Retinal tear and detachment: the importance of early diagnosis

GPs are well placed to recognise, and should maintain a low threshold of suspicion for, the symptoms of retinal detachment, including flashing lights, visual floaters and a shadow in the peripheral visual field. Prompt referral of patients for diagnosis and surgical treatment is essential for successful outcomes and to prevent possible blindness.
Retinal tear and detachment are common, particularly in older populations and those with a history of ocular conditions. Awareness of retinal detachment is low among the general population; therefore, people may not be cognisant that initial visual symptoms, such as flashing lights or floaters, can indicate a more serious underlying ocular condition.
As the first point of contact for many people experiencing visual disturbance, GPs are well placed to recognise relevant symptoms of retinal detachment and initiate early referral for diagnosis. Many patients may also consult their GP after diagnosis with questions regarding management and postoperative care (Box 1). This article briefly outlines the causes, symptoms and treatment for retinal tear and detachment to help guide GPs.
{kind=link}
Anatomy of the eye
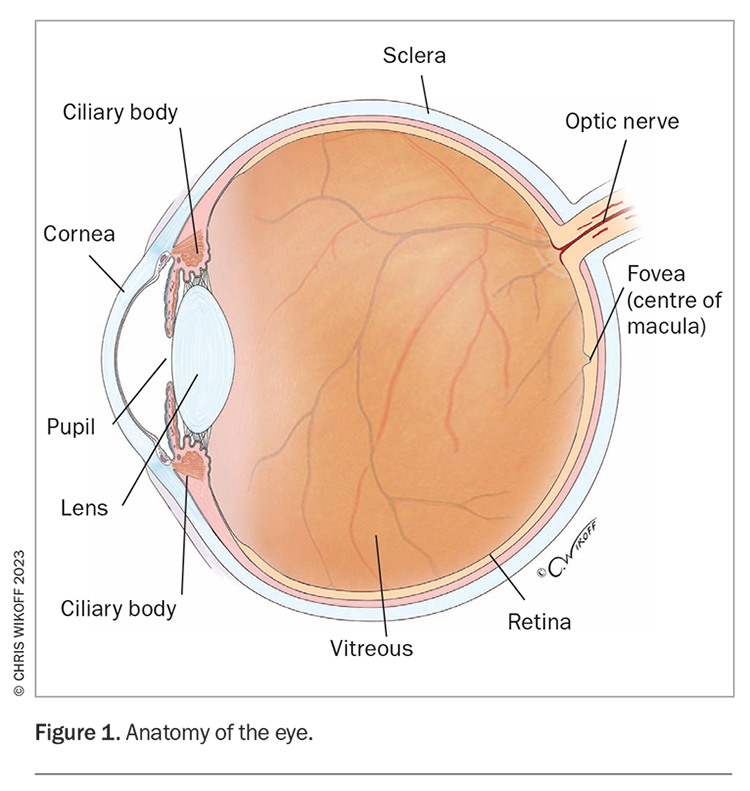
The retina is the light-sensitive neural layer lining the inside of the back of the eye and houses the macula, which is responsible for detailed central and colour vision (Figure 1). The vitreous contains a collagen network of fluid with a stiff, gel-like consistency that fills the inside of the eye and is attached to the retina. Lattice degeneration, characterised by areas of retinal thinning, occurs near the ciliary body in 6 to 8% of the general population and may predispose to retinal detachment.1 However, lattice degeneration often goes undetected as patients with the condition are usually asymptomatic.
{kind=link}
Retinal detachment
A retinal detachment occurs when the retina lifts away from its normal position against the inside of the back of the eye. The detached retina becomes deprived of nutrients from choroidal circulation and loses function, resulting in scotoma, or loss of vision, in the area of the retinal detachment.
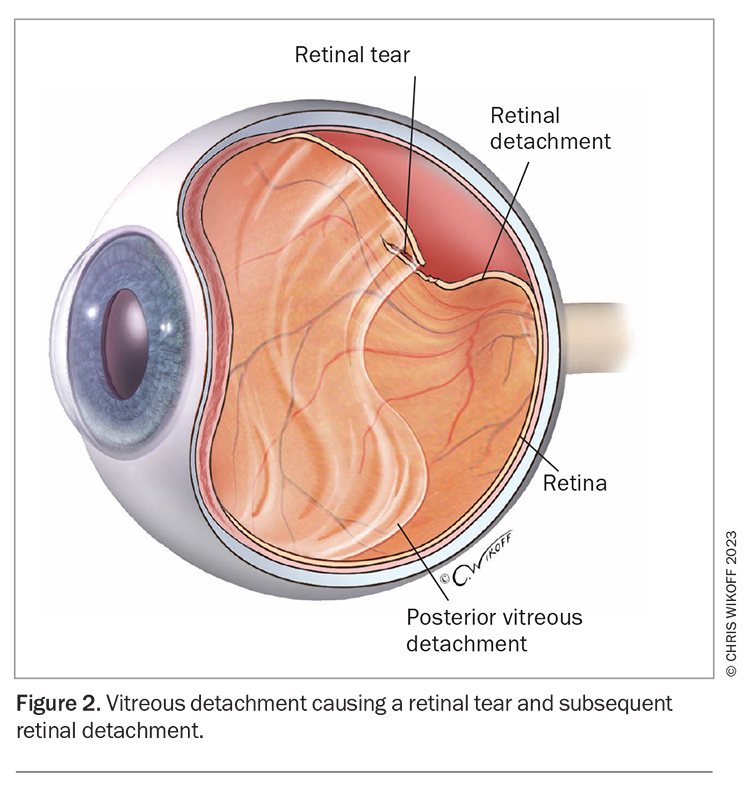
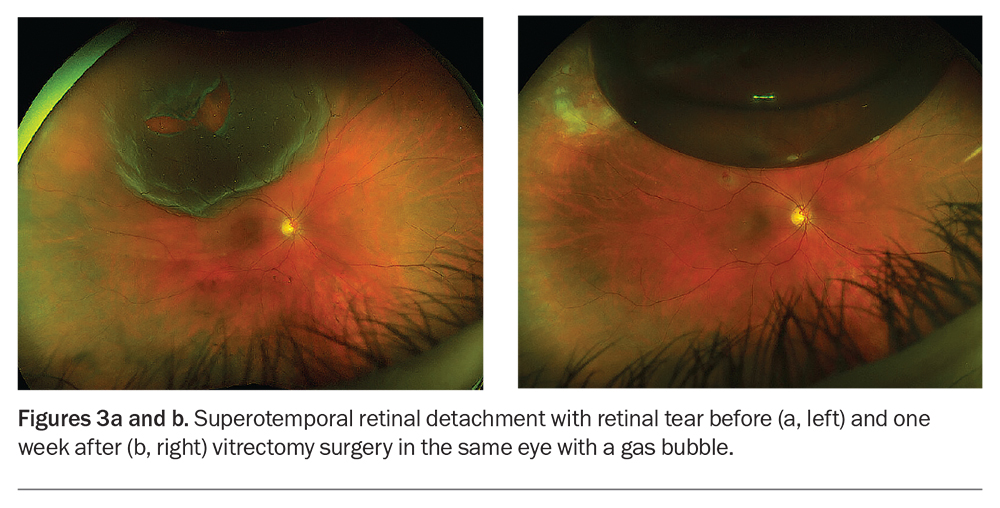
Vitreous syneresis occurs with age, as the vitreous becomes more fluid due to loosening of its collagen framework, and often results in posterior vitreous detachment (PVD), whereby ‘sloshing’ of the vitreous gel with eye movement causes the vitreous to separate from the surface of the retina as the collagen structure collapses (Figure 2). In most cases, PVD can cause frustrating symptoms, such as floaters, but does not result in significant visual problems. However, in areas of the retina with strong vitreous attachment, the resulting vitreous traction may be significant enough to tear the retina through its full thickness. The fluid inside the eye then passes through the retinal tear and lifts the retina, resulting in a retinal detachment causing an enlarging visual scotoma (Figures 3a and b). Factors that increase the risk of retinal tears and detachment are listed in Box 2. If untreated, the retina may completely detach resulting in blindness. A retinal tear and detachment may also result in vitreous haemorrhage from a ruptured retinal vessel.
{kind=link}
{kind=link}
{kind=link}
Important symptoms
Floaters
Floaters result from the collapse of the vitreous gel, resulting in areas of condensed collagen fibrils. Patients may find floaters more noticeable when they are looking at a white-coloured background, such as white paper or computer screens, or against the sky, snow and sea. A sudden increase in the number of larger floaters may indicate vitreous haemorrhage from retinal tear or detachment. The presence of floaters may be associated with anxiety, depression and reduced, vision-related quality of life.2
Flashes of light
Flashes of light (photopsia) occur when the collapsed vitreous pulls away from the light-sensitive retina, resulting in physical retinal stimulation. The typical symptoms are brief intense lightning-like flashes, usually seen in the dark and with rapid head or eye movement, such as when turning the head in reversing a car at night.
Dark shadow or grey curtain
A peripheral enlarging area of darkness (scotoma) is the classic symptom of a retinal detachment. If untreated, a small retinal detachment will progress to a total separation of the retina, including the macula, resulting in complete blindness.
Patient review and referral
In most cases, vitreous detachment remains uncomplicated and is not vision-threatening; however, about 10% of vitreous detachments may be associated with a vitreous haemorrhage, retinal tear or retinal detachment. Therefore, patients with a vitreous detachment should be reviewed promptly after the initial onset of symptoms.
Patients with a vitreous detachment should be educated on the symptoms of retinal detachment and advised to seek urgent medical attention if symptoms change. They should be warned to look out for: new or acute changes in flashes and floaters; a shadow, or scotoma, starting in the peripheral visual field, the development of which requires immediate referral; and reduced central visual acuity.
Patients should be referred for further immediate assessment, preferably on the same day, if they have evidence of any of the following:
- new or persisting symptoms of photopsia and floaters
- vitreous haemorrhage (as judged by a sudden increase in large floaters)
- a high risk of having a retinal detachment (as judged from their history, including a past or family history of retinal detachment, high myopia or previous ocular trauma)
- extensive thinning of the retina, such as lattice degeneration on imaging.
Diagnosing a retinal detachment
Retinal tears and detachment are diagnosed on clinical examination using slit lamp biomicroscopy and indirect ophthalmoscopy. Adequate imaging of suspected retinal detachment cannot be obtained using a direct ophthalmoscope, even when the examiner is competent in using this instrument. Widefield retinal cameras are useful in photographing the peripheral retina and identifying areas of retinal weakness, tears, holes and retinal detachment. In some patients, B-scan ultrasonography is used to show the position and mobility of the vitreous.
Treating tears and detachments
Retinal tears
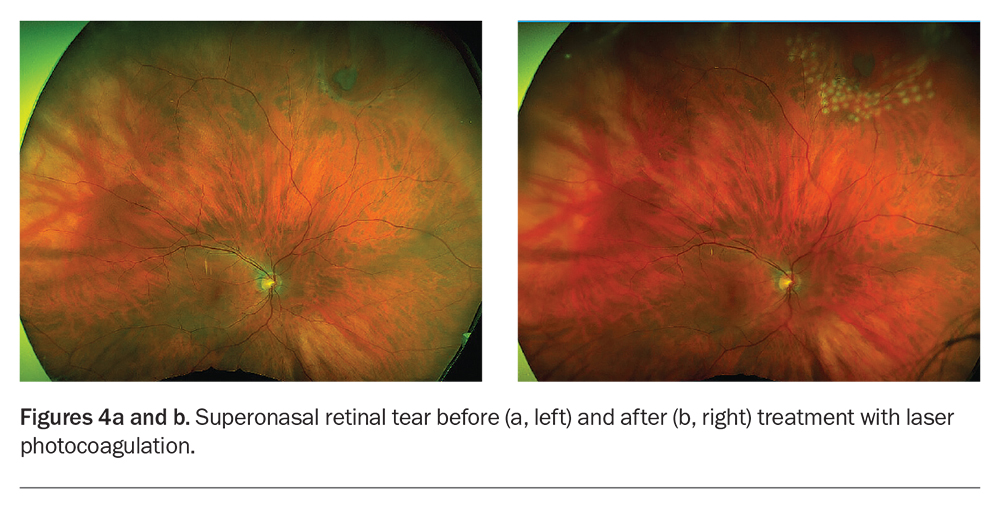
Retinal tears are usually treated in a clinic using laser photocoagulation. The aim of laser treatment is to surround the area of the tear with laser burns that then induce the formation of small scars, thereby attaching the retina more securely to underlying tissue (Figures 4a and b). If the tears are obscured by vitreous haemorrhage, have surrounding subretinal fluid or are located too far in the retinal periphery to be easily seen or reached by a laser, patients may need treatment with externally applied, transconjunctival/scleral cryotherapy, which is undertaken in an operating theatre.
{kind=link}
Retinal detachment
There are several ways to repair a retinal detachment, depending on the characteristics of the detachment. In each of the methods below, the surgeon locates the retinal tear and seals it using laser or cryotherapy during the retinal detachment operation. Generally, the retina is attached back onto the inner wall of the eye, then the tear is treated with laser or cryotherapy.
Vitrectomy surgery
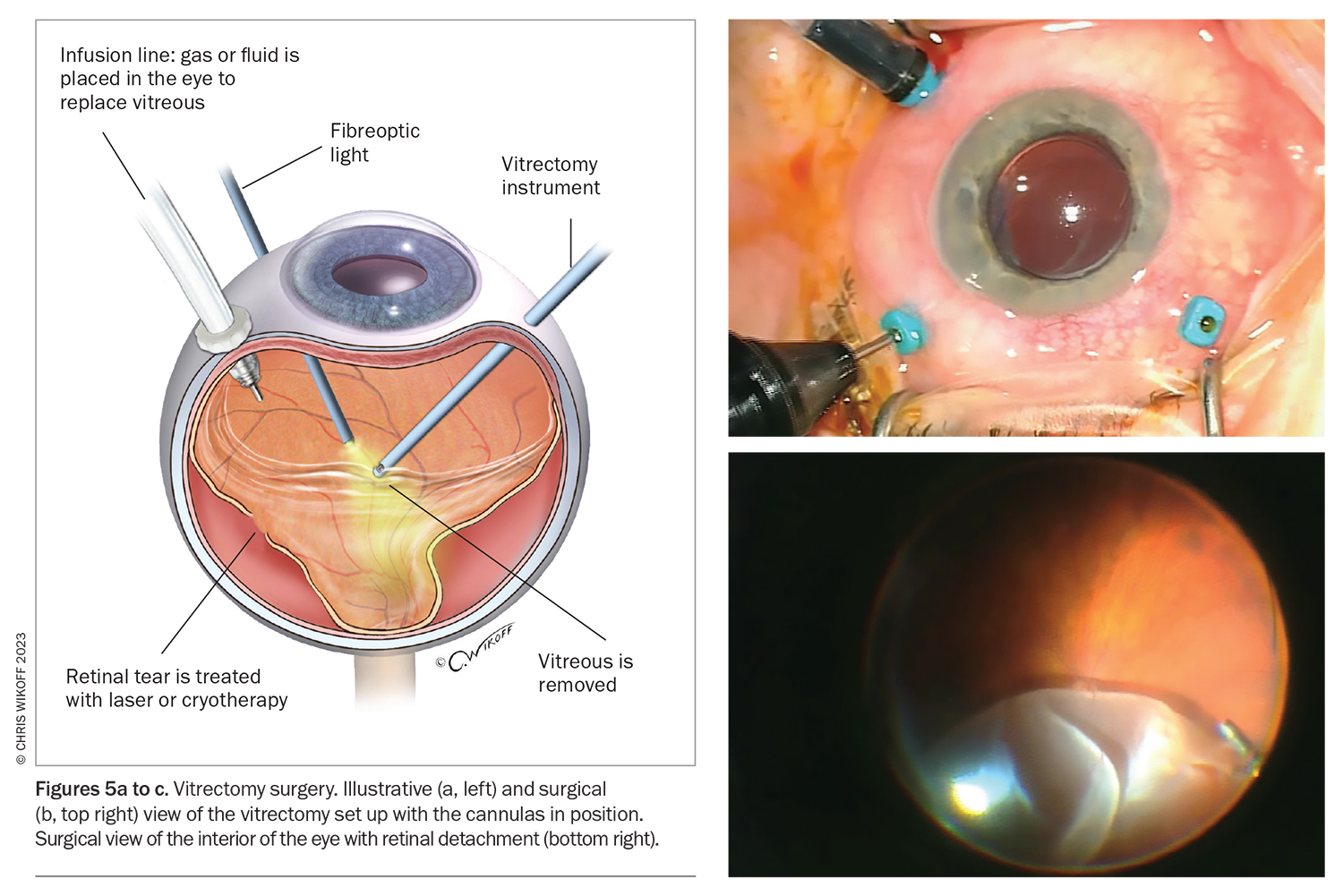
Vitrectomy surgery is a microsurgical keyhole surgical technique in which the retinal detachment is repaired internally with laser and cryotherapy (Figures 5a to c). Any vitreous gel pulling on the retina is removed and replaced with a gas bubble (Figure 3b). The gas bubble exerts a tamponading effect as it repositions the retina against the inner wall of the eye. By the time the retinal tear and detachment have healed, the gas bubble dissolves away and is replaced with aqueous/vitreous fluid produced by the eye.
{kind=link}
Generally, three different types of gas are used:
- air, which typically lasts four to seven days
- sulfur hexafluoride (SF6), a short-acting gas that typically lasts two weeks
- perfluoropropane (C3F8), a long-acting gas that typically lasts for four to eight weeks.
In cases of advanced retinal detachment, when long-term pressure on the retina is needed to keep the retina in position, other tamponading agents such as silicone oil or heavy liquid may be used. In such cases, a second procedure is required to remove the oil once the retinal position has stabilised.
Scleral buckle surgery
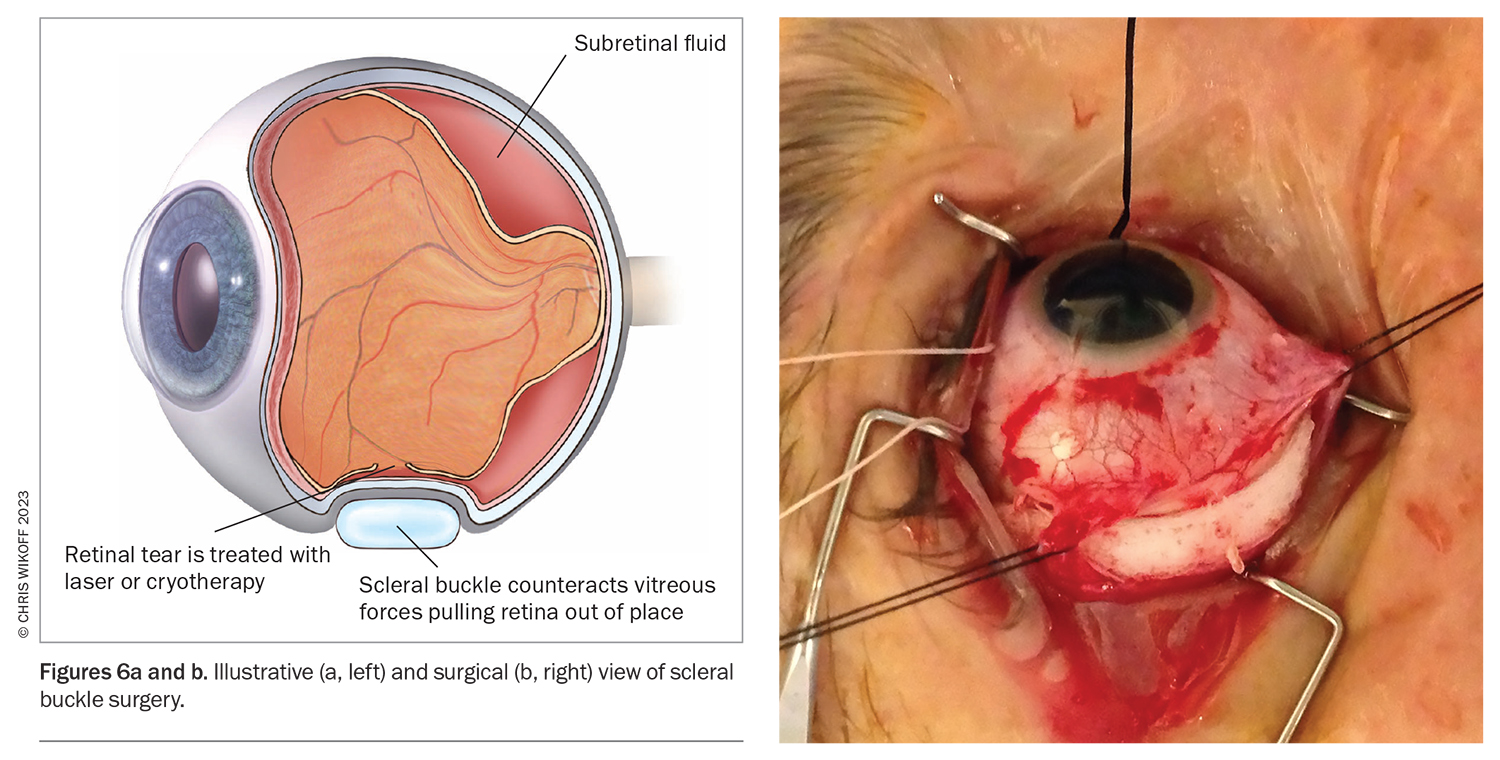
Scleral buckle surgery involves placement of a silicone band (the scleral buckle) around the outside wall of the eye to counteract the vitreous force pulling the retina internally and out of place (Figures 6a and b). Fluid that accumulates under the detached retina may need to be drained from the eye, which aids in repositioning the retina against the inside of the eye. A small gas bubble is then placed in the vitreous cavity to tamponade the retina.
{kind=link}
Postoperative care
Eye drops
Patients need to administer eye drops, typically antibiotic, corticosteroid and cycloplegic/dilating drops for several weeks after the surgery, in a tapering regime.
Gas tamponade agents
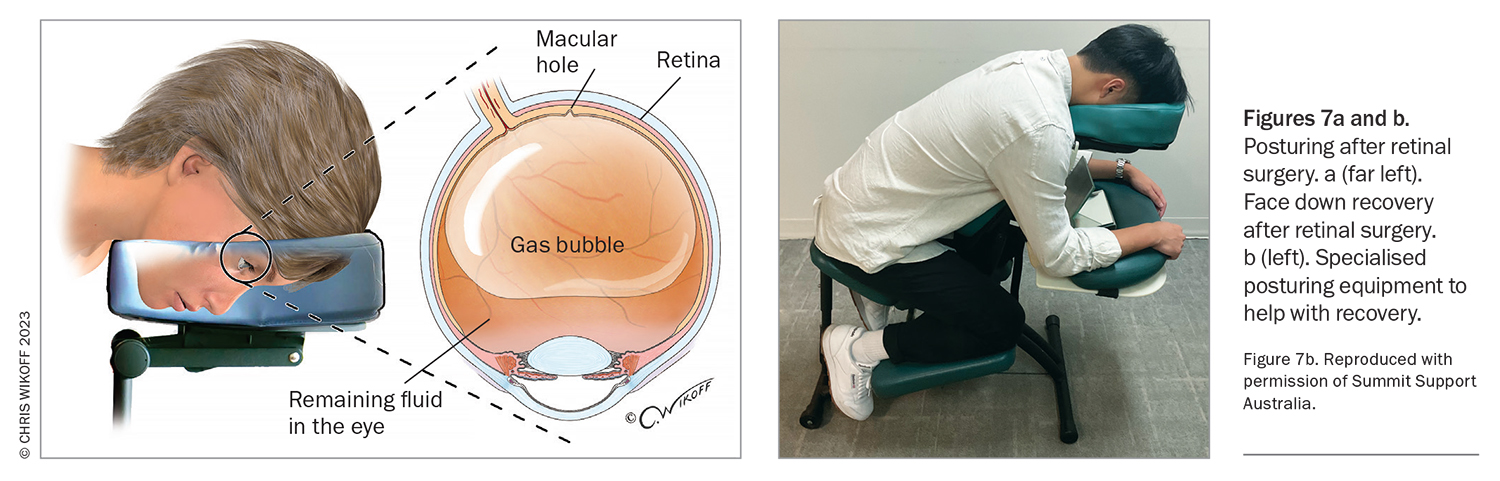
If a gas bubble was placed in the eye, the patient may be asked to maintain a particular head position for several days so that the gas places pressure on the area of retinal detachment (Figure 7a). The gas bubble is gradually replaced by aqueous/vitreous fluid and disappears over days to weeks. Patients routinely wear a wrist bracelet to warn medical staff against administering nitrous oxide while gas remains in the eye as it could cause the gas to expand. Patients with a gas bubble must not fly in a plane as the gas will expand with altitude.
{kind=link}
Posturing after retinal surgery
It is essential patients comply with posturing requirements after retinal surgery to allow adequate healing of the retina. Patients may be asked to position during the day and night, even in their sleep. Patients can hire a special chair to make this positioning more comfortable (Figure 7b)
Post vitrectomy cataract
Cataract formation can accelerate after vitrectomy surgery, typically within 24 months. Patients may complain of symptoms related to cataract, such as blurred vision and difficulty with night driving and reading. Patients are warned of this risk as part of the informed consent before undergoing retinal surgery.
Outcomes for vision
It may take many months for a patient’s vision to improve after treatment, depending on the extent of the initial retinal detachment. If the macula is involved, recovery of fine central vision is usually limited. Therefore, it is important to diagnose and treat retinal detachment before the macula is damaged. Timely surgery and modern techniques allow the repair of even complex retinal detachments with recovery of vision. A discussion with patients that includes explaining treatments and outcomes can alleviate symptoms of depression and anxiety, with a positive impact on quality of life.2
Conclusion
Public awareness of retinal detachment is limited, and it is thus important to raise awareness of this condition so that patients and their primary care clinicians seek immediate care when symptoms develop. Early referral and diagnosis are vital for optimal patient outcomes. Laser therapy can repair most retinal tears, whereas surgery is often required for retinal detachment. Postoperative care may include eyedrops, specific posturing and avoiding high or rapidly increasing altitude so as to not increase eye pressure. MT
COMPETING INTERESTS: Associate Professor Chang has received consultancy fees from Alcon, Apellis Bayer, Roche and Novartis; speaker fees from Alcon, Apellis Bayer and Roche; Travel support from Bayer and Roche; is the Secretary General Asia Pacific Vitreoretinal Society; and Chair of the Board, Sydney Eye Hospital Foundation. Dr Ham: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.