Burning soles of the feet

A burning sensation affecting the extremities can have a negative effect on quality of life. Simple measures and pharmacological interventions may provide relief but management can prove difficult.
Case scenario
Abe, who is 58 years of age, complains of a burning sensation affecting the soles of his feet. It only occurs when he is in bed at night and often keeps him awake. Sometimes the discomfort eases if he gets up and walks around; at other times he immerses his feet in cold water for relief. He has no symptoms during the day and says that in fact his feet are usually quite cool to the touch at other times, as are his hands.
Abe works in a sedentary job but he is quite physically active, walking regularly and playing golf, despite evidence of some early osteoarthritis of his hips and knees. His weight is in the normal range. He has hypertension controlled by an ACE inhibitor, and there is a family history of ischaemic heart disease. He is a nonsmoker and his fasting lipids and glucose levels are within the normal ranges.
What is the mechanism of Abe’s burning soles and what can be done to ease his discomfort?
Commentary
The symptoms and initial evaluation in Abe’s case are highly suggestive of erythromelalgia, an uncommon clinical syndrome characterised by episodes of burning pain, redness and increased temperature (sensation of intense heat) affecting the extremities – usually the lower limbs (alone in two-thirds of cases) and predominantly the feet and soles (Figure). The hands may be involved in up to one-quarter of cases. The pain may be severe and seemingly out of proportion to the clinical findings.
{kind=link}
Clinical features
Erythromelalgia usually remains intermittent, generally lasting for minutes or hours before resolving. Episodes are typically precipitated by exercise or an increase in environmental or local warmth, and often occur during the evening or at night. The symptoms tend to be much more severe during summer months. Mild symptoms often impair normal activities such as walking and exercising. Sleep may also be affected. Some patients report that symptoms become more frequent and prolonged over months to years. Occasionally, episodes become severe, continuous and disabling.
A characteristic feature of erythromelalgia is that patients instinctively resort to cooling the affected areas to provide complete (but temporary) relief. Such measures include using a fan, walking on a cold surface such as a tiled floor, applying ice packs (or equivalent), or submerging the feet in cold water or iced water. Symptoms may also be ameliorated by elevating the extremity. However, continued immersion in iced water ultimately aggravates the problem by decreasing the temperature threshold at which symptoms recur and may cause a cold-induced neuritic syndrome that amplifies the disease.
Examination reveals erythema and warmth of the affected extremities. Results of pulse examination, including digital pulses, are normal and there is no clinical evidence of a peripheral neuropathy, connective tissue disorder, vasculitis (purpura), microembolic event or infection. Skin injury, blisters or ulceration, or perniosis, may be evident from repeated use of iced water. Rarely, frostbite and digital necrosis occur.
Between episodes, the characteristic features of redness, heat and pain are absent. In up to two-thirds of patients, the extremities will be cool and cyanotic (acrocyanosis) or there will be features of Raynaud’s phenomenon.
Aetiology and pathogenesis
In most cases the cause of erythromelalgia is unknown and the condition is referred to as primary or idiopathic erythromelalgia. It usually occurs spontaneously and may present at any age but is most common in middle age. Males are more commonly affected than females. Symptoms in primary cases are typically bilateral and symmetrical. An autosomal dominant transmission has been postulated and may relate to a sodium channelopathy (heterozygous mutation in the SCN9A gene on chromosome 2q24) conferring hyperexcitability to peripheral nociceptive and sympathetic neurons.
In about 40% of cases an associated condition or factor may be present and the erythromelalgia is referred to as secondary. Symptoms are more likely to be unilateral or asymmetrical. Myeloproliferative disorders (particularly essential thrombocythaemia, polycythaemia vera) account for the majority of secondary cases, although the true incidence is unknown (estimates vary between 5 and 65%), and may precede, follow (by a median 2.5 years) or coincide with the development of erythromelalgia. Other secondary causes/associations have been reported, including drugs (calcium channel antagonists, ticlopidine, bromocriptine, fluoroquinolones), autoimmune disorders (e.g. systemic lupus erythematosus), hypertension, diabetes, mercury poisoning, mushroom poisoning, infections, neoplasms and pregnancy, but the relationships are unclear.
The pathogenic mechanisms of erythromelalgia are poorly understood but there is profound disturbance of vasomotor control of vascular tone. Studies have reported abnormal results from vascular, neurophysiological and autonomic testing. In most patients, neuropathy (predominantly small-fibre neuropathy) and vasculopathy (with intermittent increased blood flow and perhaps shunting) coexist. About 60% of patients have a large-fibre neuropathy with abnormal electromyography results. Thermoregulatory sweat testing during symptoms may show patchy areas of anhidrosis or hypohydrosis in a pattern consistent with small-fibre neuropathy. The increase in blood flow (measured by transcutaneous Doppler ultrasound) and temperature in affected areas, accompanied paradoxically by a decrease in oxygenation (measured by transcutaneous oximetry), suggests microvascular arteriovenous shunting leading to a deficit in skin nutritive perfusion and subsequent skin hypoxia. In addition, there is postganglionic sudomotor impairment and peripheral adrenergic dysfunction. Furthermore, a role for increased cellular metabolism has been postulated.
Investigations and differential diagnosis
The diagnosis of erythromelalgia is clinical and based on identification of key features:
- increased skin temperature or local heat involving the symptomatic region
- intense burning pain involving the distal extremities that is aggravated by warming and relieved by cooling
- marked erythema of the acral regions.
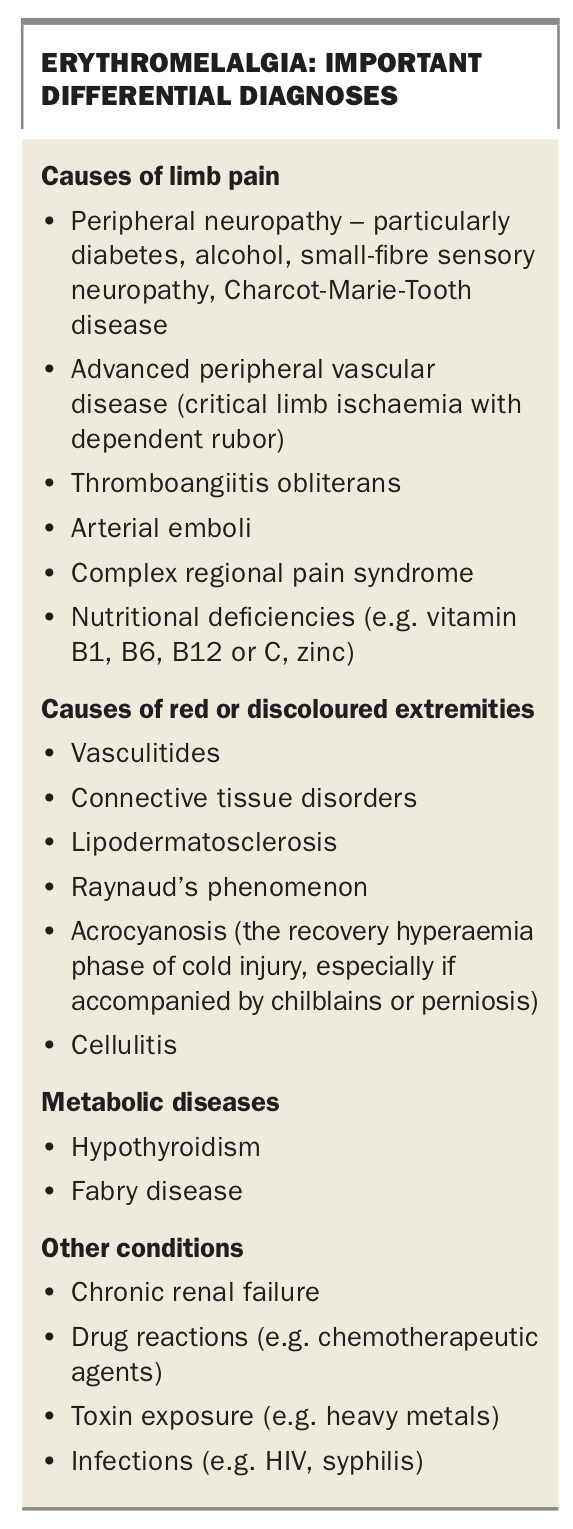
There are no laboratory biomarkers for erythromelalgia and no serological tests can confirm the diagnosis. Baseline laboratory investigations should include full blood count, erythrocyte sedimentation rate and C-reactive protein, blood glucose, liver function tests, cardiolipin antibody and autoantibody measurements. Additional testing should include exclusion of myeloproliferative syndrome. Important differential diagnoses for erythromelalgia are listed in the Box.
{kind=link}
Erythromelalgia may resemble complex regional pain syndrome (CRPS) or reflex sympathetic dystrophy, and distinguishing these conditions may be difficult. Most patients with CRPS have unilateral symptoms, are allodynic to cold and avoid cold exposure, and often have a history of injury or a known trigger for their symptoms. Furthermore, sympathetic blocks or sympathectomy are effective in CRPS.
Vascular evaluation should include assessment of all pulses, checking for colour change (elevation pallor and dependent rubor), skin and core temperature, ankle-brachial indices, blood flow (using laser Doppler flowmetry when available), oxygen saturation (transcutaneous oximetry), automonic function testing and adrenergic function testing.
Neurological evaluation with electromyography, nerve conduction studies and tests for small fibre neuropathy (e.g. quantitative sudomotor axon reflex test or thermoregulatory sweat testing) often reveals abnormal results. Routine performance of these tests is not usually recommended, unless to advocate the use of medications to treat concomitant neuropathy.
Skin biopsies of affected areas show nonspecific changes in primary erythromelalgia and are not indicated in the majority of patients. Skin biopsy samples in patients with myeloproliferative disorders show lesions in the arterioles: vacuolised and swollen endothelial cells, intimal proliferation, vascular smooth muscle cell proliferation and occlusive thrombi. Venules, capillaries and nerves are not involved.
Management
Unfortunately, there is no specific therapy or cure for primary erythromelalgia. Treatment often proves difficult. The lack of scientific studies and randomised controlled trials has limited the amount of established data about effective therapies. No guidelines exist to direct management, which primarily involves a combination of nonpharmacological and pharmacological (topical or systemic) interventions, and the response to individual strategies is highly variable. For most patients, nonpharmacological measures and topical pain-relieving medications improve symptoms. Patient counselling and pain rehabilitation programs are secondary modifiers.
Simple measures include avoidance of exercise or environmental temperatures that precipitate symptoms, limb elevation and short exposure to cooling measures such as fans or cool water but total avoidance of iced water. An air-conditioned environment may reduce distress, especially at night. Baths, using a water temperature below the threshold for pain, may give temporary relief. Any medications that the patient is taking should be evaluated as a possible causative trigger.
Topical medications for pain relief include lignocaine patches, compounded amitriptyline or ketamine, capsaicin cream, diclofenac gel and compounded gabapentin ointment as well as non-prescription pain-reliving rubs. Topical vasoactive medications (e.g. compounded midodrine 0.2%) may be helpful for improving redness.
Systemic therapy may be beneficial in patients whose symptoms are unresponsive to simple measures and topical therapies alone. Analgesics and sedatives may be necessary but narcotics should be avoided. Pharmacological strategies targeting neuropathy include gabapentin, pregabalin, tricyclic antidepressants and selective serotonin reuptake inhibitors. Strategies targeting vasculopathy include calcium channel antagonists, nitrates and beta-blockers.
In patients with the diurnal vasomotor pattern of symptoms, the intensity of erythromelalgia is often responsive to beta-blockers, which help to reverse the relaxed vasomotor tone at various points of time during the day/night. Agents such as metoprolol also affect reactive vasodilatory response in the skin arterioles. Topical nitrate patches, applied to the dorsum of the feet during the day when the patient is free of symptoms of erythromelalgia (i.e. on at 8 a.m. and off at 6 p.m.), may prevent any predisposing vasoconstrictor response in the skin during the day, making any rebound reactive hyperaemic phase in the night less likely.
Additional systemic agents used with benefit in some patients have included carbamazepine, oral misoprostol, sodium nitroprusside, high-dose oral magnesium and intravenous immunoglobulin. Systemic corticosteroids, used in patients with sudden-onset, severe erythromelalgia within weeks of onset, have sometimes led to improvement in symptoms. Rarely, epidural anaesthesia or surgical intervention with sympathectomy has been used for debilitating symptoms, with minimal success. Injection of alcohol into peripheral nerves has been tried without success.
Treatment of secondary erythromelalgia should be targeted towards the underlying cause and can effectively alleviate symptoms. In the setting of myeloproliferative syndromes, particularly thrombocythaemia, erythromelalgia is exquisitely responsive to aspirin, which can relieve symptoms rapidly and for several days. Indomethacin can be used but is only effective for about 24 hours. The underlying myeloproliferative disease should also be treated if possible. Aspirin is ineffective in primary erythromelalgia but a trial is worthwhile because symptoms can precede change in the peripheral blood count.
Final comments
Erythromelalgia can have a profound negative effect on quality of life due to the potential for debilitating symptoms. Treatment often proves challenging for primary erythromelalgia; however, some patients may undergo spontaneous remission. Treatment of underlying causes of secondary erythromelalgia is imperative. Early recognition and implementation of behavioural strategies can have a lasting impact. Patients who have refractory, debilitating pain may benefit from pain rehabilitation programs utilising a multidisciplinary and behavioural therapy approach to help restore physical activities and improve quality of life. Support groups such as The Erythromelalgia Association (https://erythromelalgia.org) can be a valuable resource for patients. In addition, counselling to reduce patients’ fear of precipitants and to encourage their participation in normal lifestyle activities has shown benefit. MT
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.