Scalp pain and tenderness: early features of temporal arteritis

Temporal arteritis, a panarteritis occurring in the older population, with female predominance, may present with localised scalp pain and tenderness. The triad of visual disturbances, jaw claudication and new-onset headache, also in combination with scalp symptoms and signs, should arouse suspicion of temporal arteritis. The patient’s sight and life may be preserved by early diagnosis and management.
- This article describes three patients with biopsy-proven temporal arteritis, all of whom presented with scalp symptoms and signs before developing vision loss.
- To prevent sight- and life-threatening complications, early diagnosis and emergent management of temporal arteritis with corticosteroids are of paramount importance.
- The classic triad of symptoms of temporal arteritis comprises new-onset headache, visual disturbance and jaw claudication; however, scalp pain and tenderness can be early features of this condition and recognition of these can aid the clinician in making an early diagnosis.
- Awareness of the differential diagnoses for scalp pain and tenderness assist the diagnosis.
- A template summarising the 42 symptoms and signs of temporal arteritis, including three newly recognised signs, is useful for guiding diagnosis.
- Temporal arteritis is optimally managed using a multidisciplinary approach with input from the GP, a rheumatologist, an ophthalmologist and a pathologist.
Temporal arteritis (TA), also known as giant cell arteritis, is an immunologically based granulomatous panarteritis of large and medium-sized vessels that occurs among the older population with a female preponderance.1 Its diagnosis is important because, if missed, patients may rapidly become blind or even die from their disease. Thus, prompt recognition and management can be sight- and life-saving.
The classic triad of new-onset headache, visual disturbance, such as diplopia (double vision) or amaurosis fugax (transient unilateral loss of vision in either eye), and jaw claudication is key in making the clinical diagnosis of TA. However, scalp pain and tenderness are also important features of TA.
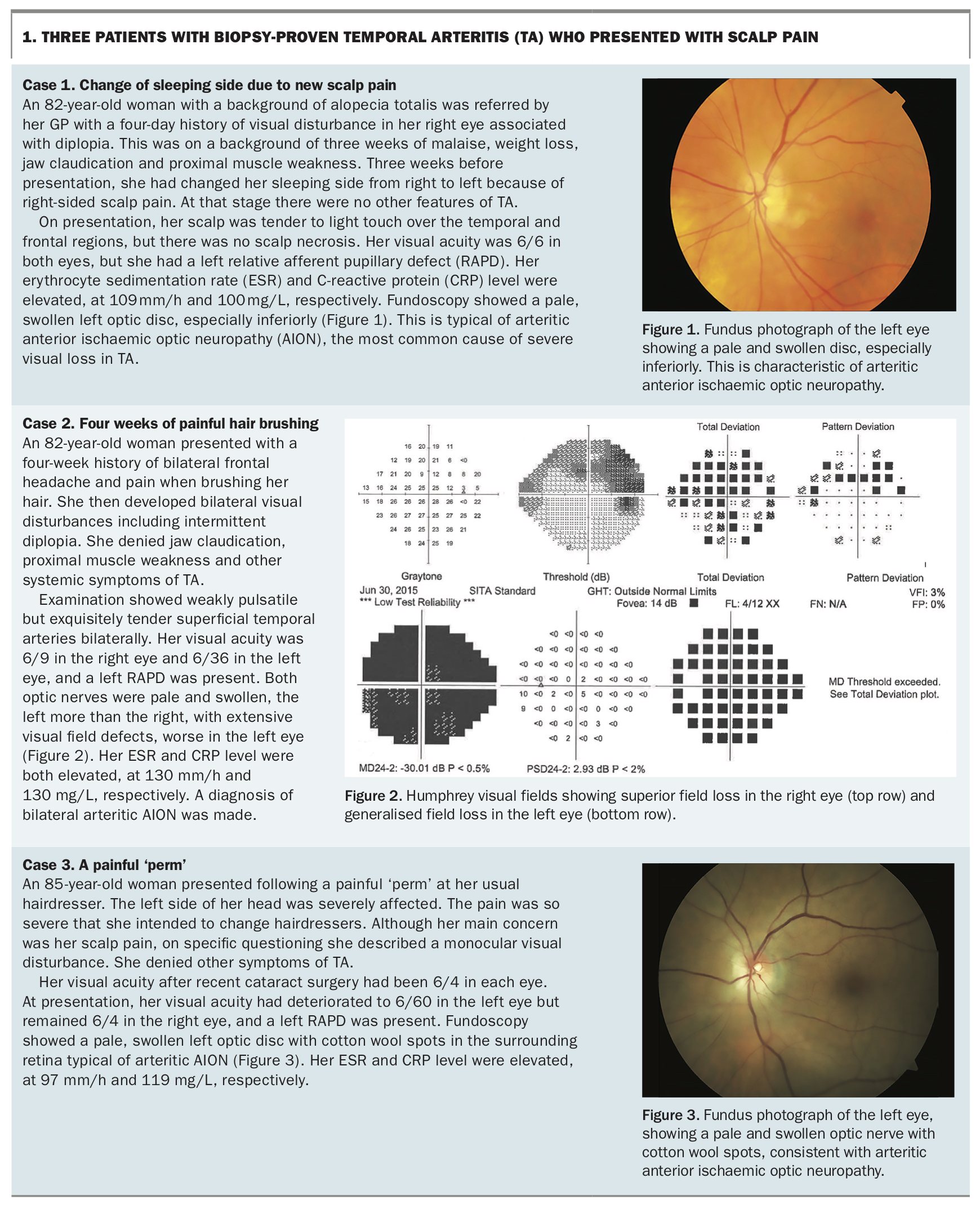
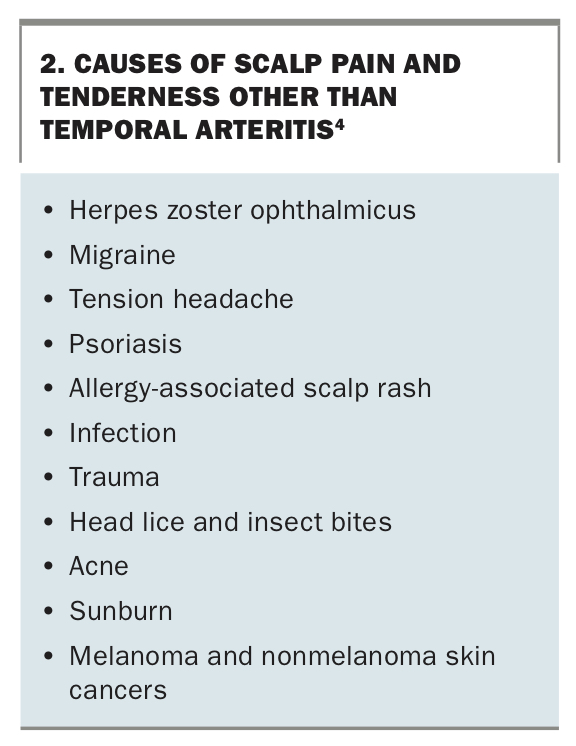
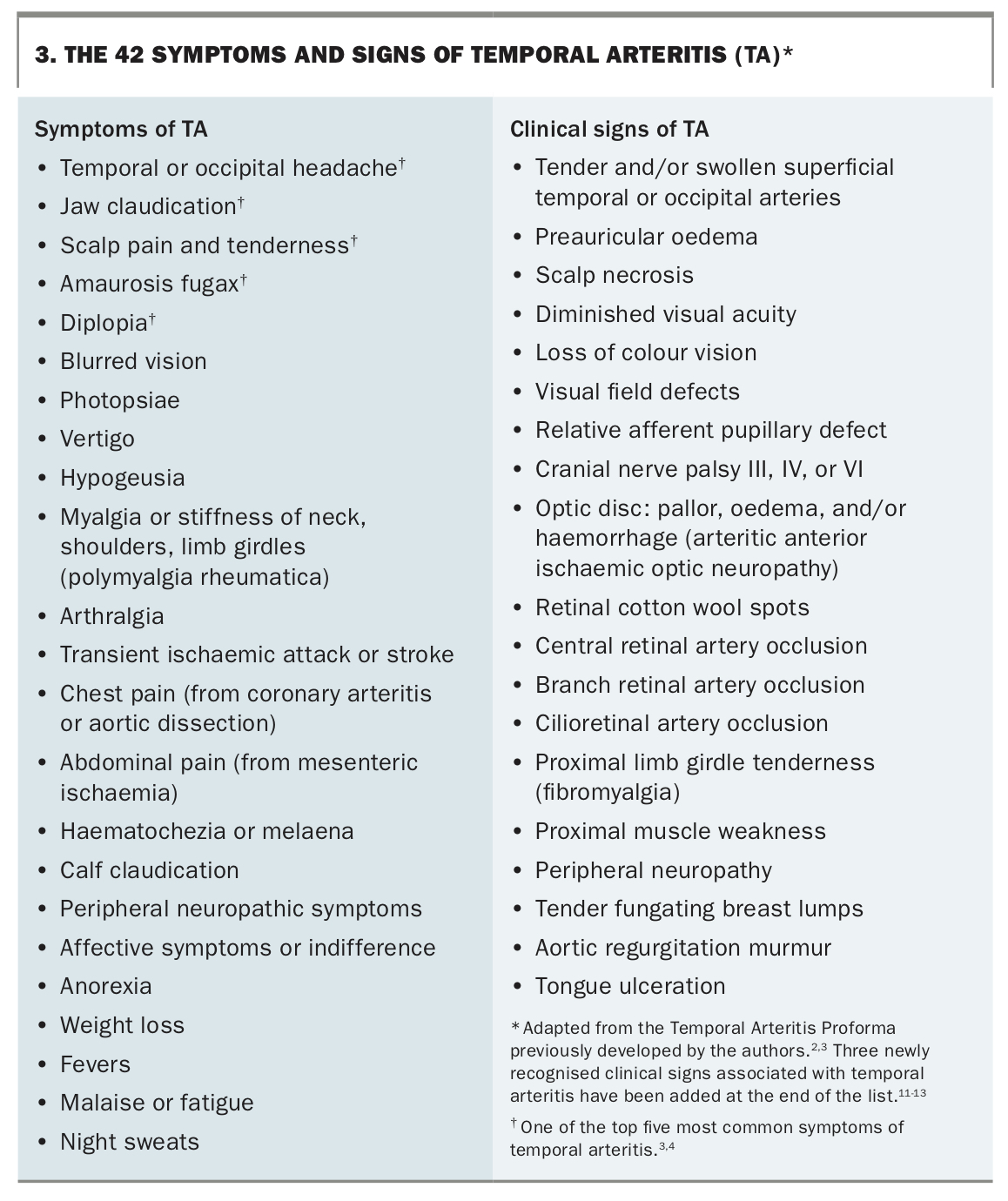
This article describes three patients with biopsy-proven TA who presented with a variety of scalp symptoms and signs (Box 1 and Figures 1 to 3). The differential diagnosis of scalp pain and tenderness is highlighted, and guidelines on the definitive diagnosis of TA are included, which may assist the clinician in making a clinical diagnosis of TA rapidly and confidently.2,3
{kind=link}
Scalp symptoms and signs of TA
The three cases in Box 1 highlight that scalp pain and tenderness can be not only the early features of TA, but the reason for patients presenting for diagnosis. However, there are various other causes of scalp pain and tenderness (Box 2).4 Most of the other disorders are not rapidly sight- or life-threatening.
{kind=link}
In patients with TA, scalp pain and tenderness are usually localised over the cranial branches of the external carotid arteries, particularly the superficial temporal and occipital arteries, which are often exquisitely tender.5 It can be useful in some patients to demonstrate to them the significant tenderness they experience when an involved artery is digitally compressed, compared with the normal response to compression of the artery in another person.
In TA, an inflammatory cascade occurs, which may result in vascular ischaemia of the scalp, rendering the scalp hypersensitive to minor stimuli, as in the three cases described.5 Patients typically state that brushing their hair engenders new pain in the scalp. They may also state that because of scalp pain, they have changed their sleeping side.
By the time of definitive diagnosis of TA, which is made by histopathological analysis of the superficial temporal artery biopsy specimen, some patients may have already developed scalp necrosis.6 Spontaneous scalp necrosis is well documented in the literature, and may precede TA and its recognition.4,6,7 Reflecting the pathogenesis of scalp necrosis, our group has noted abrupt termination of the superficial temporal artery in the scalp during a superficial temporal artery biopsy in a patient in whom the biopsy confirmed TA.8
Steps to clinical diagnosis of TA
Symptoms that are strong predictors for a positive TA diagnosis include jaw claudication, visual disturbances (diplopia and amaurosis fugax) and new-onset headache that may be associated with scalp pain and tenderness.4-6,9
In TA, jaw claudication results from masseter muscle ischaemia. It is characterised by jaw pain that develops with or soon after chewing and subsides with rest. Asking a patient to chew gum is a simple method of evaluating jaw claudication;6 however, the patient can otherwise be asked to open and close the jaw rapidly and forcefully 20 to 30 times.
Amaurosis fugax may affect one or both eyes and is characterised by a partial or complete visual field defect, often described by patients as being like a curtain closing and opening. The visual loss spontaneously resolves after a few minutes.
The headache in TA is typically new and located over the temples but may also be frontal, occipital or generalised, and is usually bilateral.9 More than two-thirds of patients experience such headaches, which can be associated with tenderness of the scalp, for example while brushing the hair (Box 1, Case 2). Unilateral headaches are uncommon in TA; however, they may prompt patients who experience them to sleep on the opposite of their preferred side, especially if there is associated unilateral scalp tenderness (Box 1, Case 1). We observed a recent case of a patient with biopsy-proven TA in whom the superficial temporal and occipital arteries, bilaterally, were visibly dilated and exquisitely tender, standing out like ‘fingers’ in the patient’s frontal and suboccipital regions.
Our comprehensive proforma of the 23 symptoms and 19 signs of TA is provided in Box 3.2-4,10-13 The last three signs have been added since the proforma was originally published: tender fungating breast lumps mimicking breast cancer, the murmur of aortic regurgitation and tongue ulceration.11-13
{kind=link}
Practical guidelines for diagnosis and treatment of TA
Diagnosis of TA
The diagnosis of TA is made clinically, and the initiation of treatment should never be delayed for the purpose of performing diagnostic investigations, especially in the presence of vision loss. Visual acuity should be assessed in each eye because of the risk of bilateral vision loss. Vision loss may not be ipsilateral to the side of the headache.14 Urgent same-day measurement of ESR and CRP levels and platelet count should be carried out, all of which are usually elevated in TA.
A superficial temporal artery biopsy is still the diagnostic gold standard, and we aim to obtain 20 to 25 mm of artery. We also recommend that if an adequate biopsy has been performed and the histopathology is negative for TA, then corticosteroid therapy for TA can be stopped immediately. This spares the patient from the side effects of unnecessary high-dose corticosteroid therapy, which occur especially in the first few weeks. An explanation for the patient’s clinical presentation needs to be further sought, often by the GP in conjunction with a rheumatologist. Further, if there is still real concern about the clinical diagnosis of TA, the pathologist can be asked to confirm the diagnosis by re-reviewing the histopathology or examining more sections. This is because a negative biopsy precludes TA, but suggests that other arteritic processes, or possibly systemic neoplasia or infection, may be present.
Recently, positron emission tomography-CT has been recommended as being diagnostically useful in TA. Its place is not yet clear, but we consider it may have a major role in diagnosing recurrent TA.15
The clinician and the operating surgeon should remember that removing a section of superficial temporal artery could cause a brainstem stroke. This may occur if the internal carotid artery is already occluded, leading to the patient’s intracranial arterial supply being provided by branches of the external carotid artery (typically the superficial temporal arteries) with retrograde flow intracranially along the supraorbital vessels. Stroke can be prevented by delineating the superficial temporal artery intended for biopsy and occluding it by digital pressure for one minute. If the patient becomes anarthric or loses consciousness, biopsy of that artery is precluded. In our experience, a good technique during arterial compression is to ask patients to recall their life story from birth, which allows the one minute to pass quickly.
Treatment of TA
Patients without visual disturbances at diagnosis should be commenced immediately on oral prednisone 1 mg/kg once daily to a maximum dose of 100 mg daily. By contrast, if any visual disturbance is present, then immediate pulsed intravenous methylprednisolone at a dose of 500 to 1000 mg once daily for three days is recommended. This is followed by oral prednisone at 1 mg/kg once daily, depending on the patient’s progress. TA is optimally managed by a multidisciplinary team with input from the GP, a rheumatologist, an ophthalmologist and a pathologist.
Although methotrexate has traditionally been used as a corticosteroid-sparing agent, recently tocilizumab has been shown to be therapeutic in patients with TA in clinical trials, and is now listed on the PBS.16 Furthermore, worldwide trials of upadacitinib, a janus kinase-1 selective inhibitor, have been commenced in patients with TA, with Australian centres included.
Conclusion
Scalp pain and tenderness may present early in the course of TA. Presentations to GPs with symptoms and signs of TA, and especially with otherwise unexplained scalp pain, tenderness and ulceration, should prompt investigation to exclude TA. If the patient has the triad of new headaches, jaw claudication and visual disturbance, a high index of suspicion for the diagnosis of TA must be considered. Immediate and appropriate management at this point may prevent loss of sight and loss of life. MT