Skin lesions in darker skin phototypes

Pigmented skin is protected against UV damage and the development of certain skin cancers. However, some skin conditions are more prevalent in darker skinned communities, particularly Indigenous Australian communities. GPs should be aware that such patients are still at risk of developing skin cancer and early diagnosis and considered management are key to improving patient outcomes.
- Increased skin pigmentation is protective against UV radiation and development of skin cancers. There is, however, increased significance for trauma and chronic inflammation in the development of skin cancers.
- Although less common, skin cancers such as melanoma do occur in Indigenous populations but are diagnosed at a later stage. This results in significant hospitalisation and reduced survival.
- The risk of hyperpigmentation should be considered in the presentation and treatment of common skin conditions in pigmented skin.
- There is a higher prevalence of certain skin conditions including infectious diseases, systemic lupus erythematosus and discoid lupus erythematosus in Indigenous Australians.
- Awareness by GPs and patients of the risks of these skin lesions and conditions is important to improving outcomes for Indigenous patients.
Skin can be categorised into different phototypes based on richness of pigmentation. These are the Fitzpatrick skin types, ranging from type I fair skin (which always burns and never tans) to type VI darkly pigmented skin (Table 1).1 Darker skin phototypes (Fitzpatrick skin types IV to VI) display differences in incidence, presentation and management of many dermatological diseases compared with lighter skin phototypes.2 This article will discuss common skin conditions and how they present in darker skin phototypes, and the skin conditions that are more prevalent in the Australian Indigenous population.
{kind=link}
Skin cancers in darker skin phototypes
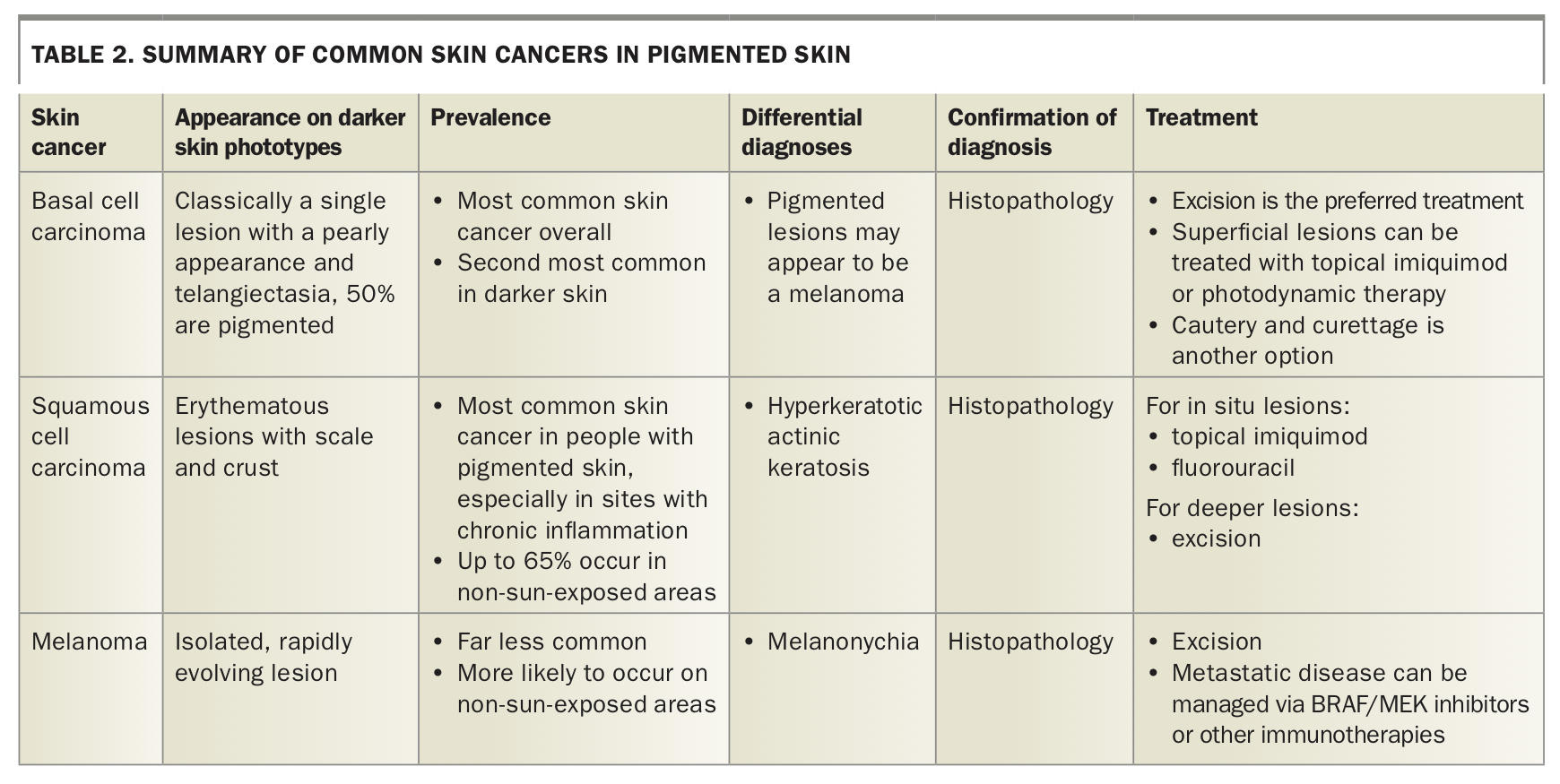
Increased levels of melanin and larger melanosomes in darker skin phototypes provide greater photoprotection that results in a lower overall incidence of skin cancers.2,3 The combined burden of melanoma and nonmelanoma skin cancers is thus lower in Australian and Torres Strait Islander peoples than the general Australian population, although it is still a very common cause for hospitalisation.4 In Indigenous patients, skin cancers account for 1% of deaths compared with 4% in the non-Indigenous population.4 A summary of the most common skin cancers in pigmented skin and their management is outlined in Table 2.
{kind=link}
Basal cell carcinomas
Basal cell carcinomas (BCCs) are the most common cancer overall in people with fair skin. In people with pigmented skin, increased levels of melanin offer UV protection, which results in a lower prevalence of BCC; however, this means that scarring, radiation and trauma have a greater role in carcinogenesis.2,5,6
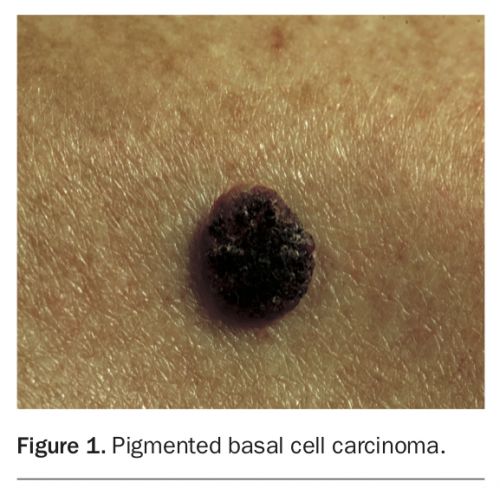
BCCs classically present as single, discrete lesions with a pearly appearance, rolled border and telangiectasia. In darker skin phototypes, they are often translucent with central ulceration.5 Half of BCCs that present in darker skin types may be pigmented (Figure 1) compared with 6% in lighter skin.5 It holds true that BCCs most commonly occur on sun-exposed areas.2
{kind=link}
Diagnosis is made via histopathology. Treatment modality is the same as with lighter skin types and includes topical imiquimod, topical fluorouracil, photodynamic therapy, cautery and curettage or excision.2 Exact treatment options depend on BCC site and histological subtype.
Squamous cell carcinomas
Squamous cell carcinomas (SCCs) are the most common skin cancer in dark skin phototypes.5 Classically, SCCs appear in areas exposed to UV light; however, in darker skin, up to 65% occur in non-sun-exposed areas.7,8 The most important risk factors for formation of SCCs are chronic inflammation and scarring.2,5
SCCs present as erythematous lesions with scale and crust in darker skin.7 Treatment modalities are the same as for lighter skin types and include topical imiquimod or fluorouracil for suitable in situ lesions, depending on site and other risk factors such as immune suppression, or excision for invasive lesions.2 Risk factors for metastasis in darker skin are cancers associated with scarring, discoid lupus erythematosus, non-sun-exposed areas, or involvement of the mucous membranes.2,9,10
Melanomas
Melanomas occur less commonly in pigmented skin; the incidence of melanoma in Indigenous Australians is lower compared with non-Indigenous Australians. However, survival rates for melanomas directly relate to disease extent at time of diagnosis, and thus early diagnosis is crucial. Unfortunately, melanoma is often diagnosed at a later stage in darker skin, resulting in reduced survival.2,11 This is attributed to less education around skin cancer in Indigenous and darker skinned communities, in contrast to the increased awareness across the population more broadly.2
Melanoma typically presents as an isolated, rapidly evolving pigmented lesion, although it may be hypomelanotic or amelanotic. It arises de novo or from an existing naevus. The most common sites in darker skin are non-sun-exposed sites, especially the palms and plantar or subungual surfaces (acral lentiginous melanoma).12 A clinical pearl is to look for the presence of Hutchinson’s sign – the extension of pigment into the proximal nail fold (Figure 2) – which occurs in a subungual melanoma and helps distinguish malignancy from benign melanonychia.5 Melanonychia is also more likely to involve multiple nails.
{kind=link}
Confirmation of diagnosis is via histopathology, with excision being the mainstay of treatment. Further management depends on the staging. There are many targeted molecular therapies and immunotherapies for advanced melanoma. Testing for BRAF gene mutation guides the decision-making. If positive, BRAF/MEK inhibitors are an effective treatment. Other therapies for advanced melanoma include immune checkpoint inhibitors but these have unpredictable toxicity.13
Acne
Acne is one of the most common skin conditions seen in outpatient clinics. Darker skin is more predisposed to postinflammatory hyperpigmentation, keloids and scarring than lighter skin, and hence acne warrants a discussion here.2
Acne presents similarly with open and closed comedones, papules, pustules, nodules and cysts.2 Initial acne therapies are the same for all skin phototypes, and include benzoyl peroxide, topical antibiotics and retinoids. Oral antibiotics can be used in moderate to severe acne. Isotretinoin is used for resistant nodular cystic acne. To help avoid postinflammatory hyperpigmentation, treatments that cause irritation or inflammation should be avoided in the treatment of pigmented skin.2 Retinoids can be commenced at lower doses and less frequent intervals (such as every second day). Benzoyl peroxide can be drying and irritating, therefore, using concentrations less than 5% can limit subsequent hyperpigmentation.2
For presentations of both acne and post-inflammatory hyperpigmentation, treatment with azelaic acid 15% or 20%, topical retinoids and chemical peels may be helpful.14-16 Last-line therapies include oral antibiotics, hormonal therapies (spironolactone, oral contraceptives) or isotretinoin.2
Postinflammatory hyperpigmentation
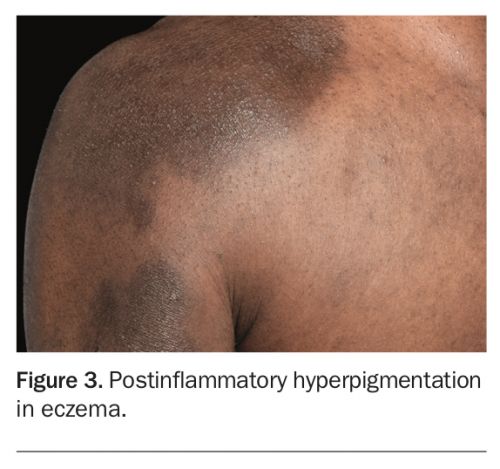
Post-inflammatory hyperpigmentation is more common in people with darker skin.17 It results from inflammation from a condition (such as eczema or acne) or from medication. Clinically, it presents as ill-defined hyperpigmented macules and patches in the distribution and shape of the original lesions (Figure 3). The exact colour of the hyperpigmentation depends on its depth in the skin, and can range from tan and brown to dark brown and then blue-grey as the pigmentation extends deeper.2
{kind=link}
The mainstay of treatment is control of the underlying disorder to prevent further inflammation. Hyperpigmentation will fade over six to 12 months, although this can take longer. Avoidance of sun exposure and the use of sunscreen to prevent darkening of hyperpigmented areas, as well as avoiding irritants such as medications, alcohol, fragrances and cosmeceuticals is also recommended.2,17
Optimal medical therapy involves hydroquinone 4%,17 although it has been linked to ochronosis (darkening of the skin).18 Other treatment options include retinoids, azelaic acid, chemical peels, corticosteroids, or a combination of these. There is also emerging evidence for topical tranexamic acid in improving hyperpigmentation.19
Common skin conditions affecting Indigenous Australians
It is well known that Indigenous Australians bear a disproportionately high burden of disease compared with non-Indigenous Australians. Skin disease contributes to this high burden, constituting roughly 15% of consultations between Indigenous Australians and primary healthcare practitioners.3,20 Skin problems in Indigenous communities predominantly result from infectious diseases. The most common noninfectious skin diseases include vitamin D deficiency, systemic lupus erythematosus and discoid lupus erythematosus are more prevalent, while psoriasis and type I hypersensitivity disorders are less common.3
Infectious diseases
Infectious diseases make up a higher burden of disease in the Indigenous population, which is likely to be due to socioeconomic determinants of health such as economic inequities, living conditions and overcrowding and access to healthcare in remote communities.21,22 One study of Indigenous patients attending dermatology clinics found that fungal infections were the most common type of skin infection, followed by viral, parasitic and bacterial infections.20
The most common dermatophyte in central and northern Australian communities is Trichophyton rubrum.21 Other Trichophyton species and Malassezia furfur, which causes pityriasis versicolor, are also common.21,22 Pityriasis versicolor responds to topical selenium sulphide or imidazoles such as clotrimazole or miconazole.21,22 Tinea corporis or unguium, or simply more widespread disease may require oral griseofulvin or terbinafine.21
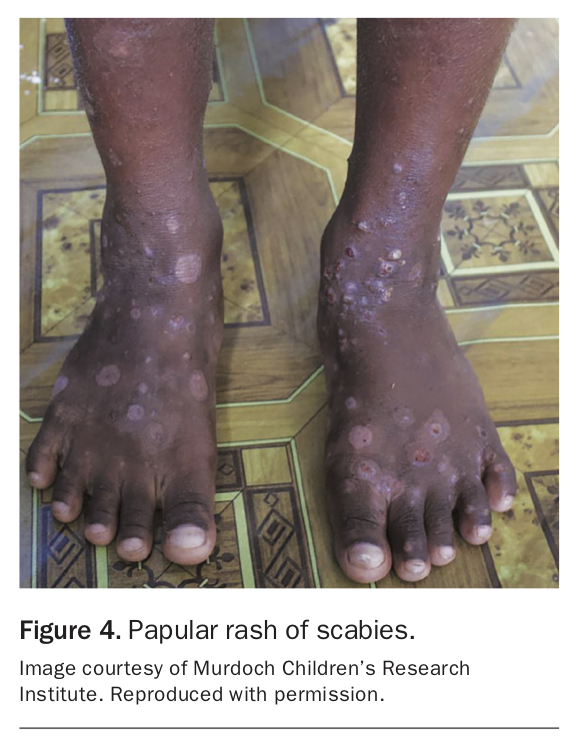
Sarcoptes scabiei is endemic in many remote Aboriginal communities with scabies and is prevalent in up to 50% of children and 25% of adults (Figure 4).21 In these communities, scabies may be associated with 50 to 70% of streptococcal pyoderma.23 Treatment with 5% permethrin is highly effective and has been used effectively in public health settings for whole communities.21 Whole-community treatment has the additional benefit of halving the prevalence of pyoderma.21 Crusted scabies may require oral ivermectin.24
{kind=link}
Streptococcal pyoderma affects up to 70% of children in Indigenous communities and has the sequelae of post-streptococcal glomerulonephritis and acute rheumatic fever.21 Streptococcus pyogenes, a Group A streptococcus, is the primary pathogen in up to 80% of cases.21 Streptococcal pyoderma has an excellent response to treatment with benzathine penicillin.21,22
Common viral infections are Herpes simplex, which may require treatment with aciclovir, and Molluscum contagiosum, which is likely to resolve spontaneously with no need for treatment.20,22
Systemic lupus erythematosus and discoid lupus erythematosus
The prevalence of systemic lupus erythematosus in Indigenous patients is 2.1 to 3.8 times higher than in non-Indigenous patients.3,25,26 Indigenous people also tend to have a higher morbidity and mortality, which may relate to later presentation.26
Discoid lupus erythematosus has also been reported to have a higher prevalence in Indigenous communities compared with non-Indigenous communities.27 The cause for this higher prevalence is uncertain, although it has been postulated that it may be due to higher rates of infections through the induction of cross-reactive anti-double stranded DNA antibodies, via the super antigen effect, or the result of increased environmental UV light exposure leading to exacerbation of subclinical lupus.25,28
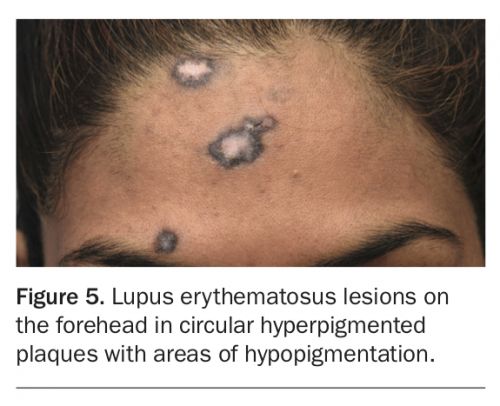
Discoid lupus erythematosus presents as sharply demarcated circular hyperpigmented plaques with peripheral erythema and scale (Figure 5). There is a propensity for it to occur on the lips, and there is an association with SCCs at this site.3,29
{kind=link}
Vitamin D deficiency
Although the increased melanin content of pigmented skin may be protective against skin cancer, it unfortunately results in enhanced susceptibility to vitamin D deficiency. Vitamin D is obtained through UVB exposure, and deeper skin pigmentation requires longer exposure of UVB to synthesise adequate amounts of vitamin D.30 Average levels of 25-hydroxy vitamin D levels have been found to be low in Indigenous populations.31
Vitamin D deficiency has been associated with chronic diseases such as diabetes and heart disease.32 There is also some evidence to suggest a link between low vitamin D levels and high body mass index.33,34 Maintaining adequate vitamin D levels, particularly in remote Indigenous communities where access to emergency health services may be lacking, is therefore important to not only prevent falls and risk of fracture, but also to reduce the risk of chronic and cardiometabolic disease.
Psoriasis and eczematous conditions
Although less common in Indigenous patients, it is instructive to note the appearance of these disorders on darker skin phototypes. Psoriasis tends to form violaceous rather than red/pink plaques, with grey rather than white scale. There is more pronounced postinflammatory hyper- and hypopigmentation.35 As for eczematous conditions, erythema may present as subtle hyperpigmentation. There is also increased prominence of postinflammatory hyper- and hypopigmentation. Follicular papules may be more common.36 The correct diagnosis may rely on nonpigmentary aspects of the lesions.
Conclusion
Darker skin phototypes are protective against the development of skin cancers. However, dark skinned populations, in particular Indigenous Australians, are still at risk of developing skin cancers and other skin conditions. Greater awareness and recognition of the risks to Indigenous populations and implementation of preventative strategies are required to improve early diagnosis in these communities. Certain diseases have a higher prevalence in Indigenous Australians, and requires careful consideration of diagnosis and management. MT