Corticosteroids and the eye

Corticosteroids are commonly used to treat many eye diseases but their inappropriate use can lead to vision loss. Systemic corticosteroids to treat nonocular diseases can also have ocular adverse effects. Important considerations before prescribing corticosteroids to treat eye conditions in general practice include taking a detailed history asking about risk factors and examination for any signs of infection.
Corticosteroids are often described as a double-edged sword. They are powerful drugs with many uses in medicine, especially in the treatment of inflammatory ailments such as allergic disorders, asthma, inflammatory bowel disease and eczema.1 They are also often used to treat ocular conditions. However, corticosteroid use in and around the eye requires careful clinical consideration, as ill-considered use may lead to irreversible vision loss. Further, systemic corticosteroids can cause significant ocular adverse effects.
This article explores the use of corticosteroids to treat eye diseases and common ocular side effects of local and systemic corticosteroids. It also discusses important considerations before prescribing corticosteroids to treat eye conditions in general practice.
Ocular indications for corticosteroid therapy
Among their many uses, corticosteroids are commonly used to treat ocular inflammatory diseases such as noninfectious uveitis and noninfective keratitis and ocular surface diseases such as atopic keratoconjunctivitis and cicatrising conjunctivitis. They are also used, in combination with appropriate antimicrobial cover, to dampen the inflammatory response during an infective process. Corticosteroids are also often used postoperatively, after most forms of intraocular surgery, including cataract surgery, and ophthalmic laser procedures such as selective laser trabeculoplasty.
Corticosteroids to treat eye conditions can be delivered either locally or systemically. Local delivery is preferable as it carries less risk of systemic side effects. Local delivery methods include topical application, periocular injection (subtenon, orbital floor, peribulbar or retrobulbar) and intravitreal injection.
Systemic delivery of corticosteroids may be considered for ocular diseases in certain situations. These include in patients with systemic diseases that require systemic corticosteroid treatment. In children, systemic corticosteroids and their adverse effects must be carefully considered against the risk of general anaesthesia required for periocular and intravitreal injections, particularly if multiple injections are needed.
Common ocular adverse effects of corticosteroids
The adverse effects of corticosteroids on the eye depend on the route of delivery, frequency of use and cumulative dose. Adverse effects can occur with local delivery to treat an ocular condition. Corticosteroids administered to treat nonophthalmological conditions, remote to the eye and orbit, may also have unintended effects on vision. These effects can occur with systemic delivery via the oral, intramuscular and intravenous routes and also with nasal, inhaled and dermatological delivery.
Cataract
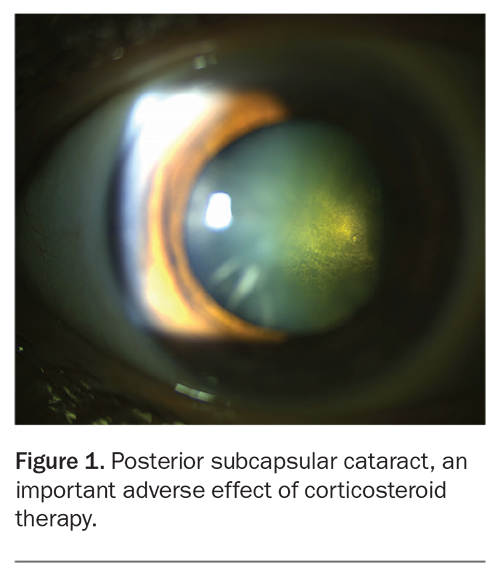
Posterior subcapsular cataract (PSC) is the most common type of cataract related to corticosteroid use. This type of cataract forms over the posterior cortex, just within the posterior capsule (Figure 1). PSC, although less common than nuclear sclerotic cataract (NSC), is often seen in patients with diabetes or long-term corticosteroid exposure. NSC is often seen with ageing.
{kind=link}
All forms of cataract can result in reduced visual acuity, field and quality. However, patients with PSC more often complain of glare and haloes along with reduced vision than patients with other types of cataract.
Glaucoma
Corticosteroids administered via any route can cause an increase in intraocular pressure. Patients who develop raised intraocular pressure secondary to corticosteroid use are often termed ‘steroid responders’. Typically the increase occurs three to six weeks after starting topical corticosteroid therapy but can occur earlier or later; the latter is more common with intravitreal injections.2 Raised intraocular pressure over a prolonged period can result in secondary open angle glaucoma which, if left untreated, can lead to irreversible blindness. Risk factors for being a steroid responder include a personal or family history of primary open-angle glaucoma, high myopia and diabetes mellitus. Children aged under 6 years and older patients are at greatest risk.3,4
Anecdotally, topical corticosteroid eye drops can be purchased over the counter in some countries for cosmetic treatment of red eyes caused by air pollution. Use of these drops is more common in younger people. Without appropriate monitoring, long-term use of these drops may lead to devastating consequences.
Systemic use of corticosteroids can result in both cataract and raised intraocular pressure, leading to glaucoma. Glaucoma and irreversible blindness have also been reported with corticosteroid use for eczema (not only when applied around the eye).1 Reliance on patients presenting with ocular symptoms alone is insufficient to detect conditions such as glaucoma, which can be asymptomatic in the early stages. Therefore, patients who are taking corticosteroids long term via any route should have their eyes checked regularly.
Central serous choroidal retinopathy
Central serous choroidal retinopathy (CSCR) is a retinopathy typically affecting men aged 20 to 50 years. Pregnant women in the third trimester are also at increased risk. CSCR is associated with both endogenous and exogenous corticosteroid use. It is more commonly associated with systemic than with topical ophthalmic corticosteroid use.5,6 Endogenous risk factors for CSCR include Cushing’s disease, Conn’s syndrome, type A personality and psychosocial stress factors.7
Immunosuppression
Corticosteroids can downregulate the immune system, leading to secondary infection or worsening of an existing ocular infection. Therefore, patients with a noninfective corneal ulcer should receive topical corticosteroids only if there is significant ocular inflammation and only after appropriate antimicrobial cover has been administered resulting in the ulcer showing marked improvement.
Systemic adverse effects of ocular corticosteroids
Topical corticosteroids can have systemic side effects. Cushing’s syndrome secondary to topical corticosteroid use has been reported in both adults and children.8-10 A rise in blood glucose level has been reported after topical corticosteroid use in people with diabetes, although there was no statistically significant change in patients without diabetes.11
Considerations before corticosteroid use
Route of administration
When choosing the route of administration of a corticosteroid to treat an eye condition, there are several factors to consider. The main criterion is to choose a route that minimises adverse effects.
Topical corticosteroids
Topical corticosteroids (eye drops and ointment) are most commonly used to treat anterior segment pathologies. Eye drops are simple to administer and stop if necessary. Systemic absorption can be reduced by occluding the nasal lacrimal drainage system with finger pressure for a few minutes after administering the drops or insertion of a punctal plug. However, adherence may be an issue with eye drops, along with ocular irritation from the active ingredients or preservatives. Preservative-free preparations can be compounded and used in special circumstances.
After the disease process has settled, the corticosteroid dose should be tapered over time. For example, if drops are applied four times daily, an option is to omit one daily dose every five days, until the drops are ceased. It is important to warn patients that if symptoms rebound, they should return for reassessment as soon as possible; if there are no signs of infection, the tapering regimen may need to be extended over a longer period. A good guide to determine whether a patient is ready to taper the dose is to ask what happens if they miss a dose; if there are no significant symptoms then they are ready to taper, otherwise it may be too soon.
Periocular corticosteroids
Periocular injection (subtenon, peribulbar or retrobulbar) allows corticosteroids to be deposited in the periocular region for a longer period. This may target posterior segment pathologies and reduce the risk of nonadherence, but has the disadvantage that the corticosteroid cannot be removed after administration. Periocular injections can be done under local anaesthesia in adults. However, general anaesthesia is usually required in children, and the risks associated with such anaesthesia need to be considered.
Intravitreal corticosteroids
Intravitreal corticosteroid injection allows direct targeting of the posterior segment over a period of time and eliminates the risk of nonadherence. However, this method has the risk of endophthalmitis and, after administration, the corticosteroid can be removed only via vitrectomy surgery.
Infection
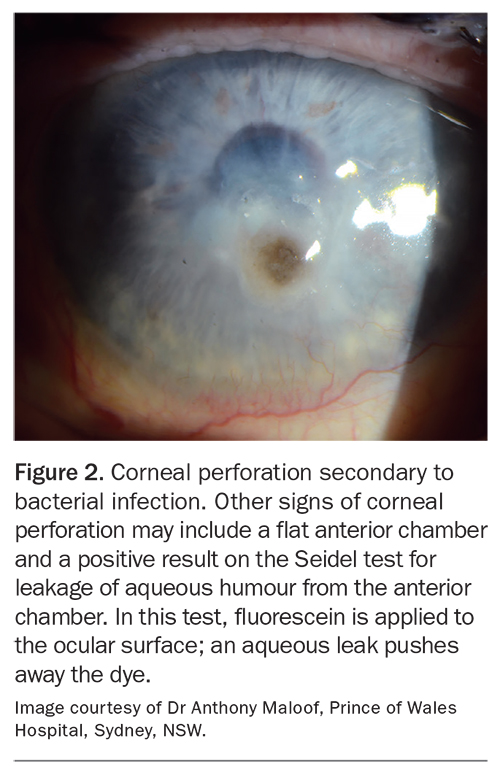
Before prescribing any topical, periocular or intravitreal corticosteroid therapy, it is imperative to determine whether there is any ocular infection. Inflammation secondary to autoimmune (allergic) causes, surgery or other procedures will often improve with corticosteroids. However, if a corticosteroid is administered to an infected eye without appropriate microbial cover (bacterial, viral, parasitic or fungal), it will exacerbate the infection and may lead to complications such as corneal perforation (Figure 2).
{kind=link}
A detailed ocular history is essential, (see below) along with an appropriate examination. Consider taking a corneal swab or scrape for microscopy, culture and sensitivity testing before starting any periocular corticosteroid. In the GP setting, if the practitioner is comfortable treating small infections (less than 1 mm diameter) then a swab is advisable before starting any treatment. In the ophthalmological setting, any suspected bacterial keratitis with an infiltrate more than 1 mm in diameter is usually sampled with a swab and scrape.
Risk factors and red flags for infective keratitis
GPs should consider several important points before prescribing topical corticosteroids for an eye condition. Most important is a detailed history asking for risk factors and examining for any signs of infection.
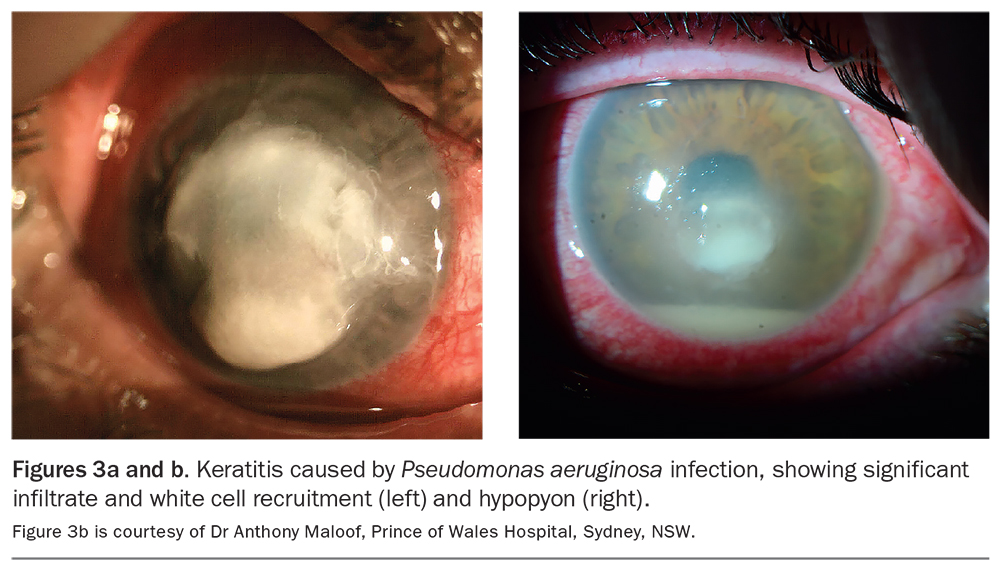
A history of contact lens wear is particularly important, as contact lens wearers are at higher risk of Pseudomonas aeruginosa infection. They need to be treated by an ophthalmologist with appropriate antibacterial cover, such as topical ofloxacin, instead of the usually prescribed chloramphenicol eye drops.12
Signs of P. aeruginosa infection may include corneal infiltrate with white cell recruitment (Figure 3a) and anterior chamber inflammation, which can result in a hypopyon (Figure 3b). Signs of infective keratitis typically include more central location of the lesion, anterior chamber inflammation, lesion size more than 1 mm and the presence of an infiltrate.
{kind=link}
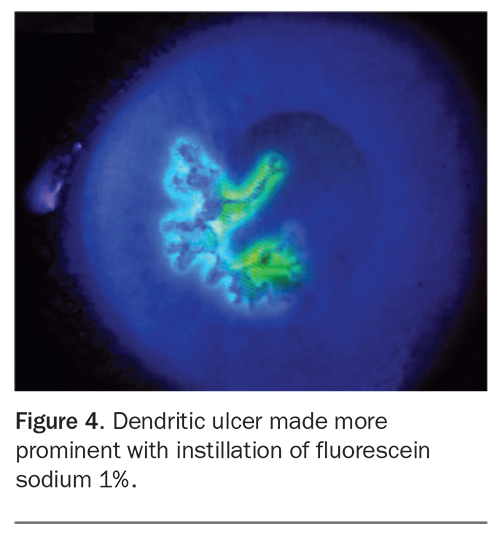
Risk factors for herpetic keratitis include previous cold sores, immunosuppression or previous confirmed herpetic keratitis. Herpetic keratitis produces characteristic dendritic ulcers, which are more readily seen after instilling fluorescein (Figure 4). The use of topical corticosteroids without appropriate antiviral cover, such as valaciclovir, can significantly worsen viral keratitis.
{kind=link}
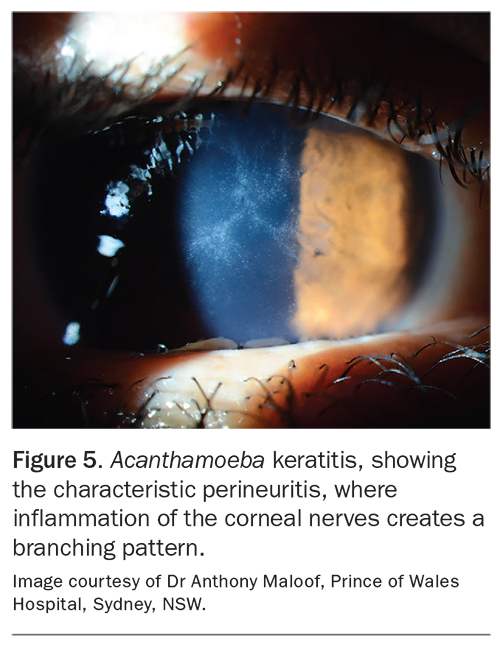
Risk factors for Acanthamoeba keratitis include extended contact lens wear, poor contact lens hygiene, such as rinsing under tap water, and swimming or using hot tubs while wearing contact lens. Perineuritis is characteristic of Acanthamoeba keratitis (Figure 5).
{kind=link}
Risk factors for fungal keratitis include immunosuppression (diabetes and corticosteroid use) and trauma from organic material such as gardening or animal-related injuries (Figure 6).
{kind=link}
Fungal and Acanthamoeba keratitis are important considerations because they are difficult to treat and require appropriate confirmation and topical treatments that are hard to access in general practice. Patients who are at risk of fungal or parasitic keratitis require early referral. Topical corticosteroids should be prescribed only after full assessment by a specialist ophthalmologist.
Corneal protective mechanisms
Patients with poor corneal protective mechanisms, such as reduced corneal sensation, a poor Bell’s reflex or lagophthalmos, are at higher risk of corneal infection and poor healing. They should be referred to an ophthalmologist as soon as possible.
As a general rule of thumb, if a patient has poor corneal protective mechanisms or significant risk factors for infective keratitis, prompt ophthalmological referral is warranted. In the case of an infective corneal ulcer or infiltrate then corticosteroids should not be started by a nonophthalmologist until the corneal ulcer has healed or shown significant improvement.
Children
Long-term corticosteroid use in children requires close monitoring of intraocular pressure and assessment for cataract formation. Adults with cataract who previously had good vision can have their vision restored with cataract surgery. However, in children, the eyes require constant stimulus to develop until the age of 7 to 9 years. If this stimulus is hindered by a cataract then amblyopia may develop, and vision may not return to normal even with cataract surgery.
Common topical ophthalmic corticosteroids
Common topical corticosteroids for ophthalmic use include:
- prednisolone (e.g. prednisolone acetate 1% and prednisolone sodium phosphate 0.5%)
- dexamethasone (e.g. dexamethasone 0.1%)
- progesterone-like agents (e.g. fluorometholone 0.1% and fluorometholone acetate 0.1%; the acetate form penetrates the ocular surface better than fluorometholone, resulting in more potent intraocular treatment)
- hydrocortisone (e.g. hydrocortisone suspension 0.5% and 1.0% eye drops and hydrocortisone acetate 0.5% and 1.0% eye ointment).
Topical corticosteroids are commonly formulated in liquid or ointment form, with ointments being much more viscous. Liquid eye drops may be available in multidose bottles or daily use minims. Minim preparations are typically considered preservative-free and are preferred if drops cause ocular irritation or need to be applied more often than four times daily, as preservative in excess is more likely to cause ocular irritation, inflammation and dry eyes. However, even minim preparations contain excipients to which allergy can develop.
Ointments are often preferred for evening application as they provide longer cover overnight. Further, although ointments provide some relief from pain and discomfort, they cause blurred vision, which is less of a problem with application at night. However, if an ointment is applied during the day, the patient must be warned of reduced vision and refrain from activities that require good vision such as driving and operating heavy machinery.
The efficacy of corticosteroid preparations depends not only on the active ingredient and frequency of administration but also on the degree of penetration into the ocular surface. Medications that are more lipophilic have greater corneal penetration, and therefore acetate preparations penetrate more than phosphate preparations.13 Preservatives also enhance penetration by disrupting the tight junctions between corneal epithelial cells.14 However, the greater the penetration, the higher the risk of raised intraocular pressure and cataract.
Alternatives to corticosteroids
Alternatives to corticosteroids for treatment of selected eye diseases include:
- calcineurin inhibitors (e.g. ciclosporin)
- the second-generation topical immunomodulator lifitegrast
- NSAIDS.
Ciclosporin 0.05% is commonly prescribed to treat keratoconjunctivitis sicca or dry eye syndrome, where inflammation is a hallmark.15 Ciclosporin suppresses ocular inflammation and increases tear production. Typically, it takes a few months for maximal effect and can cause stinging in the early phase of treatment. Ciclosporin is safe for long-term use, which is usually necessary in patients with moderate to severe dry eye syndrome.
Lifitegrast is TGA approved for the treatment of moderate to severe dry eye disease in adults when treatment with artificial tears has not been sufficient. Patients who require this treatment are best referred to an ophthalmologist.
NSAIDs, including ketorolac trometamol ophthalmic solution 0.5% and nepafenac ophthalmic suspension 0.3%, are often prescribed for the temporary relief of itchy eyes caused by seasonal allergies, inflamed pterygia and pinguecula. NSAIDs are also used in conjunction with topical corticosteroids for the treatment of cystoid macular oedema after ocular surgery. Ketorolac trometamol is applied twice daily, and nepafenac is applied once daily. Although topical NSAIDS do not cause cataracts or corticosteroid-induced glaucoma, they can have serious complications, including corneal melt (peripheral ulcerative keratitis) leading to perforation.16 Therefore, patients using ophthalmic NSAIDs should be reviewed regularly by a practitioner with ophthalmic expertise.
Conclusion
Corticosteroids are powerful and useful medications to treat ocular and other diseases. Like all such medications, their use must be carefully considered and their side effects need careful monitoring. The ocular consequences of systemic corticosteroids must be considered, and the patient monitored for these. If there is any doubt, early and prompt ophthalmological referral can be sight-saving. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.