Risk factor management in atrial fibrillation. A key pillar of care

The role of intensive cardiovascular risk factor management is being increasingly recognised in atrial fibrillation guidelines. GPs play a critical role in supporting patients to optimise their cardiovascular risk factor profiles to reduce the rapidly growing burden of this condition.
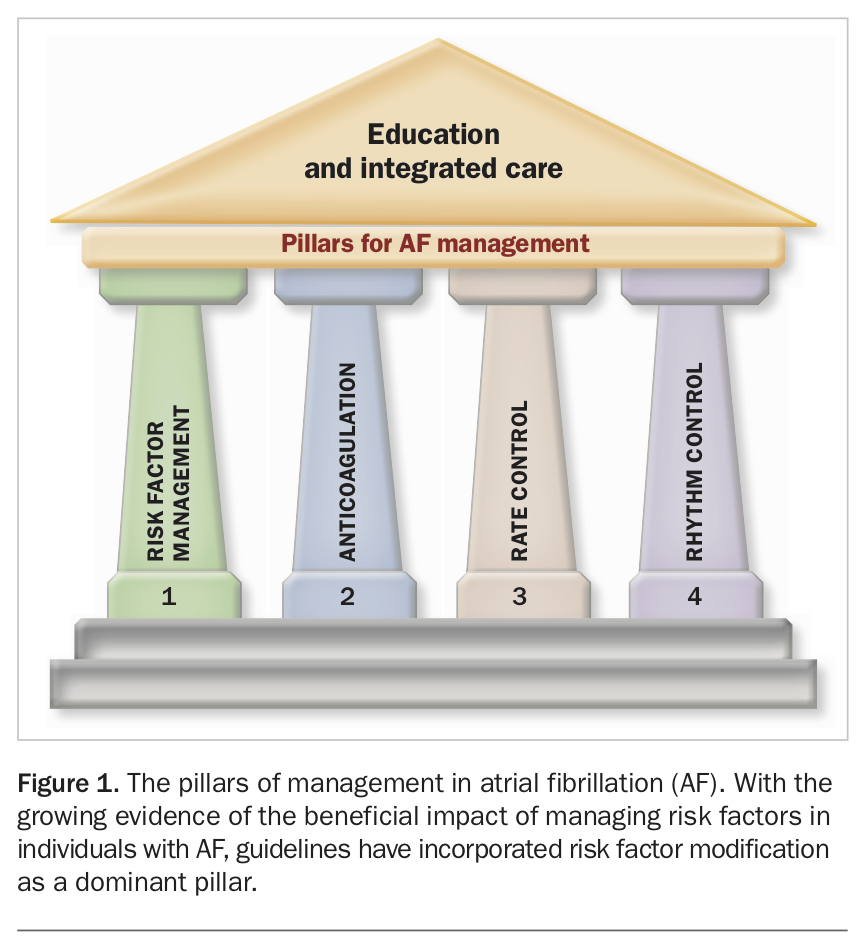
- Crucial pillars of care for atrial fibrillation (AF) include risk factor modification, anticoagulation, rate control and rhythm control.
- Randomised controlled trials and cohort studies show the benefit of risk factor modification in patients with AF, irrespective of treatment strategy, to reduce recurrence and burden of AF.
- Key modifiable risk factors include a high body mass index, physical inactivity, alcohol use, tobacco use, hypertension, dyslipidaemia and obstructive sleep apnoea.
- Risk factor modification for patients with AF is most effective when carried out in a structured clinic with multidisciplinary involvement and should be carefully tailored to the individual patient.
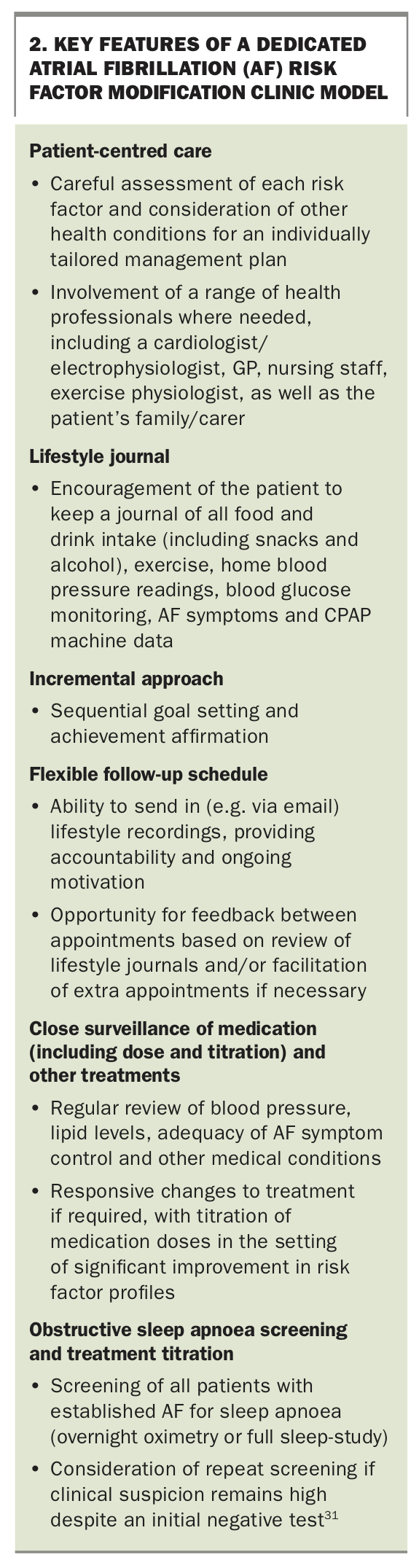
- Risk factor modification should encompass patient-centred care, lifestyle journals, stepwise goal setting, flexible follow-up schedules, close surveillance of medications and other treatments, and comprehensive management of all modifiable risk factors.
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia encountered clinically and is associated with increased rates of all-cause mortality, stroke, heart failure and healthcare resource utilisation. Globally, the incidence and prevalence of AF are rising, with recent Australian data demonstrating that hospitalisations for AF now outnumber both heart failure and myocardial infarction.1-3
Risk factor modification has been introduced as an essential component of AF care as there is now a significant body of evidence demonstrating that this reduces AF burden and progression, with or without additive catheter ablation (Figure 1).4-6
{kind=link}
Importantly, evidence suggests that targeting risk factors may reverse the AF process and potentially reduce complications.6,7 Given that risk factor modification provides such clear benefit to individuals with AF, it should be instigated, advocated for and managed by all healthcare professionals, and GPs are especially well placed to do this.
Modifiable risk factors associated with AF
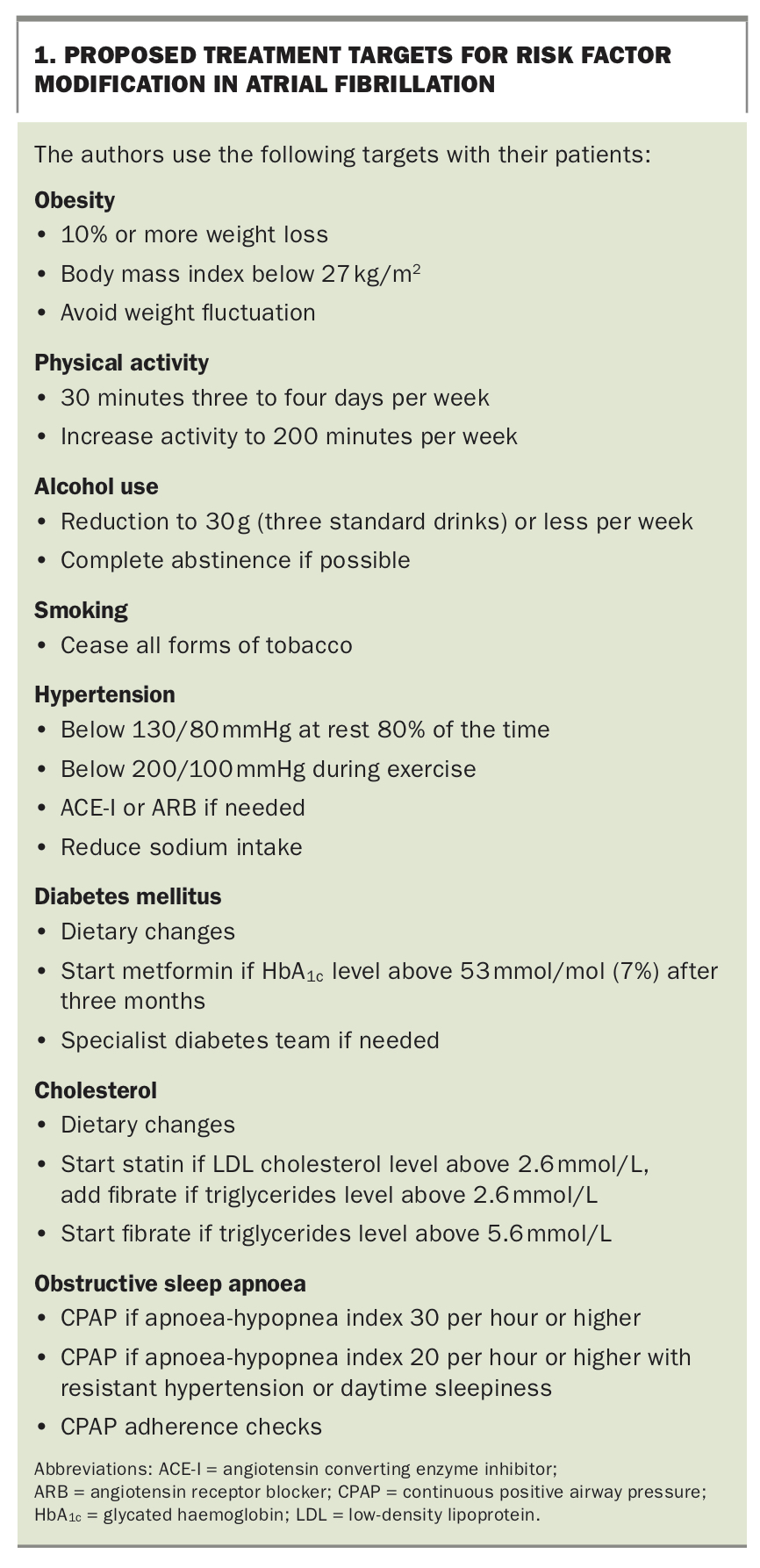
Changes in left atrial structure and function through the haemodynamic, electrophysiological and metabolic effects of underlying risk factors are thought to be responsible for the increasing incidence and prevalence of AF. Suboptimal management of these risk factors can increase AF burden and progression, and impact on complications related to AF. This article presents specific details on each modifiable risk factor and their respective treatment targets (Box 1).
{kind=link}
Obesity
A high body mass index (BMI) is a growing contributor to the risk of developing AF in our community. The risk of developing AF increases up to 29% with each five-point increase in BMI.8 An increased BMI has been associated with an increased left atrial size, pressure and blood volume, increased central blood volume and systemic vascular resistance, increased epicardial and pericardial fat deposition, conduction slowing and other electrophysiological adverse changes in human and animal studies.9-12
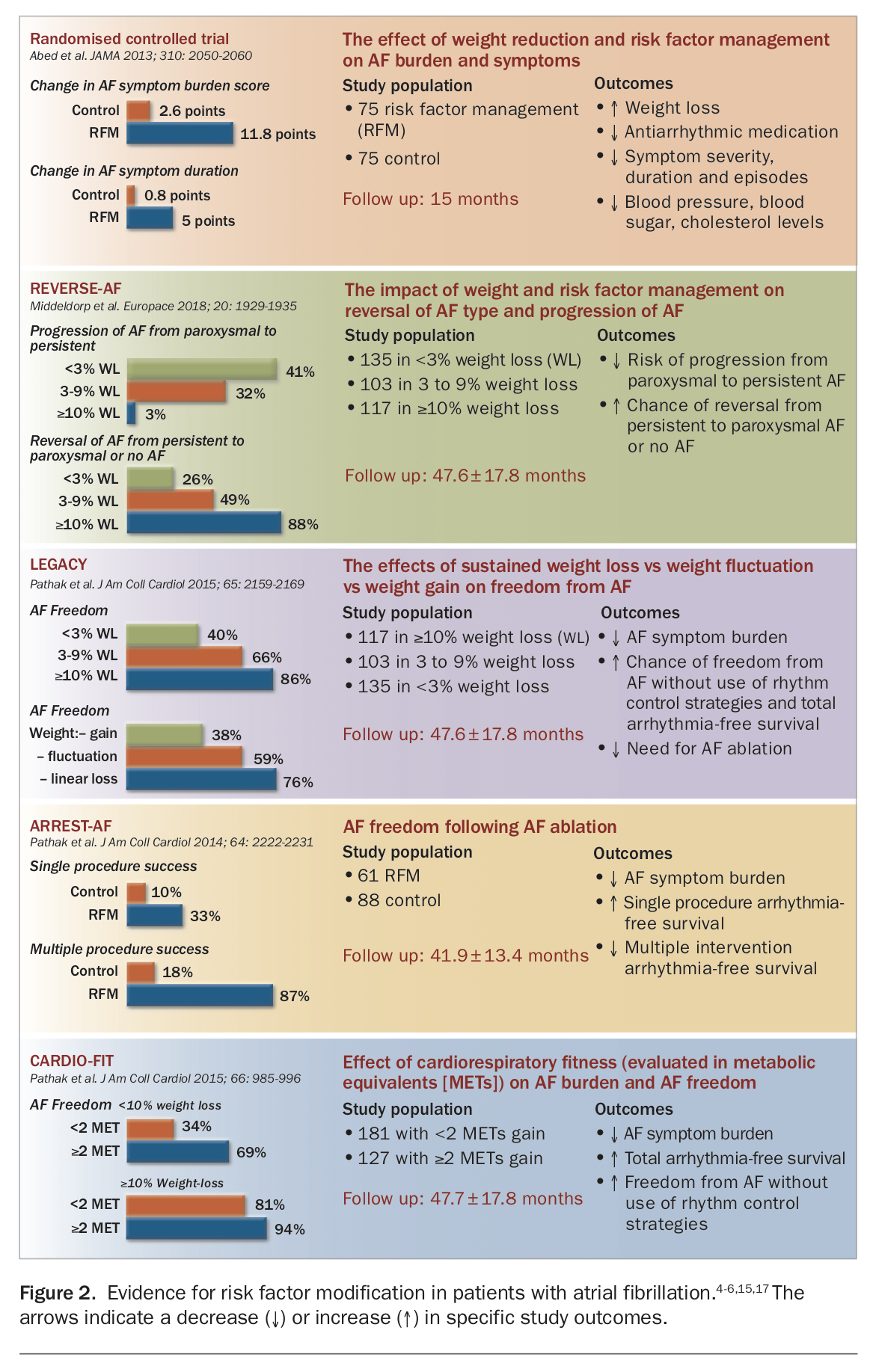
Sustained weight loss has dramatically reduced AF recurrence when it is achieved as part of a co-ordinated comprehensive risk factor modification approach, as demonstrated in the LEGACY and ARREST-AF studies, in patients pre- and post-catheter ablation.4,5 Weight loss was advised for all participants with BMI of 27 kg/m2 or higher in a physician-led dedicated clinic, separate to medical care. Individualised advice to modify current dietary habits was delivered via frequent reviews and feedback to maintain engagement. In LEGACY, 10% weight loss resulted in about a 50% reduction in AF burden, with incrementally reduced benefit in those achieving smaller degrees of weight loss.
Physical inactivity
Increasing evidence links sedentary lifestyle with a higher risk of developing AF, as well as poorer cardiovascular health and development of obesity.13 Light to moderate physical activity can reduce the risk of AF development by up to 28%.
Improved cardiorespiratory fitness has been found to have an additive effect to weight loss in reducing AF burden, as demonstrated in the CARDIO-FIT study.14,15 Moderate, rather than extreme, exercise levels should be advised because of a U-shaped relation between exercise and outcomes.13,16 Recommended targets for exercise are similar to those in general cardiovascular disease prevention guidelines: commencing with 30 minutes, three to four times per week, increasing to 200 minutes of at least moderate intensity exercise per week.4-6,17
Hypertension
In the Framingham Heart Study, hypertension was associated with a 40 to 50% increased likelihood of developing AF.18 Analysis of a large cohort of nearly 300,000 patients with prevalent AF identified that a blood pressure above 130/80 mmHg was associated with significantly higher risk of major adverse cardiovascular events.19
Hypertension causes an increased afterload, which leads to left ventricular hypertrophy and stiffening, reducing diastolic filling, and increasing left atrial volumes. The resultant left atrial dilatation leads to adverse electrophysiological changes and circulating hormones such as angiotensin II, further perpetuating these adverse changes and fibrosis.20-22
Treatment of hypertension to a target systolic blood pressure of 130 mmHg or lower has been found to reduce AF incidence roughly equal in magnitude to the increased risk attributed to this risk factor in the Framingham Heart Study.23 The recommended target for blood pressure management with AF is therefore below 130/80 mmHg at least 80% of the time.4-6,17 Treating to a lower blood pressure target may be associated with increased adverse events so is not recommended.24
Additionally, a hypertensive response to exercise (peak exercise systolic blood pressure of more than 210 mmHg in men or more than 190 mmHg in women) can indicate potential benefit for intensifying anti-hypertensive treatment. Such aggressive management of blood pressure needs to be tailored to the individual, monitoring for symptoms of postural hypotension and for changes in renal function. Resolution of left ventricular hypertrophy is also a surrogate indicator for adequate management of blood pressure.
Obstructive sleep apnoea
The presence of obstructive sleep apnoea (OSA) has been shown to double the risk of developing AF.25 Recurrent pharyngeal collapse with repetitive interruption of ventilation leads to hypoxaemia-associated atrial electrophysiological changes and significant haemodynamic changes that increase LA pressures, with resultant atrial enlargement. Chronic OSA is also linked to inflammatory and prothrombotic systemic changes.26-28 Treated OSA has been associated with reduction of AF recurrence risk after cardioversion or catheter ablation to a similar level as in patients without OSA.29
Screening for OSA is usually symptom-based; however, significant data demonstrates that OSA symptoms do not correlate with disease severity in symptomatic AF patients, with individuals with AF often showing no symptoms of OSA despite having the condition.30 Emerging evidence from implanted cardiac devices that highlight the night-to-night variability in the severity of sleep-disordered breathing further complicates this. Therefore, an individual with a high index of suspicion warrants repeated testing even in the setting of an initial negative screening or testing for OSA.30,31
It has been our practice to screen all patients for OSA if a rhythm control strategy is pursued, or in the setting of significant AF burden or resistant hypertension. Treatment of sleep apnoea should be initiated in conjunction with a sleep physician. Continuous positive airway pressure (CPAP) should be prescribed if the apnoea-hypopnoea index is greater than 30 per hour (or greater than 20 per hour with resistant hypertension or daytime sleepiness), and mandibular advancement splints and/or sleep positional devices should be considered if CPAP is not tolerated.
Diabetes mellitus
Diabetes mellitus has been found to independently increase the risk of AF by over one-third.32
In the prevalent AF population, the presence of diabetes has been associated with an increased risk of thromboembolism and stroke; poorer diabetic control has been associated with an increased risk of stroke and systemic embolism, and higher recurrence rates of AF in patients undergoing catheter ablation.33-35
Improved treatment of diabetes is an established component of the risk factor modification model leading to reduction in AF, although there is little to no data on treating this risk factor in isolation. The glycaemic target should be the same as that in standard diabetes care, aiming for a glycated haemoglobin (HbA1c) level of below 53 mmol/mol (7%). This target can vary, however, with duration of the condition and progression to insulin requirement, prevalence of hypoglycaemic episodes, number of comorbidities and functional capacity. Generally, if the HbA1c level is over 53 mmol/mol (7%), metformin should be prescribed, with or without other oral hypoglycaemics as needed. Involvement of a specialist diabetes team is strongly recommended.
Alcohol consumption
Alcohol consumption has been recognised as an important trigger for the development of AF. In its earliest form, the ‘holiday heart syndrome’ was described after binge drinking episodes.36 Increasingly, it is also recognised that chronic use of alcohol results in progressive injury to the atrial myocardium that promotes the progression of AF. Chronic alcohol consumption is linked with hypertension, obesity and OSA. A recent study using UK Biobank data reported that while fewer than seven standard drinks per week may protect against developing AF, there may be significant variations based on the type of beverage consumed, with even low-level consumption of beer and cider associated with a higher risk of AF than with wine or spirits.37
Practitioners should consider recommending alcohol abstinence for secondary prevention of AF. A recent randomised controlled trial found that abstinence advice led to an 88% reduction in weekly alcohol intake compared with a 20% reduction in the control arm.38 The abstinence group had a 20% reduction in AF recurrence at six months and longer delay to arrhythmia recurrence compared with the control group.
Low-level consumption of alcohol, which has been purported to reduce the risk of other cardiovascular outcomes, has not been demonstrated to be beneficial in patients with AF. Heavy alcohol consumption has been clearly linked with increased adverse events in the prevalent AF population.39,40 In our series of studies, we observed an appreciable clinical reduction in AF burden with abstinence or reduction of alcohol to three or fewer standard drinks per week.
Smoking
Smoking is an independent predictor for the development of AF in observational cohort studies, with up to double the risk shown in the ARIC study.41-43 Increased sympathetic tone, oxidative stress, inflammation and atrial fibrosis are thought to promote AF. Smoking also increases the risk of thromboembolism and mortality associated with AF.44
The risk of AF is lower in former smokers compared with current smokers and those who have recently quit smoking, which supports the pursuit of smoking cessation in all patients with AF.41 Smoking cessation is of course also a key component of reducing overall cardiovascular risk. The recommended approach is using ‘the 5 As’: ask, advise, assess, assist, arrange follow up.45
Cholesterol
Data from observational studies on the association between lipid levels and AF suggest a ‘cholesterol paradox’, with increased low density lipoprotein (LDL) and total cholesterol levels associated with reduced AF development.46,47 Meta-analysis of randomised data has shown a signal of reduced AF recurrence in patients treated with statins, but the most convincing data is in patients undergoing cardiac surgery or with myocardial infarction. There is no clear statin dose or target LDL cholesterol level associated with reduced AF.48 Any treatment for dyslipidaemia should therefore be guided by overall cardiovascular risk or established conditions. However, in our clinic we have aimed initially for improvement through dietary changes. If the LDL cholesterol level is above 2.6 mmol/L after three months, we initiate statin therapy. If the triglyceride level is above 2.6 mmol/L then we add fibrates. In the setting of a normal LDL cholesterol level, should the triglyceride level exceed 5.6 mmol/L then we start fibrates. Review by an endocrinologist is undertaken for those who have not responded to initial treatments.
Evidence for risk factor modification
A growing body of evidence, based on delivery of a comprehensive risk factor modification intervention encompassing the broad range of AF risk factors, demonstrates clear benefit in reducing AF burden and progression.4-6 Figure 2 summarises the evidence for comprehensively managing risk factors for individuals with AF.4-6,15,17
{kind=link}
Need for comprehensive risk factor modification
Addressing only a single risk factor is often not sufficient as most patients with AF have several coexistent risk factors, all of which contribute to the development and progression of AF. The beneficial effect of treating a single risk factor seems to be mostly in those individuals where there is a dominant risk factor in an extreme state. Evidence for this has been demonstrated with severe hypertension, alcohol use and, anecdotally, for the treatment of sleep apnoea.24,38,49,50 In the context of multiple risk factors with modest contribution, such an isolated strategy has little if any benefit.24 We would therefore advocate for the use of a comprehensive approach that targets each risk factor.
Delivery of risk factor modification
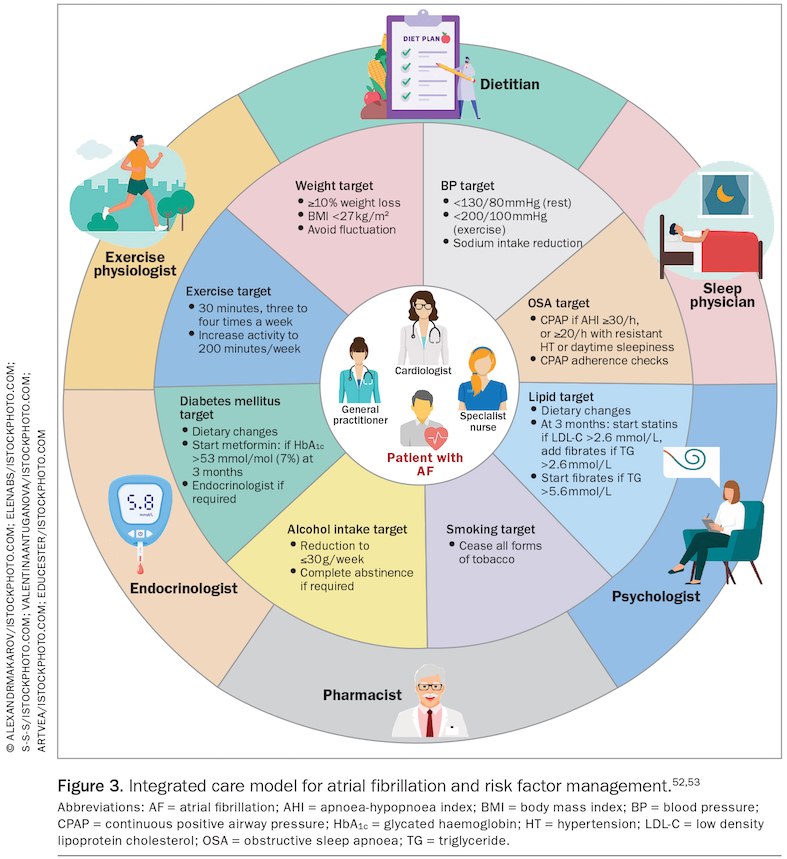
There is now considerable evidence that a structured, co-ordinated and integrated approach to chronic disease management results in better compliance and outcomes. Specialised AF clinics have demonstrated better guideline adherence, enhanced patient compliance and improved clinical outcomes.51 The introduction of risk factor management has increased the complexity of service delivery. This has called for an integrated care approach to delivery (Figure 3).52,53 Central to this delivery is the individual with AF. Most of the delivery is managed by a core group of healthcare professionals, in which the GP has a pivotal role, as well as the subspecialists required for a given individual.
{kind=link}
In our clinic, we have found the separation of AF management from risk factor management to be a useful strategy. This has been largely to avoid information overload for patients. This has been effectively delivered using physicians and nurses with support from other multidisciplinary team members. A dedicated risk factor clinic model shows the most encouraging evidence to date, and is now enshrined in national and international guidelines, including the 2018 National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand: Australian Clinical Guidelines for the Diagnosis and Management of Atrial Fibrillation, the 2019 American Heart Association (AHA)/American College of Cardiology (ACC)/Heart Rhythm Society (HRS) Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation, and the 2020 European Society of Cardiology Guidelines for the Diagnosis and Management of Atrial Fibrillation.54-56 The key components of this model are patient-centred care, a lifestyle journal, an incremental approach, flexible follow up, surveillance of medication and other treatments, and OSA screening and management (Box 2).
{kind=link}
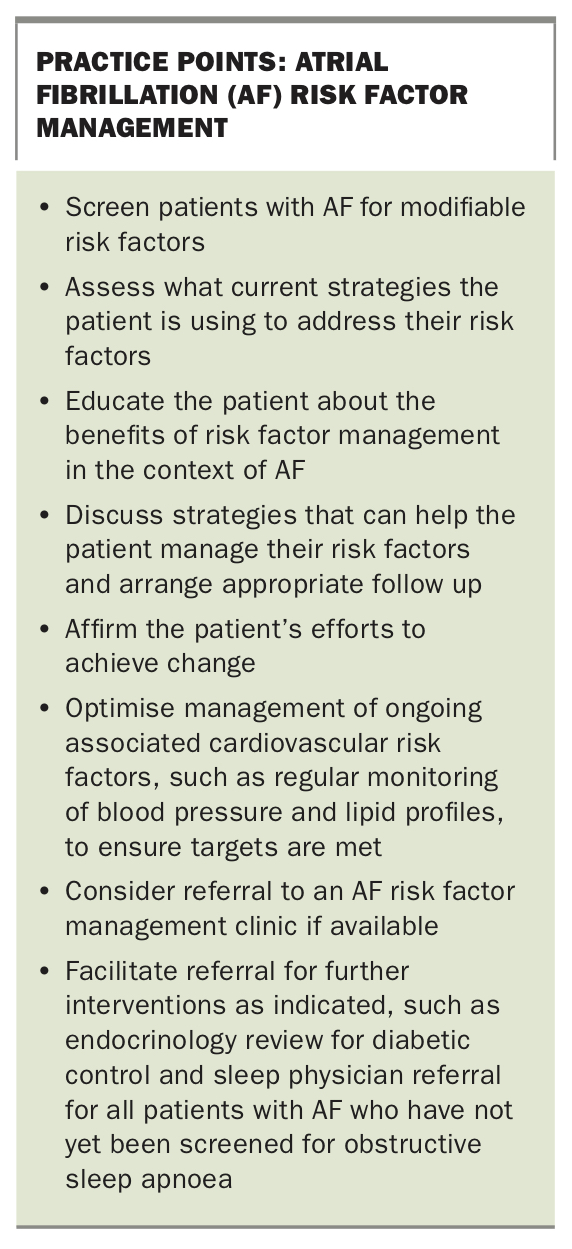
Regardless of whether patients have access to a structured AF risk factor modification clinic, the role of the GP is crucial in assisting patients to gain better risk factor control. When access to a structured AF risk factor management clinic is not available, it is worthwhile exploring delivery of risk factor modification components through institution of a GP-led chronic disease management plan with involvement of practice nurses and available allied health professionals. The primary care team can provide essential reinforcement of the message that patient participation is key and can enhance patient motivation for positive lifestyle changes by using the same key components of an AF risk factor modification clinic (see Practice Points box).
{kind=link}
Conclusion
Risk factor modification has become a key pillar of atrial fibrillation care and is recognised in current international guidelines. Patient-centred care and engagement to modify obesity, physical inactivity, hypertension, dyslipidaemia, diabetes mellitus, OSA, and alcohol and tobacco use ensures a cost-effective contribution to long-term improvement in AF outcomes. GPs play a critical role in this to reduce the condition's rapidly growing burden. MT
COMPETING INTERESTS: None.