Alcohol – use and misuse during the COVID-19 pandemic

Dr Giannopoulos is a Senior Clinical Psychologist from Sydney Local Health District Drug Health Service, NSW and the Edith Collins Centre, Royal Prince Alfred Hospital, Sydney.
Associate Professor Kirsten Morley is an Associate Professor in the Sydney School of Medicine (Central Clinical School) Faculty of Medicine and Health, The University of Sydney, NSW and the Edith Collins Centre, Royal Prince Alfred Hospital, NSW.
Professor Haber is Clinical Director of Drug Health Services, Royal Prince Alfred Hospital; and Head of Discipline and Conjoint Professor, Addiction Medicine, The University of Sydney, Sydney, NSW.

GPs can play a pivotal role in the identification and management of alcohol problems at any time, and their role is even more important during the COVID-19 pandemic as more and more patients are resorting to alcohol to manage the stress and anxiety created by the pandemic.
- For some people, alcohol consumption has increased during the COVID-19 pandemic.
- This is likely associated with the elevated stress, anxiety and depression experienced by many, as well as increased time spent at home during periods of lockdown.
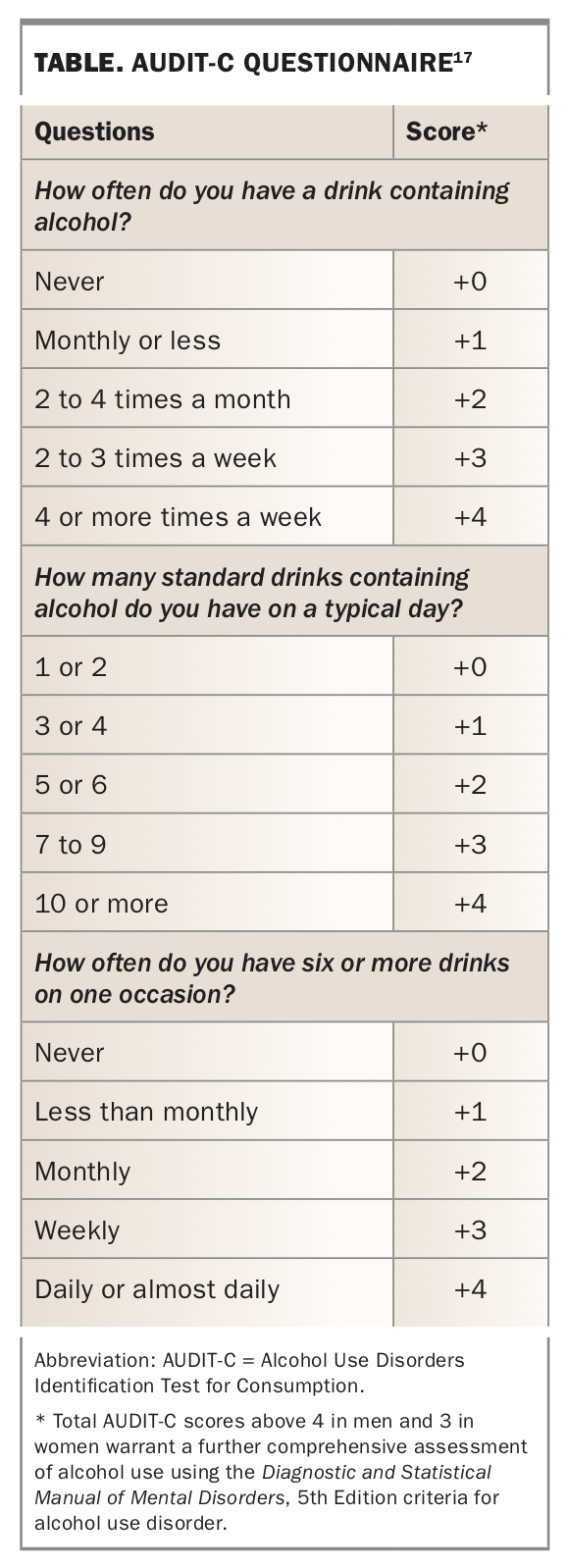
- GPs should screen every patient for alcohol misuse, even if they do not suspect it. The Alcohol Use Disorders Identification Test for Consumption (AUDIT-C) and the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition checklist for alcohol use disorder (AUD) are ideal assessment tools.
- Mental health problems commonly co-occur with AUD; therefore, GPs should also be prepared to investigate these during consultation.
- Laboratory investigations and physical examination may also indicate AUD; however, they should not be used in isolation.
- Management options include pharmacological treatment, withdrawal management and supportive counselling.
Alcohol is the most widely used drug in Australia, with almost 85% of the population reporting at least occasional use and 20% exceeding recommended safe drinking levels.1 Of the risk factors contributing to the burden of disease in Australia, alcohol ranks sixth, with over 200 medical conditions attributed to alcohol use, including chronic liver disease (which covers liver cancer), injuries sustained through motor vehicle accidents, suicide and self-inflicted harm.1 In recent years, population-wide alcohol use has fallen but medical complications have not changed significantly. Fewer than 20% of those with problematic drinking seek treatment for their alcohol use.2 Given most people in Australia visit a GP at least once per year, GPs are ideally placed to identify those with problematic alcohol use, and to screen all patients routinely as recommended by the RACGP guidelines.3
Impact of COVID-19 on alcohol use
The impact of COVID-19 on the drinking patterns of people in Australia has resulted in either a marked reduction in alcohol use or, conversely, a marked increase in alcohol use. As a result of the pandemic, the Australian government introduced social distancing measures and ordered nonessential services including licensed venues such as pubs and clubs to temporarily close, which resulted in changes to the sale and consumption of alcohol.4
For some people, lockdown offered an opportunity to change previously problematic drinking behaviour by facilitating abstinence.5 Changes in financial security because of the pandemic may also have indirectly contributed to forced abstinence from alcohol, and may account for the increased rates of complicated alcohol withdrawal reported during the COVID-19 pandemic.6,7
Although some Australians reduced their drinking during COVID-19, others increased their alcohol intake. Alcohol sales and home delivery increased significantly during the pandemic. Spending more time at home and the increased stress associated with the pandemic has led many Australians to increase their alcohol intake, with women aged 35 to 44 years reporting the greatest increase in alcohol consumption.8 Using alcohol to cope with anxiety and stress was reported by one in three people in Australia during lockdown.9
Stressful life experiences such as pandemics and other natural disasters are associated with increased risk of alcohol use and alcohol-related problems.10,11 However, the COVID-19 pandemic is unique in that it has lasted for much longer than typical natural disasters such as floods or bushfires. Most workers in Australia worked from home during lockdown and many children were also spending more time at home, causing a disruption to many households’ usual routines. Connecting with family and friends has become difficult, if not impossible, for many since the pandemic. Rates of domestic violence during the COVID-19 pandemic increased dramatically.12
During lockdown, rates of solitary drinking at home increased, with people reporting a tendency to not monitor their alcohol intake given the usual restraints such as driving home from licensed venues was no longer a concern. Traditionally, solitary drinking has been associated with more alcohol-related harm.13 One NSW study found that people who increased their alcohol intake during lockdown continued to drink excessively even once lockdown restrictions were eased.14
The GP consultation
Around one in four Australians delayed seeing a GP during the height of the COVID-19 pandemic.15 GPs in Australia reported fewer face-to-face consultations since the pandemic, with most consultations conducted via telehealth.16 Telehealth consultations have a number of benefits, particularly for patients in rural or remote areas, such as increasing access to care. Telehealth consultations also limit unnecessary travel and reduce community transmission of COVID-19 and other diseases. However, there are numerous barriers to consultation including privacy concerns, access issues for patients without internet or technology and the fact that some procedures such as pathology or physical examinations necessitate a face-to-face consultation.
Despite this, GPs are well placed to assess and screen for alcohol problems given that 83% of the population visited a GP in 2019-2020.15 GPs play a pivotal role in identifying alcohol problems as well as providing advice to patients on how to reduce or abstain from alcohol and monitor their alcohol use (Box 1).
{kind=link}
Screening and identifying alcohol use disorder
Patients rarely present to a GP specifically to request assistance with their alcohol use. As recommended by the RACGP’s Red Book, GPs should screen every patient for alcohol misuse, even if they do not suspect alcohol misuse. The Alcohol Use Disorders Identification Test for Consumption (AUDIT-C) is a brief three-item scale that can be integrated into routine history taking during a standard consultation (Table) along with information on what constitutes a standard drink.17 This rapid screener has been developed by the World Health Organization and has been extensively validated in Australian populations. The AUDIT-C can be administered in a nonjudgemental way to enable open discussion of the patient’s alcohol use, especially with patients who may be reluctant to freely discuss their drinking. Total AUDIT-C scores above 4 in men and 3 in women warrant a further comprehensive assessment of alcohol use using the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition) criteria for alcohol use disorder (AUD).18
{kind=link}
Comprehensive assessment of alcohol use
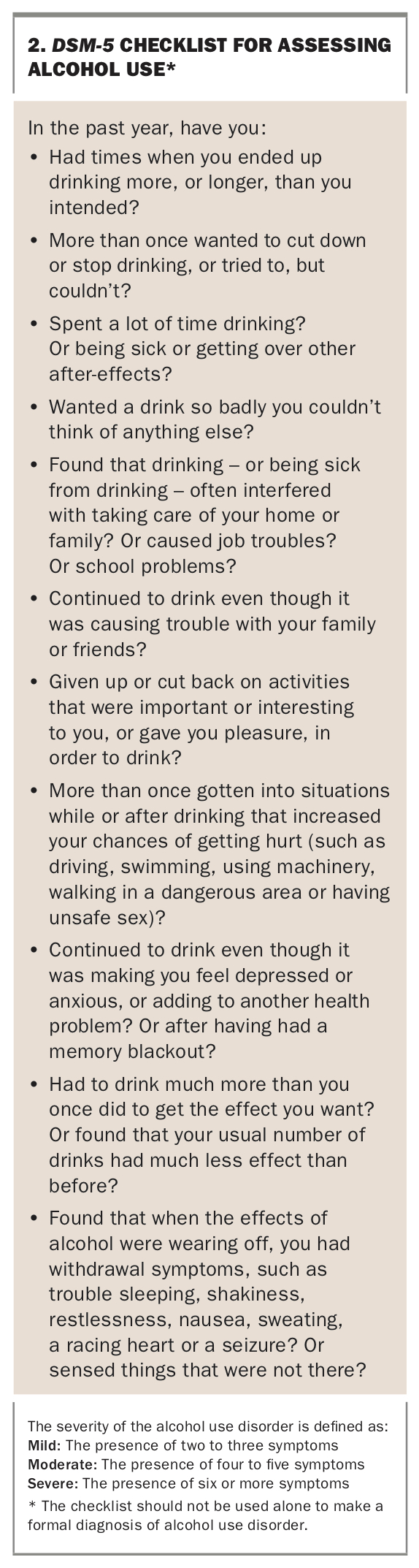
GPs should ask the patient each of the 11 items in the DSM-5 checklist (Box 2) in order to provide a more in-depth assessment of the patient’s alcohol use. The presence of two or more items from the DSM-5 checklist suggests AUD; however, the results from this checklist should not be used alone to make a formal diagnosis of AUD. In addition to the DSM-5 checklist, GPs should gather information on the patient’s typical daily use of alcohol, including quantity and frequency of alcohol use as well as identifying any triggers to drink (e.g. low mood, boredom). The Australian Guidelines for Treatment of Alcohol Problems provides further information on assessment and treatment options.19
{kind=link}
Readiness to change alcohol use
The results of the DSM-5 checklist should be fed back to the patient in a neutral, nonjudgemental manner, keeping in mind that ambivalence on the patient’s part is normal. Principles of motivational interviewing should be used when discussing the patient’s alcohol use. Regardless of the patient’s results on the DSM-5 checklist, the GP should keep in mind that not all patients will consider their drinking to be problematic, nor will they necessarily be ready to change their drinking habits right now. One quick way to determine how ready patients are to change their drinking is to ask:
‘How ready are you to change your drinking right now out of 10, where 10 is ready to change now and 0 is not at all ready to change my drinking?’
If patients are clearly resistant to the idea of changing their alcohol use, respectfully acknowledge their decision and offer to be of assistance in future if they later choose to change their drinking.
If patients are ambivalent about changing their drinking, further assess the pros and cons of drinking versus changing their drinking habits, increase their belief in their ability to change and offer information about the effects of alcohol on their health if they agree to this.
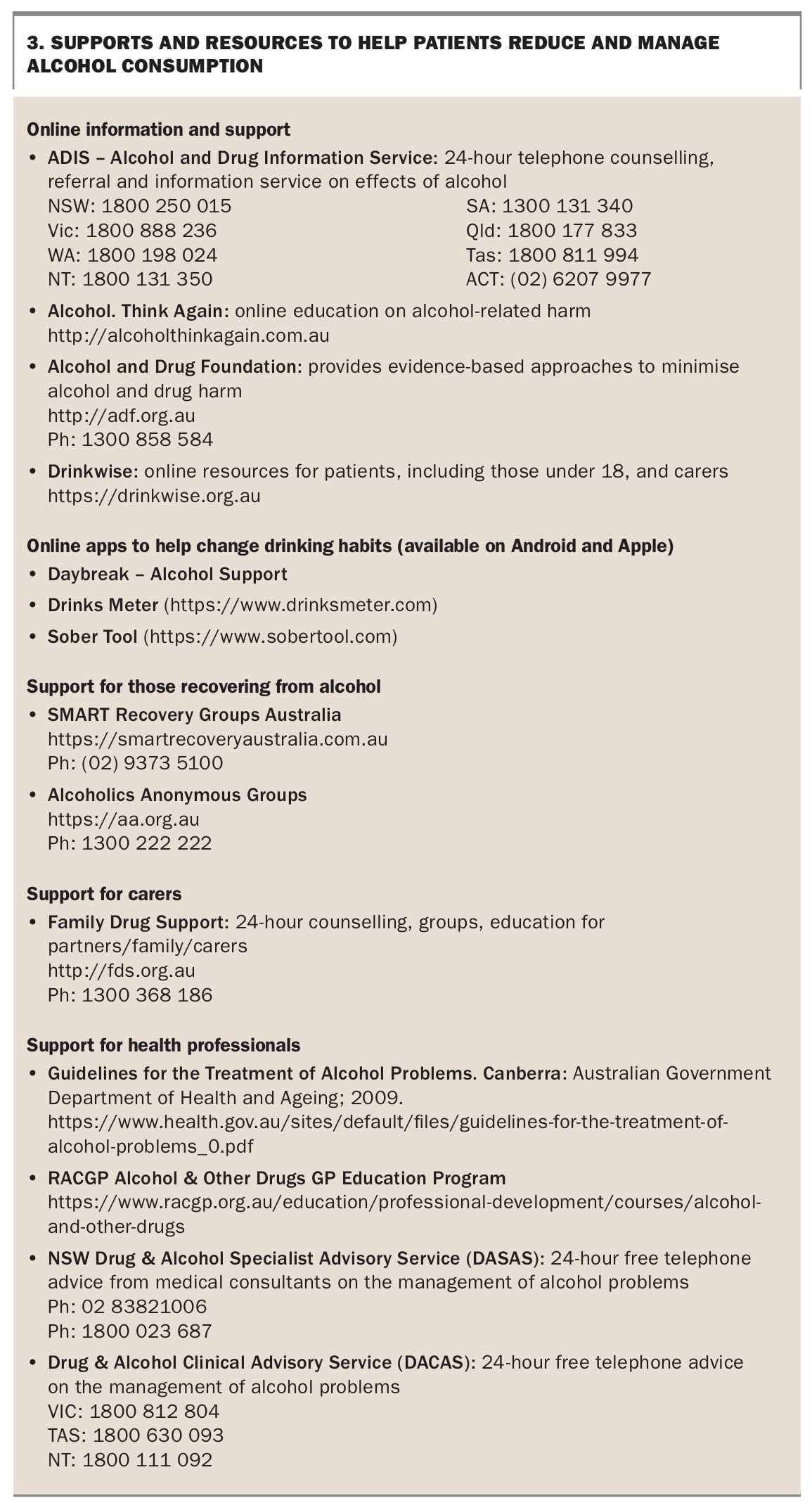
If patients are ready to change their drinking right now, offer advice and suggestions on how to achieve this and set concrete measurable drinking goals. There are a number of telephone and online support services for patients who wish to change their alcohol use, and for carers and treatment providers including GPs. Some of these resources are listed in Box 3.
{kind=link}
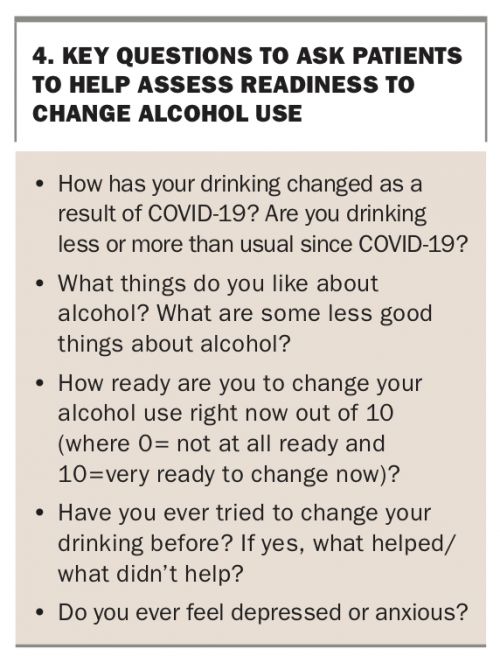
Other key questions to ask patients regarding their alcohol consumption during the COVID-19 pandemic are provided in Box 4.
{kind=link}
Comorbid mental health problems
Alcohol use and mental health problems often occur together, with depression and anxiety the most commonly co-occurring conditions.20 Globally, mental health has worsened during the COVID-19 pandemic. Increased rates of stress, anxiety, depression, post-traumatic stress disorder and insomnia have been reported, even among people without a pre-existing mental health problems.21-23 Rates of suicide have not increased since the pandemic in Australia as originally expected; however, rates of help-seeking for suicidal ideation increased dramatically during 2020.24
Given the negative impact of the COVID-19 pandemic on the mental health of people in Australia and the co-occurrence of mental health and alcohol problems, it is vital that GPs are prepared to assess and manage mental health problems in addition to alcohol use.
GPs can confidently ask about symptoms using mental health screeners, such as the Kessler Psychological Distress Scale (K10) and the Depression, Anxiety and Stress Scale 21 (DASS21), which can be used routinely to assess patients who overuse alcohol.25,26 The relationship between a patient’s level of social isolation and anxiety, depression and alcohol use may be assessed during consultations. GPs should also routinely assess suicide risk and implement suicide prevention plans for patients presenting with suicidal ideation.
Laboratory investigations
Elevated levels of the following biomarkers are only seen in a minority of patients with excessive alcohol use:
- serum gamma glutamyl transferase (GGT) level
- mean corpuscular volume (MCV)
- aspartate aminotransferase (AST) level.
Normal results do not exclude significant AUD. It is important for the patient to understand this may be a false reassurance as these tests do not identify alcohol-related damage to social function, mood, brain function or cardiovascular health.
Even when elevated, biomarkers may reflect nonalcohol-related pathology, but if AUD is confirmed, they do suggest liver disease or other physical toxicity. Results from the above tests can be used to motivate patients with AUD who may be ambivalent about moderating their alcohol intake, and appropriate biochemical testing should be considered before embarking on a goal of reduced drinking, to exclude significant health problems. If test results are abnormal, additional investigation may be warranted. Progress testing is very helpful in identifying response to intervention.
Specialised tests include the biomarkers carbohydrate deficient transferrin (CDT) and urinary ethylglucuronide (EtG). Both are readily available from major pathology providers but are costly because they are not covered by Medicare. They would normally be ordered according to directions from authorities such as the family court and professional regulators such as AHPRA.
Abnormal results for biomarkers can be used to raise concerns about alcohol use, especially when GPs suspect the patient may be under-reporting excessive alcohol use during consultations or on self-report measures (such as the AUDIT-C and DSM-5 checklist).
Physical examination
Signs of excessive alcohol consumption may be evident on physical examination. Common indicators of excessive drinking include, but are not limited to:
- signs of intoxication or withdrawal, which may be subtle
- hypertension
- conjunctival injection
- hepatomegaly and other signs of liver disease.
The presence of any of the above physical signs is not diagnostic of or essential to diagnosing AUD. Most patients with AUD have no abnormal physical findings. Only those with more severe AUD show signs of cognitive impairment and poor general presentation. Abnormal findings can be fed back to patients whom GPs suspect may be under-reporting their alcohol intake in order to encourage more open discussion about their drinking.
Management options
Pharmacotherapy for relapse prevention
GPs are well placed and trained to offer brief interventions for patients with mild to moderate AUD. For patients with moderate to severe AUD, numerous pharmacotherapy options are available for both abstinence and reduced drinking goals including acamprosate, naltrexone and disulfiram.
Withdrawal management
Patients who meet the criteria for severe AUD should not be advised to stop drinking abruptly given they likely to be physically dependent on alcohol and are at risk of experiencing potentially life-threatening withdrawal. Such patients would benefit from medicated detoxification that can be offered in primary care or via external referral to the appropriate specialist service. Outpatient withdrawal management uses long-acting benzodiazepines such as diazepam in a tapering dose with daily thiamine for five to seven days. Outpatient detoxification is not indicated in those without social support, or who have significant medical and mental comorbidities, seizure disorders, or a history of complicated withdrawal or failed withdrawal attempts.
Supportive counselling
Evidence suggests that patients are more likely to achieve their drinking goals if they combine pharmacotherapy with supportive counselling.27 Counselling teaches patients coping skills to manage high-risk situations in which they would typically drink, such as when depressed or bored. Due to the pandemic, counselling services are now typically delivered online via telehealth. Most support groups such as SMART Recovery and Alcoholics Anonymous groups are also being offered online during the COVID-19 pandemic.
Numerous mobile apps also exist to help patients manage their alcohol use and are listed in Box 3.
Conclusion
Alcohol use remains a significant cost and burden to patients and society. Given increased rates of alcohol use since the COVID-19 pandemic in Australia, it is vital that GPs take the time to routinely screen patients for possible alcohol misuse. GPs have the necessary skills to routinely screen, conduct a comprehensive assessment and devise a treatment plan for patients drinking excessively since the pandemic. MT