation. Digital mucous cysts are common benign lesions that present as a firm nodule on fingers or toes. The lesions are usually not painful and are located adjacent to distal joints. The age range of presentation is wide, with highest incidence and prevalence in the seventh decade. Spontaneous remission is unusual.1
Beau’s lines are present in one-third of cases. They are the result of local pressure on the nail matrix, where the fingernails start to grow, causing temporary cessation of cell growth and subsequent nail changes. The cysts are usually chronic, and rarely resolve spontaneously. Other factors that affect nail growth include trauma, fungal nail infection, malnutrition, medications and systemic disorders such as coronary occlusion, hypocalcaemia and chemotherapy. The differential diagnosis of Beau’s lines include Muehrcke’s lines, which are areas of hypopigmentation without palpable ridges on the nails, and Mees’ lines, which are areas of discolouration in the nail plate.
Commentary
Mucous cysts of the fingers are benign and do not usually require surgery. Conservative treatment includes observation, repeated sterile draining and cyst aspiration, and injection with corticosteroid. Cryotherapy with liquid nitrogen and carbon dioxide ablative laser are sometimes used, but are best avoided as they can be associated with persistent nail deformity.2 Repeated cyst occurrence usually requires surgical intervention.
A Korean study reported the successful use of laser therapy to successfully ablate and coagulate the cavity walls of recurrent digital mucous cysts in two patients.3 A review of 134 mucous cysts on the fingers of 116 patients treated by one surgeon over 11 years with a minimum follow up of two years found that 31 of the patients had nail ridging or deformity at presentation.4 Eight patients underwent multiple soft-tissue punctures of the cyst with a 25-gauge needle and injection with local anaesthetic and corticosteroid. Multiple needle passes were performed to produce scar formation to stop the capsule leaking. A compression tubular gauze dressing or elastic digit bandage was applied for several days, followed by activity, as tolerated. Fifty-four patients underwent surgical excision of the cyst, stalk and osteophytes and joint debridement with careful protection of the extensor mechanism.
In the aspiration/injection group, the problem did not recur in 48 digits (60%). Among the 32 with recurrence, the mean time to recurrence was 6.7 months (range, 1 to 23 months). Repeat injections were performed in eight cases, with only three being curative. Hence, while aspiration/injection was convenient, there was a 40% recurrence rate.
In contrast, surgery provided definitive treatment with no major long-term complications in any of the 54 patients.4 In addition, the 29 cysts that failed to respond to injection were cured with surgery. Nail ridging resolved in most cases after surgery. Two superficial wound infections occurred in the injection group, and the surgical group had one deep and two superficial infections. The superficial location of the cyst and its communication with the DIPJ made it vulnerable to infection. Simple excision of the cyst has been associated with higher recurrence rates compared with more aggressive surgical techniques that remove osteophytes from the DIPJ.4-6 Possible surgical complications include diminished range of DIPJ movement, infection, recurrence and persistent nail deformity.
Conclusion
Although concerned about the recurrence, once the patient knew what the lesion was and that it was benign, he chose conservative management. However, if the cyst recurs, and if symptomatic, surgery remains an option. MT