Unboxing herpes zoster ophthalmicus and the recombinant shingles vaccine

Reactivation of the varicella zoster virus as herpes zoster (shingles) typically affects the peripheral nerves, resulting in a painful rash, most often on the torso. However, it can also manifest ophthalmologically, affecting the ophthalmic division of the trigeminal nerve. This manifestation is associated with a particularly high level of morbidity and may result in blindness. A new recombinant shingles herpes zoster vaccine protects patients against this virus and post-infection sequelae, improving medical and psychosocial outcomes.
- Varicella zoster virus reactivation in adulthood manifests as herpes zoster and is characterised by a painful vesicular rash in a unilateral dermatomal pattern in the distribution of a cranial nerve or dorsal root ganglion.
- Postherpetic neuralgia (PHN) is the most common long-term sequela of herpes zoster.
- Herpes zoster can involve the ophthalmic division of the trigeminal nerve, referred to as herpes zoster ophthalmicus (HZO), and can result in chronic pain, reduced quality of life and permanent vision loss.
- Early treatment of HZO rash with antiviral therapy reduces the incidence of ocular complications but is ineffective in reducing PHN.
- A new recombinant subunit vaccine, Shingrix, is now available in Australia for people aged 50 years and over and is highly efficacious in preventing herpes zoster and PHN.
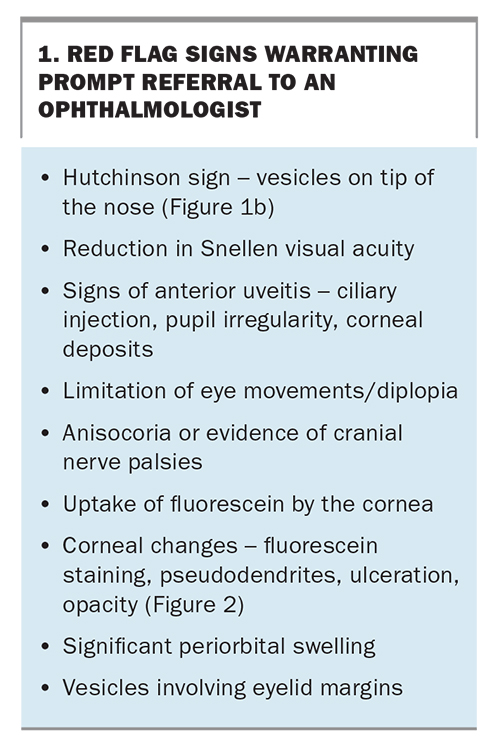
- Referral to an ophthalmologist is crucial if patients present with signs of HZO, including the presence of vesicles on the tip of the nose or signs of anterior uveitis.
With COVID-19 becoming the pre-eminent viral infection worldwide, it is important to keep in mind other common viral infections associated with high morbidity. Among these is herpes zoster, a condition with increasing prevalence, onset in younger patients and serious risk of long-term localised and systemic sequelae. Also known as shingles (‘zoster’ and ‘shingles’ both refer to its girdle-like distribution when it manifests in the thoracic and lumbar dermatomes), herpes zoster represents reactivation of latent varicella zoster virus (VZV). It presents with a characteristic painful vesicular rash in a unilateral dermatomal pattern in the distribution of a cranial nerve or dorsal root ganglion.
Compared with initial VZV infection (chicken pox), herpes zoster carries a much greater clinical burden.1 It not only has a debilitating acute presentation but is associated with chronic sequelae, most often postherpetic neuralgia (PHN), with long-term health consequences and reduced quality of life.2 Although cranial dermatomes are the second most commonly affected region in herpes zoster, after thoracic dermatomes, involvement of the ophthalmic division of the trigeminal nerve, or herpes zoster ophthalmicus (HZO), is arguably the most important because of the potential for serious early and late ocular disease and blindness.3
Herpes zoster vaccination is recommended for older people in Australia.4 A new nonlive recombinant herpes zoster vaccine, Shingrix, is now available for people aged 50 years and over. It is effective in preventing herpes zoster and PHN and in reducing the severity of acute and chronic VZV-associated pain.5
Incidence of herpes zoster
The incidence of herpes zoster has been increasing worldwide.6 In Australia, about 120,000 cases of herpes zoster are recorded annually, accounting for one in 1000 GP visits, with 10 to 25% of cases presenting as HZO.6,7
One in two people will develop shingles by the age of 85 years, with the risk increasing with age. However, a large study conducted in 2011 found a mean age of 52 years at presentation, which is younger than found in previous studies. This trend towards younger age of onset is thought to be related to the introduction and effectiveness of a shingles vaccination program for people aged over 65 years.8 Another theory is based on an epidemiological model that suggests this trend could be attributed to the varicella vaccine and subsequent reduced opportunities for subclinical boosting of VZV immunity.8
A possible association between statin use and herpes zoster has been raised, and the incidence of undiagnosed diabetes is higher in patients with herpes zoster.9,10
Herpes zoster ophthalmicus
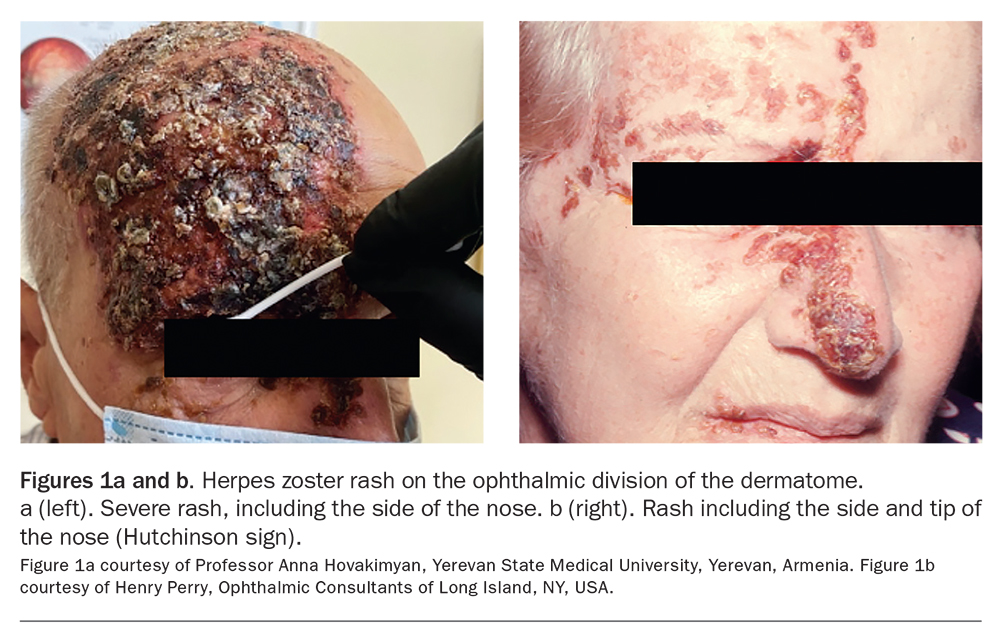
HZO afflicts the ophthalmic branch of the trigeminal nerve after reactivation of latent VZV in the dorsal root ganglia. Reactivation is related to a reduction in T cell-mediated immunity due to increasing age, immunosuppressive therapies or disease. HZO typically presents with pain, followed by a painful blistering rash, in the dermatomal distribution extending from the vertex of the skull to the nose, without crossing the vertical midline (Figures 1a and b).
{kind=link}
A period of dermatomal pain, headache and fever preceding the eruption of the characteristic rash is common. The rash has an erythematous base with clustered vesicles, which evolve over a period of five to seven days from fluid-filled blisters to pustules, which then burst and form a crust. Atypical and unusual presentations can occur, especially in immunocompromised people, which may delay diagnosis. It is important to note that the vesicular rash is contagious until the blisters burst and form a crust.1
In the acute phase, the pain is categorised as neuropathic, and patients commonly experience burning, tingling or stabbing pain. The neuropathic symptoms, including hyperaesthesia, allodynia (pain elicited by a stimulus that does not normally provoke pain) or paraesthesia, may persist for weeks to months after the acute phase. During the acute phase of herpes zoster, over 75% of patients report significant pain, with substantial proportions also having significant reductions in mobility and ability to undertake usual activities and basic self-care.11
As the incidence of herpes zoster has increased over recent years, so has the rate of HZO and its ocular complications.6 Hutchinson’s advice from 1865 that ‘it is well to warn a patient with herpes that very likely the eye may inflame, and that, if it does, serious mischief to the organ may result’ still holds true.12 HZO has the potential to result in chronic pain, reduced quality of life and permanent vision loss.
Ocular involvement
HZO can be associated with serious ophthalmic sequelae, including both anterior and posterior segment disease. About half of patients with HZO will experience ocular involvement if not treated with antiviral therapy.13 A retrospective cohort study in 2017 highlighted that one in 10 individuals may develop immediate or delayed moderate or severe vision loss secondary to HZO.14
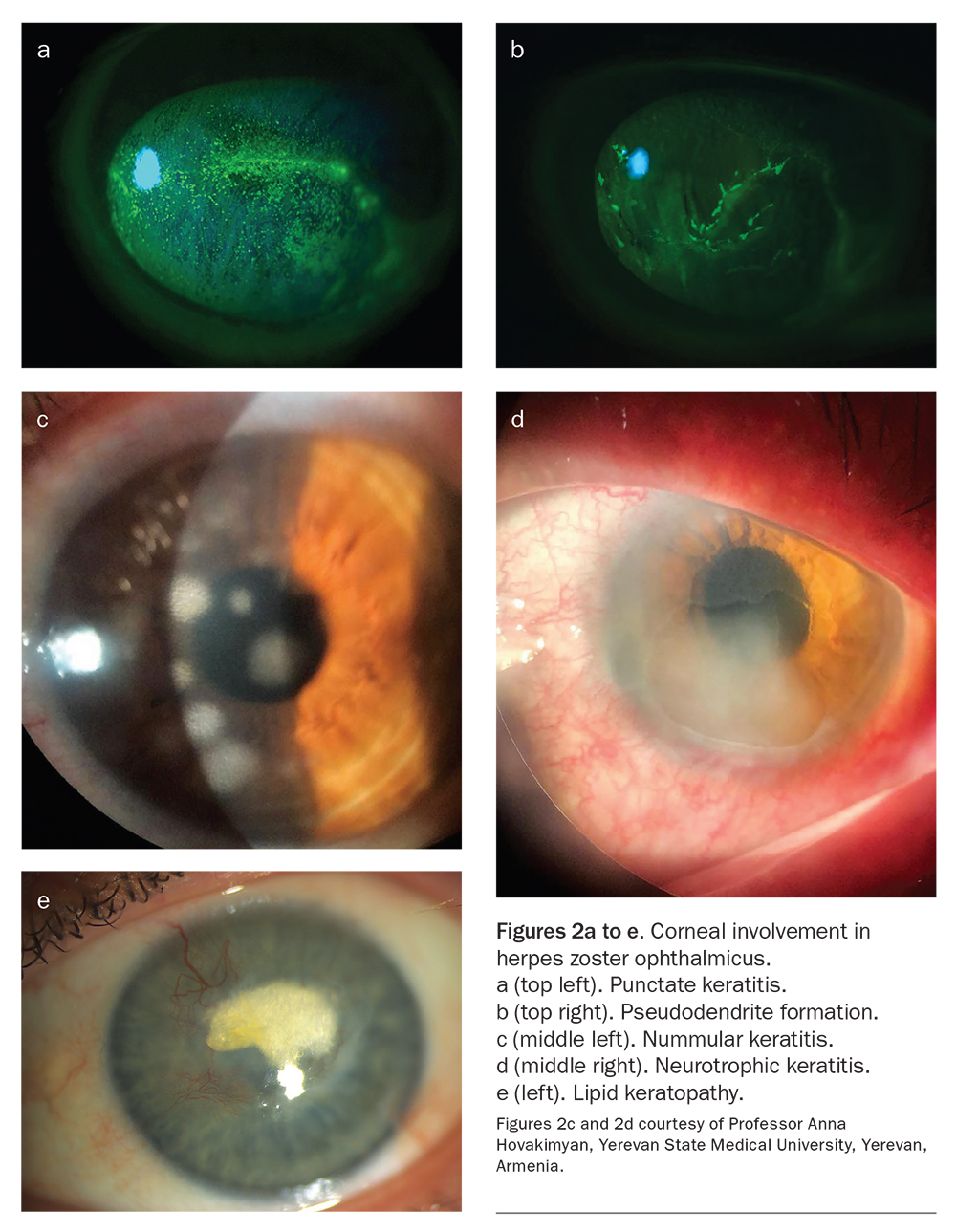
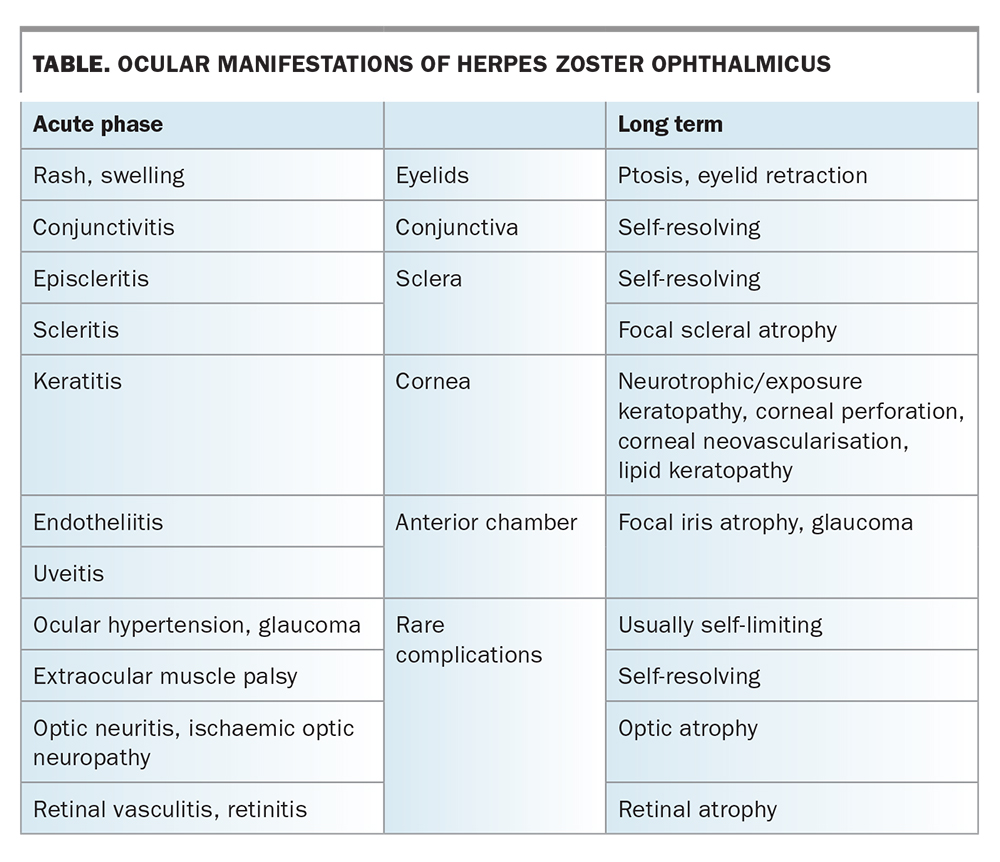
The most common forms of ocular involvement are keratoconjunctivitis, keratitis (Figures 2a, c and d) and uveitis, as outlined in the Table. Patients can lose vision through corneal scarring, lipid keratopathy (Figure 2e), corneal perforation or secondary glaucoma, as well as retinal or optic nerve involvement. As an integral outpost of the central nervous system, the eye can manifest consequences of central nervous system zoster, such as multiple cranial nerve palsies, orbital apex syndrome, papilloedema (as a consequence of VZV-associated meningitis or encephalitis) and stroke.
{kind=link}
{kind=link}
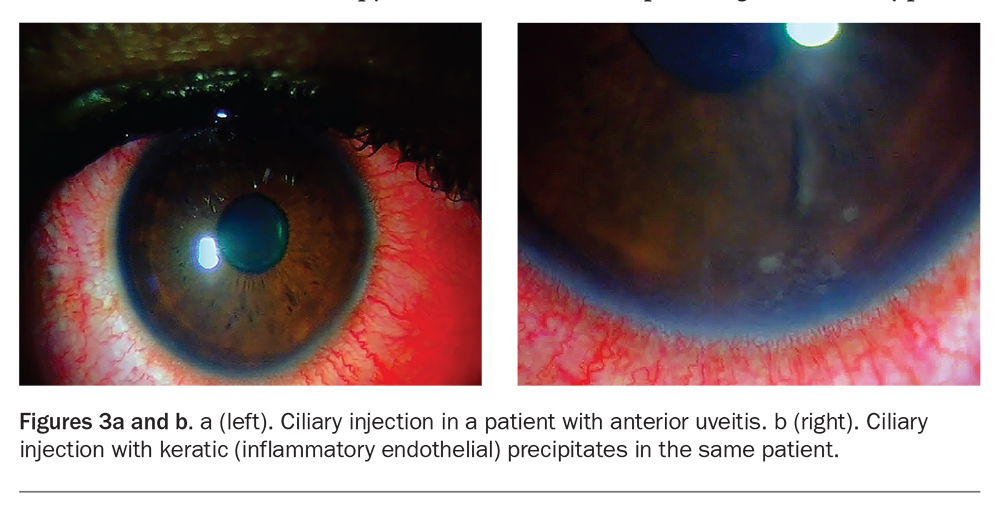
Referral to an ophthalmologist within the first week of symptom onset is therefore crucial to recognise some of these complications. Ocular involvement is very likely if there is vesicle development on the tip or side of the nose (Hutchinson sign; Figure 1b).12 An early sign of ocular involvement is ciliary injection (Figures 3a and b), which is indicative of uveitis and warrants urgent referral. However, about a third of patients without nasociliary nerve involvement may also develop ocular complications.15
{kind=link}
GPs should promptly refer a patient to an ophthalmologist if any ‘red flag’ signs (Box 1) are seen in conjunction with the characteristic herpes zoster rash in the ophthalmic division of the dermatome.
{kind=link}
Systemic sequelae
Postherpetic neuralgia
PHN, the most common sequela of herpes zoster, is a chronic radicular pain that occurs in 10 to 20% of patients with herpes zoster and can last for months or years after the infection. It is defined as significant pain that persists for more than 90 days after the onset of the rash. It occurs in about 30% of patients with HZO with ocular involvement.16,17 PHN has a large socioeconomic and individual health burden, with varied effectiveness of treatments. A Cochrane review found there is insufficient evidence to conclude that antiviral therapy reduces the incidence of PHN. Therefore, preventing shingles through vaccination is crucial for reducing PHN-related morbidity in the community.18
Other systemic sequelae
Herpes zoster, particularly HZO, is a risk factor for stroke. A 2016 study found that, compared with control subjects, patients with HZO had a 4.5-times higher risk of stroke within one year of diagnosis. The mechanism is uncertain but is likely due to the zoster virus involving afferent sensory fibres of the trigeminal nerve and its proximity to the internal carotid artery plexus and its intracranial branches.19 Associations with temporal arteritis, myocardial infarction and depression have also been described. Another systemic association not to be ignored is a link between zoster and malignancy, seen in population-based studies.19
Investigations, diagnosis and management
Diagnosis of HZO is largely clinical; however, the diagnosis can be confirmed by sending samples of the fluid-filled vesicles for nucleic acid testing, such as polymerase chain reaction analysis. All patients with suspected HZO should be promptly started on an oral course of valaciclovir 1g three times daily or famiciclovir 500 mg three times daily for seven to 10 days. Renal and liver function should be monitored before starting and while using the medication.
The ophthalmologist and GP should work in conjunction to deliver expedient treatment to the patient. It has been shown that initiating treatment early, within the first 72 hours of HZO rash onset, has the best results for reducing the acute complication of pain, development of ocular complications and duration of the rash.20 Initiating early treatment with oral antiviral therapy has also been shown to reduce the incidence of ocular complications from as high as 65% to about 35%. However, as noted, systematic reviews do not show a reduction in incidence of PHN with antiviral therapy.18,21 Treatment of PHN involves topical therapy, including lignocaine or capsaicin, along with oral therapy with pregabalin, gabapentin or tricyclic antidepressants (off-label).
Ocular involvement must be treated by an ophthalmologist, as treatment varies depending on the type of complication. The most common signs of ocular involvement are outlined in the Table. For example, some cases of keratitis and uveitis, which present as a red, painful eye, require a prolonged course of topical corticosteroids to suppress the immune response. As topical corticosteroids have significant side effects, such as raised intraocular pressure, heightened risk of secondary infection and cataract formation, treatment must be initiated and monitored by an ophthalmologist. Evidence is lacking for the use of topical creams, such as aciclovir ointment, in patients with HZO, and the authors avoid this as it can cause ocular surface toxicity, which may affect epithelial healing and potentially lead to corneal ulceration.22
The use of systemic corticosteroids has been suggested as an adjuvant to antiviral therapy in patients with herpes zoster. A Cochrane review concluded that corticosteroids given during acute herpes zoster are ineffective in preventing PHN and could potentiate secondary bacterial skin infections. However, systemic corticosteroids are used by some clinicians, despite a lack of evidence regarding their efficacy in preventing HZO complications, specifically vasculitis and stroke.23 A patient’s comorbidities and age must by factored into the clinical decision regarding their use.
HZO in young people
Herpes zoster is less common in young people (aged under 50 years), although its incidence appears to be increasing.24 When a young person presents with HZO, it is the role of the treating doctor to investigate any underlying immunosuppression that may have triggered VZV reactivation, especially if the patient has had more than one episode of herpes zoster. GPs and ophthalmologists should work in conjunction to ensure there is no underlying systemic disease, and baseline blood samples and a thorough history should be taken at the time of diagnosis.
The trend towards increasing incidence of herpes zoster in young people highlights the importance of increasing awareness of the condition among primary care practitioners, including its presentation in younger patients and its sequelae. It is important to include herpes zoster as a differential diagnosis for all patients who present with unilateral moderate to severe craniofacial pain, with or without a rash.
COVID-19 and herpes zoster
Evidence suggests an association between SARS-CoV-2 and herpes zoster. A 2021 study showed that the prevalence of VZV in patients hospitalised with COVID-19 was three times that in the general population of hospital patients. This association is thought to be due to the immunosuppressive state associated with COVID-19, although its exact nature and significance are yet to be established.25
An increased prevalence of herpes zoster has also been observed after administration of COVID-19 vaccine. A Spanish study showed that VZV and herpes simplex virus reactivations accounted for 13.8% of cutaneous reactions after vaccination, mostly (17.2%) after administration of the Pfizer-BioNTech vaccine.26 Herpes zoster is most likely to occur within the first 21 days after vaccination.27
Zoster Eye Disease Study
Early research suggested that the use of long-term suppressive oral antiviral therapy may reduce complications of herpes zoster. Research regarding the best management approach to ocular manifestations of HZO remains ongoing. The Zoster Eye Disease Study, currently in the recruitment phase, is a multicentre, randomised, placebo-controlled clinical trial to study the use of long-term suppressive valaciclovir. It aims to determine whether there is a reduction in HZO complications, specifically ocular manifestations of keratitis and iritis, and to assess valaciclovir’s efficacy for treating PHN, at multiple time points up to 18 months.28
Shingrix vaccine: a major advance in prevention
Herpes zoster occurs with greater frequency and severity with increasing age and is often associated with PHN, which may interfere with function and quality of life during the acute and chronic phases. As antiviral therapy has a limited effect on the frequency and severity of PHN, a safe and effective vaccine to prevent herpes zoster in older adults, who are at greatest risk, is highly desirable.29 Vaccination remains the only way to reduce the risk of developing herpes zoster and its sequelae.
A live attenuated herpes zoster vaccine, Zostavax, has been available in Australia for over a decade. The new shingles vaccine, Shingrix, which appears to be more effective than Zostavax, is now approved in Australia and available to individuals aged 50 years or older to prevent herpes zoster and PHN.30,31 The vaccine is a nonlive recombinant zoster subunit vaccine of recombinant glycoprotein E. Two vaccine doses are administered at an interval of two to six months. Shingrix provides strong protection against developing shingles and PHN. The efficacy of the Shingrix vaccine was shown in a randomised, placebo-controlled trial across 18 countries, with a total of 15,411 participants aged 50 years or older. Compared with placebo, the study showed an overall efficacy against reactivation of VZV of 97.2%. Efficacy was maintained for four years after vaccination.32
The Shingrix vaccine can be given to adults who have previously received the live herpes zoster vaccine (Zostavax). The vaccine should not be administered to patients with a history of severe allergic reaction to any component of the vaccine, those who have active VZV infection or women who are pregnant or breast-feeding. The subunit vaccine can potentially be used for immunocompromised patients; however, clinical trial evidence in this population remains limited. The adjuvanted influenza vaccine, Fluad Quad, should not be coadministered with the Shingrix vaccine, as the safety of this combination has not yet been studied.4
A systematic review found that injection site reactions were more than five times as likely in vaccine than placebo recipients (relative risk, 5.63), and systemic adverse events more than twice as likely (relative risk, 2.28).33 In a clinical trial with participants aged 70 years or older, grade 3 injection site reactions occurred in 8.5% of vaccine recipients and grade 3 systemic reactions in 6%.34 Systemic reactions included headaches, myalgia and fever.
There have been reports of patients developing flares of herpes zoster after vaccination, with both the live and new subunit vaccines.35,36 Therefore, patients with a history of HZO or herpes zoster eye disease should be closely monitored for four to six weeks after vaccination.37
Conclusion
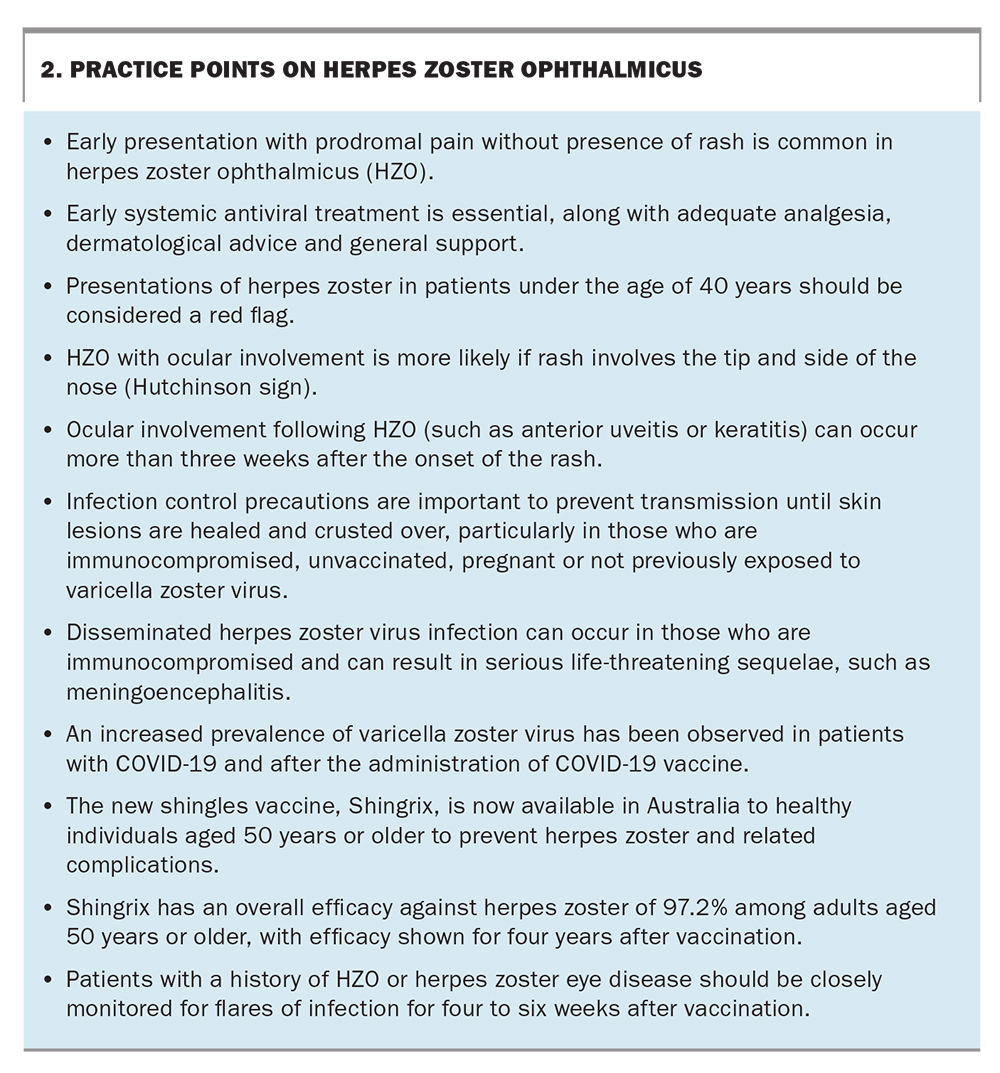
Herpes zoster is a common, disabling disease in the older population, with a trend to increasing prevalence in younger people. Although antiviral therapy is important to reduce the severity and duration of acute disease, it is not effective in reducing PHN. The recommendation for and administration of zoster vaccine is an important strategy to protect patients from herpes zoster and its complications, including PHN and ocular complications, as well as to improve their medical and psychosocial outcomes. GPs play a key role in ensuring high rates of vaccination, providing patient education and referring patients with ophthalmic complications to cotreating ophthalmologists. Practice points on HZO are shown in Box 2. MT
{kind=link}