Atrial fibrillation: management of older patients

The primary care management of atrial fibrillation requires a careful assessment of age-based factors and the risk of stroke, while balancing the increased risk of treatment-related adverse events and medication misadventure.
Correction
A correction for this article has been published in the October 2022 issue of Medicine Today. The online version and the full text PDF of this article (see link above) have been corrected.
- GPs are central to the long-term primary care management of patients with atrial fibrillation (AF), noting that the target population of older people is both expanding and further rapidly ageing, rendering decision-making even more complex.
- A patient-centred treatment plan should focus on three key goals: detecting AF to enable early treatment initiation, managing the dysrhythmia to optimise cardiac function and prevent symptoms, and preventing thromboembolism to reduce stroke risk.
- An individualised, evidence-based approach to AF management requires comprehensive assessment of age-related factors to identify treatment goals, the risk-benefit profile of available treatments, and any medication management issues, with documentation of decision-making and regular reassessment to identify any changes.
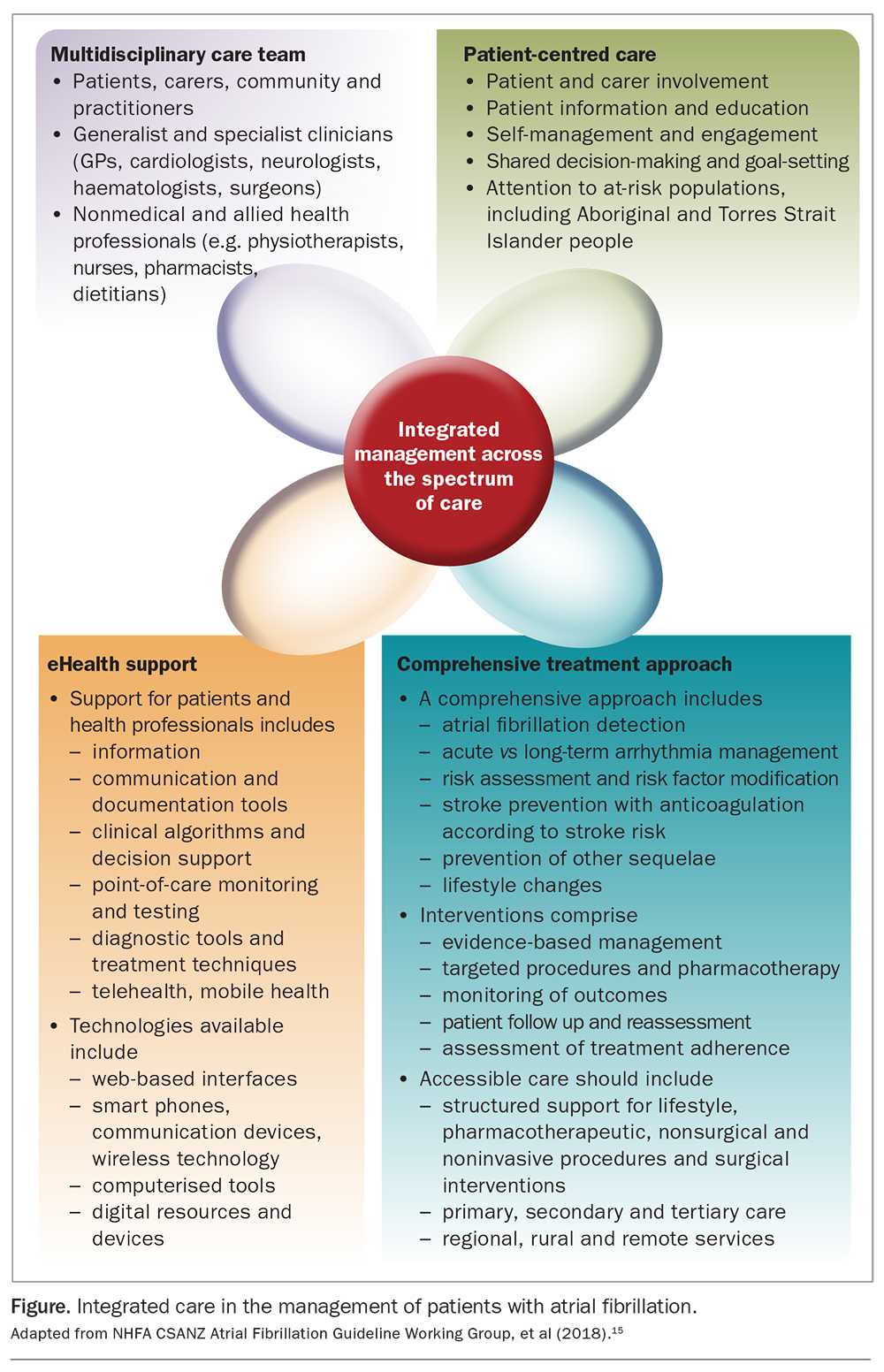
- An integrated care approach can help GPs optimise AF management in older people, drawing on the collective expertise and support of the wider healthcare team, particularly as both risk assessments and treatment goals change with increasing age.
Nonvalvular atrial fibrillation (AF) goes hand in hand with advancing age, which is an independent and nonmodifiable risk factor for AF, stroke and other cardiovascular risk factors, all adding to the risk of AF-related stroke. AF affects about 2% of the population and an estimated 5% of those aged 55 years and older.1-3 It causes significant symptoms that can reduce quality of life and is associated with an increased risk of stroke, poorer outcomes after stroke and increased mortality.
AF is routinely detected and managed in general practice, accounting for one of the highest frequencies of repeat GP visits per year and highest management ratios (ratio of the proportion of encounters at which the condition is managed to the prevalence of the condition among patients at clinical encounters).4 With population ageing, the burden of AF and attributable stroke is increasing in Australia. The complexity of management of AF also increases in older patients.
This article reviews the primary care management of AF in older people, flagging key treatment goals and guideline recommendations. Clinical considerations and practical management strategies are also discussed.
Burden of AF in primary care
AF has significant anatomical, haemodynamic and thrombotic consequences and causes symptoms such as palpitations, dyspnoea, angina, fatigue, generalised weakness, presyncope or syncope and reduced exercise tolerance, which can adversely affect quality of life.5 AF is also associated with a five- to sevenfold increased risk of stroke and poorer neurological outcomes after stroke.6 AF-related strokes are more severe, disabling and likely to be fatal than strokes caused by other conditions.7,8 In addition, AF itself increases mortality, being reported as the underlying or associated cause in 9% of total deaths.2
Given the clinical consequences of AF, it is not surprising that 1% of all GP consultations in Australia are directly related to AF, and it accounts for 2.4% of all chronic problems managed in general practice.4 A higher proportion of consultations involve AF as a secondary diagnosis or comorbid condition. It is among the circulatory and endocrine or metabolic disorders that encompass the ‘other most common’ adult conditions (hypertension, lipid disorders, diabetes, obesity, thyroid disorders and diagnosed ischaemic or cardiovascular heart disease) managed in general practice and which are key risk factors for AF.9
AF and age
Much of the complexity of AF management relates to the impact of patient age, as well as the increasing burden in primary care. The prevalence of diagnosed AF increases from 2% in the general adult population to 10% in those aged over 65 years, and about 20% in those aged 80 years or older.1,10-12 The incidence and prevalence of AF doubles for each advancing decade of life.13 Australian data modelling predicts a doubling in the number of AF cases among older age groups from 2014 to 2034.3
The risk of AF-related stroke also significantly increases with advancing age. It rises from 1.5% for those aged 50 to 59 years to 23.5% for those aged 80 to 89 years, with about 40% of strokes in patients aged over 80 years directly attributable to AF.14
Fundamentals of primary care management of AF in older people
GPs are central to AF management, drawing on specialist consultation as appropriate. AF is a major reason for referral to cardiologists (13% of referrals), second only to one of its key risk factors, ischaemic heart disease (15%).4 However, optimal management of older patients with AF requires additional expertise and resources within an integrated care approach (Figure).15 This may involve geriatricians (regarding geriatric syndromes), allied health professionals, including physiotherapists (mobility and falls risk), occupational therapists (functional ability and independence in self-care), social workers (financial and social support) and pharmacists (medication management, drug-related problems and medication adherence assessments), and practice nurses (point-of-care assessments, monitoring, patient education and care co-ordination).
{kind=link}
The need for optimal management of AF to maintain good circulatory health, improve quality of life and prevent stroke is clear, underpinned by evidence from more ‘inclusive’ clinical trials involving ‘real world’ patients and advances in diagnostics, risk assessment, rhythm management and anticoagulation therapies. However, clinical advances have not kept pace with the rapidly ageing population and the evolving AF burden in the ‘old’ old, in whom comorbidities and frailty have an additive negative impact on health.5 Very old age also independently predicts poor short- and long-term outcomes after stroke, reflecting increased hospitalisations for AF-related adverse events among older age groups.14,16
Nevertheless, arbitrary age thresholds used in clinical guidelines, often derived from the inclusion and exclusion criteria in clinical trials, do not correlate well with actual medication behaviour and treatment response in real-world patients.17 Treatment planning needs to be individualised as much as possible.
Treatment goal: AF screening and diagnosis
The incidence of AF increases sharply after the age of 65 years.18 With a mean life expectancy of 85.3 years in Australia, there are at least 20 years of optimal health, independent functioning and quality of life to be preserved.19 Early detection of AF enables early prophylaxis and treatment to improve cardiovascular function, prevent long-term complications, such as structural cardiac changes and heart failure, and avoid stroke. Also potentially amenable to early intervention are the pathophysiological mechanisms underpinning cognitive impairment and dementia in AF, such as cerebral microinfarction, AF-related cerebral hypoperfusion, inflammation, microhaemorrhage, brain atrophy and systemic atherosclerotic vascular disease.20,21 Further, initiation of new therapies is less complex in the ‘young’ old than in the ‘old’ old, before cognitive and functional changes reduce the capacity to adhere to pharmacotherapy and lifestyle measures, manage treatment changes and self-monitor.
Reliance on patients presenting with AF symptoms to prompt diagnostic investigation can miss up to 40% of AF cases, as symptoms such as palpitations, chest discomfort, dizziness or syncope, dyspnoea and fatigue are both nonspecific and common in older people.22-25 Paroxysms of AF may be asymptomatic (‘silent’ AF), with poor correlation between AF and symptoms, particularly in the very old in whom sedentary living reduces the likelihood of acute vagally or adrenergically stimulated AF. Nevertheless, asymptomatic or subclinical AF is associated with a 2.5-fold increase in stroke risk compared with no AF.26
In the absence of AF screening, the first clinical manifestation of AF may be stroke.24 Half of all AF cases identified in patients with ischaemic stroke or transient ischaemic attack are asymptomatic.27 GPs are uniquely placed to screen and initiate management for AF. In Australia, more than 90% of adults aged 65 years and over see their GP at least annually, and around 70% see their GP two or more times per year.28
Approach to screening and diagnosis
A proactive approach to detecting AF in older people is warranted and endorsed by current Australian guidelines.15 These recommend opportunistic point-of-care screening in the clinic or community for people aged 65 years and over by pulse palpation or an ECG rhythm strip. In primary care, the GP, practice nurse or GP-based pharmacist can incorporate pulse palpation into standard consultations or targeted services. For screening, a medical-quality single-lead ECG trace is preferred to pulse-taking or pulse-based devices such as photoplethysmography and blood pressure oscillometry.
Detection of an irregular pulse should be followed by a diagnostic ECG or ECG rhythm strip using a handheld ECG to confirm the diagnosis of AF. Given the episodic nature of AF, innovative wearable ‘rhythm monitoring’ technology is also being explored, although uncertainty remains about its diagnostic accuracy, the clinical significance of short asymptomatic bursts of AF and its feasibility in older people and overall cost-effectiveness.29 However, any method that might help AF detection in older people should be considered as an option, particularly when routine access to health services is restricted, such as in regional and rural areas and for patients with reduced mobility.
A diagnostic work up should assess serum levels of potassium, sodium, magnesium and calcium. Abnormalities may underly the cardiac arrhythmia or predispose to drug toxicity (e.g. for digoxin).15
Recommendation on screening and prevention – screening for silent AF
Opportunistic point-of-care screening in the clinic or community should be conducted in people aged 65 years or more (GRADE quality of evidence, moderate; strength of recommendation, strong).15
Treatment goal: dysrhythmia management
Treating the underlying dysrhythmia in AF by controlling the cardiac rhythm, rate or both is a key goal. Current guidelines recommend a strategy of either rhythm control with classic antiarrhythmic drugs or rate control.15 Although rhythm control seems inherently preferable, antiarrhythmic drugs reduce the risk of AF recurrence by only 50% and do not reduce stroke risk and mortality more than rate control. Rate control may be preferred in older people when AF is relatively asymptomatic or when restoration or maintenance of normal sinus rhythm may not be possible because of prolonged, irreversible cardiac changes (e.g. atrial enlargement due to long-standing AF).30 For ‘young’ old patients experiencing frequent and symptomatic paroxysms of AF, particularly after physical activity, or left ventricular dysfunction, rhythm control is preferred and is advantageous in enabling physical activity for broader health benefits.15
The approach chosen should be individualised, communicated in the treatment plan and monitored by ECG, measurement of ventricular rate and surveillance for emergent cardiomyopathy or overt heart failure. This is important at both the ‘macro’ level of decision-making (rhythm versus rate control) and the ‘micro’ level (choice of pharmacological agent).
Recommendation on arrhythmia management – rhythm control versus rate control
A rhythm-control or a rate-control strategy should be selected, documented and communicated for all AF patients, and this strategy should be reviewed regularly (GRADE quality of evidence, low; strength of recommendation, strong).15
Choice of medication for dysrhythmia
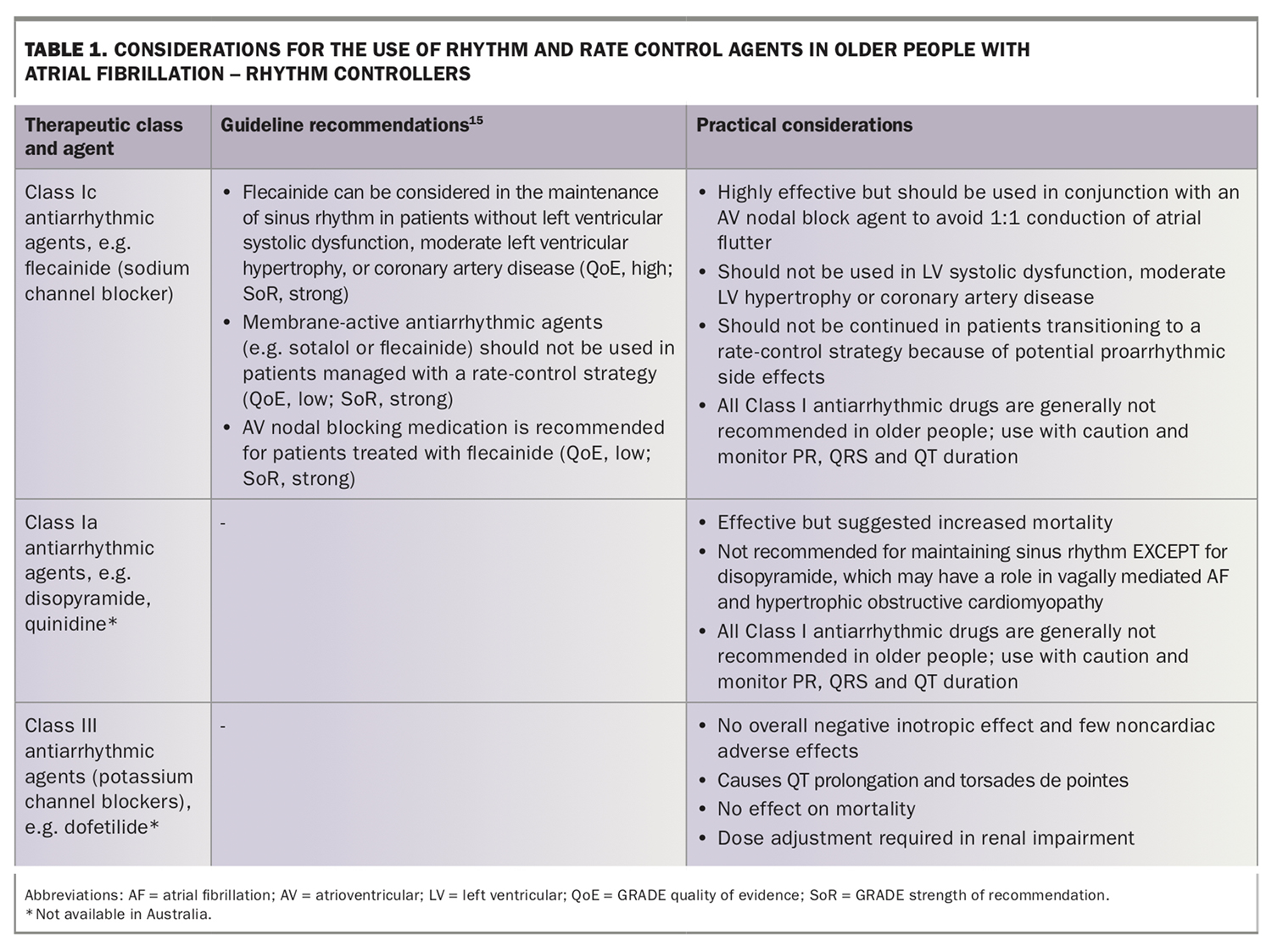
Currently available pharmacotherapeutic options for dysrhythmia include:
- rhythm controllers (e.g. flecainide)
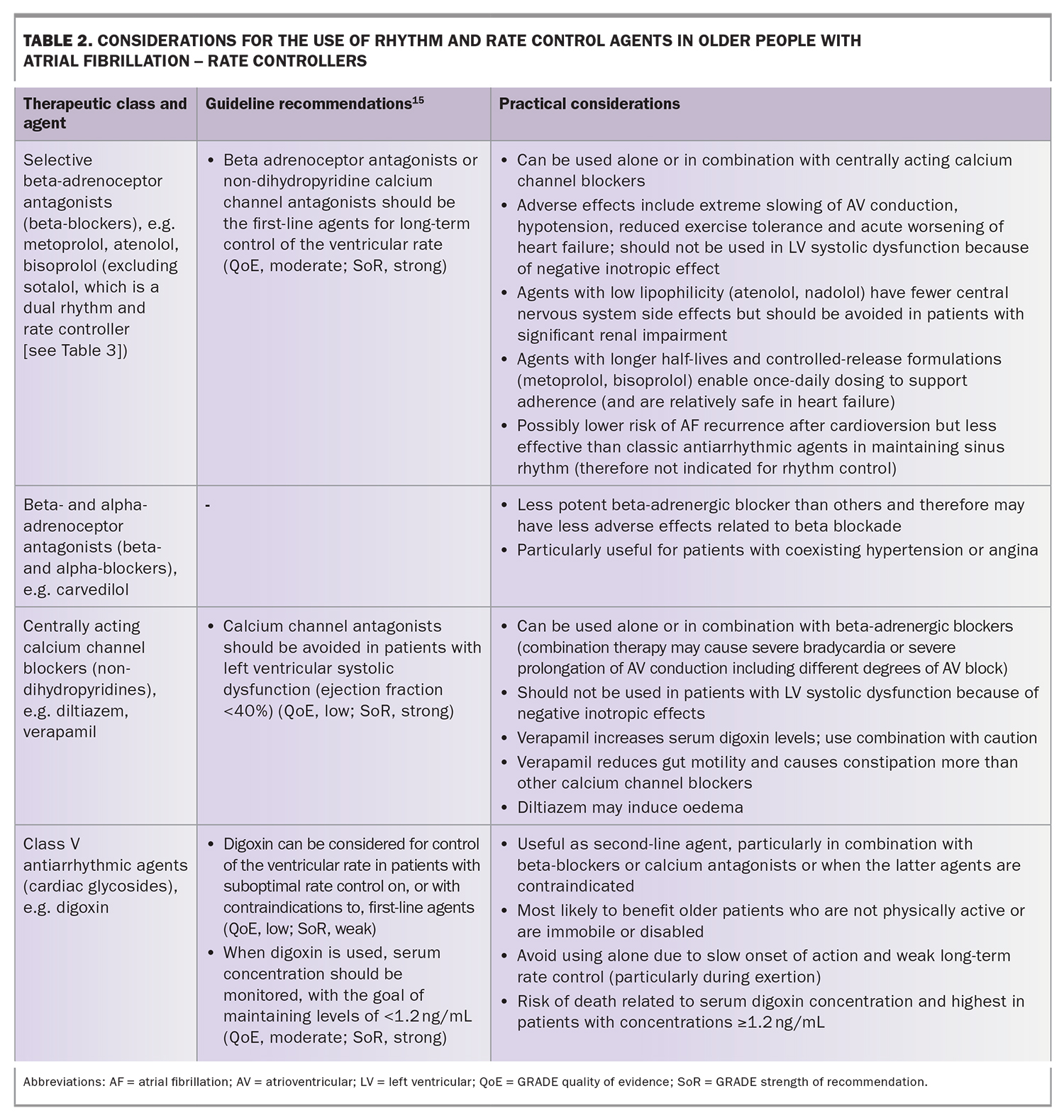
- rate controllers (e.g. beta-adrenoceptor antagonists, the centrally acting calcium channel blockers diltiazem and verapamil, and digoxin)
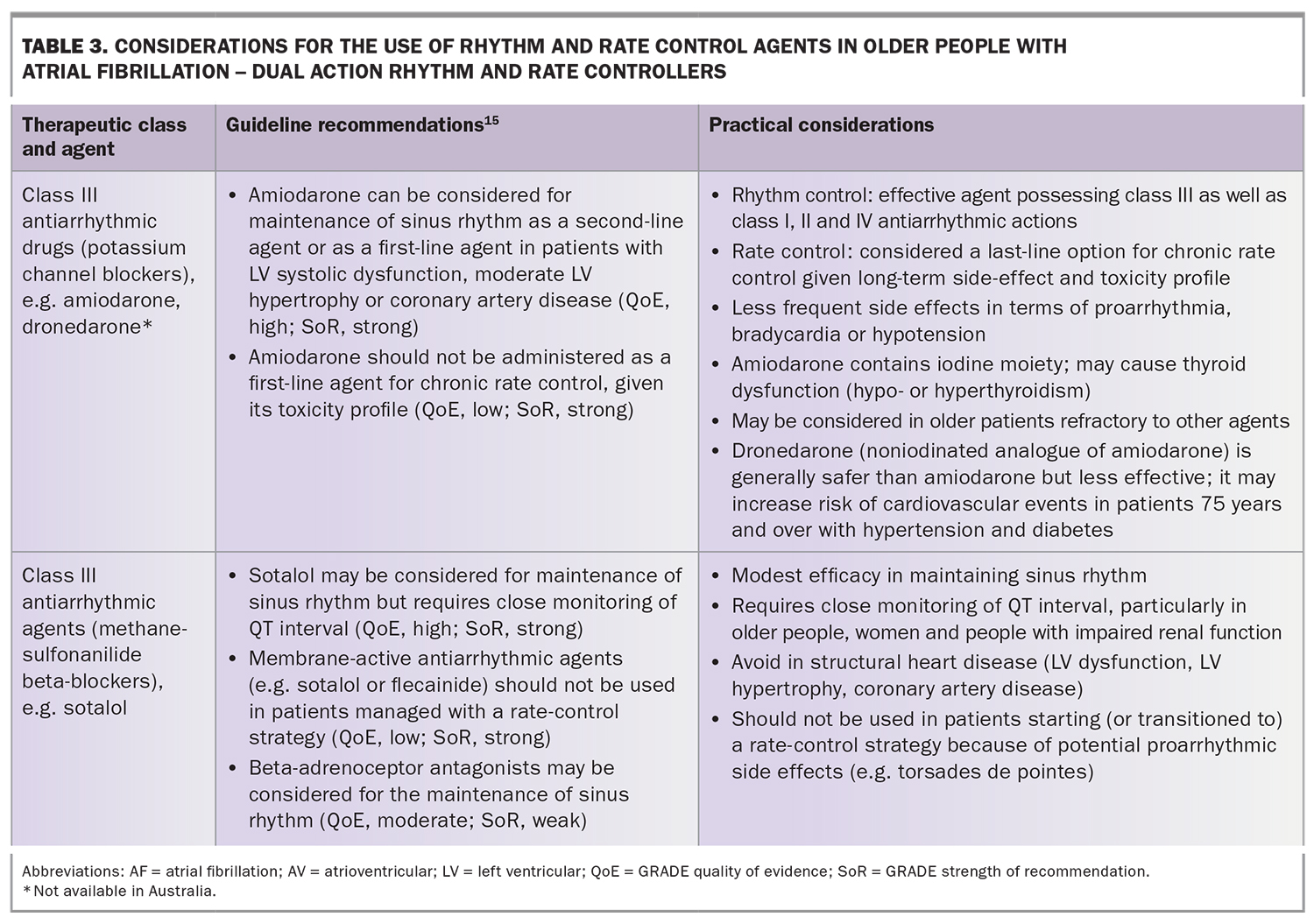
- dual-action agents possessing both rhythm and rate control properties (e.g. amiodarone and sotalol).
Specific considerations apply to the use of each option in older patients, particularly those with heart, renal or hepatic disease (Table 1, Table 2 and Table 3).30 Although the safety of rhythm controllers in older people has been a concern, with some studies suggesting an increase in mortality, more recent studies suggest that a more liberal approach towards prescribing a rhythm control strategy for older patients with AF may be warranted and seems safe.31 Pharmacological rate control also requires careful consideration and may not always be appropriate. Instead, catheter ablation of the atrioventricular node with permanent pacing should be considered, although the efficacy is lower in ‘old’ old patients because of AF permanency, frailty and comorbidities such as heart disease, sleep apnoea and obesity.
{kind=link}
{kind=link}
{kind=link}
Treatment goal: stroke risk assessment and stroke prevention
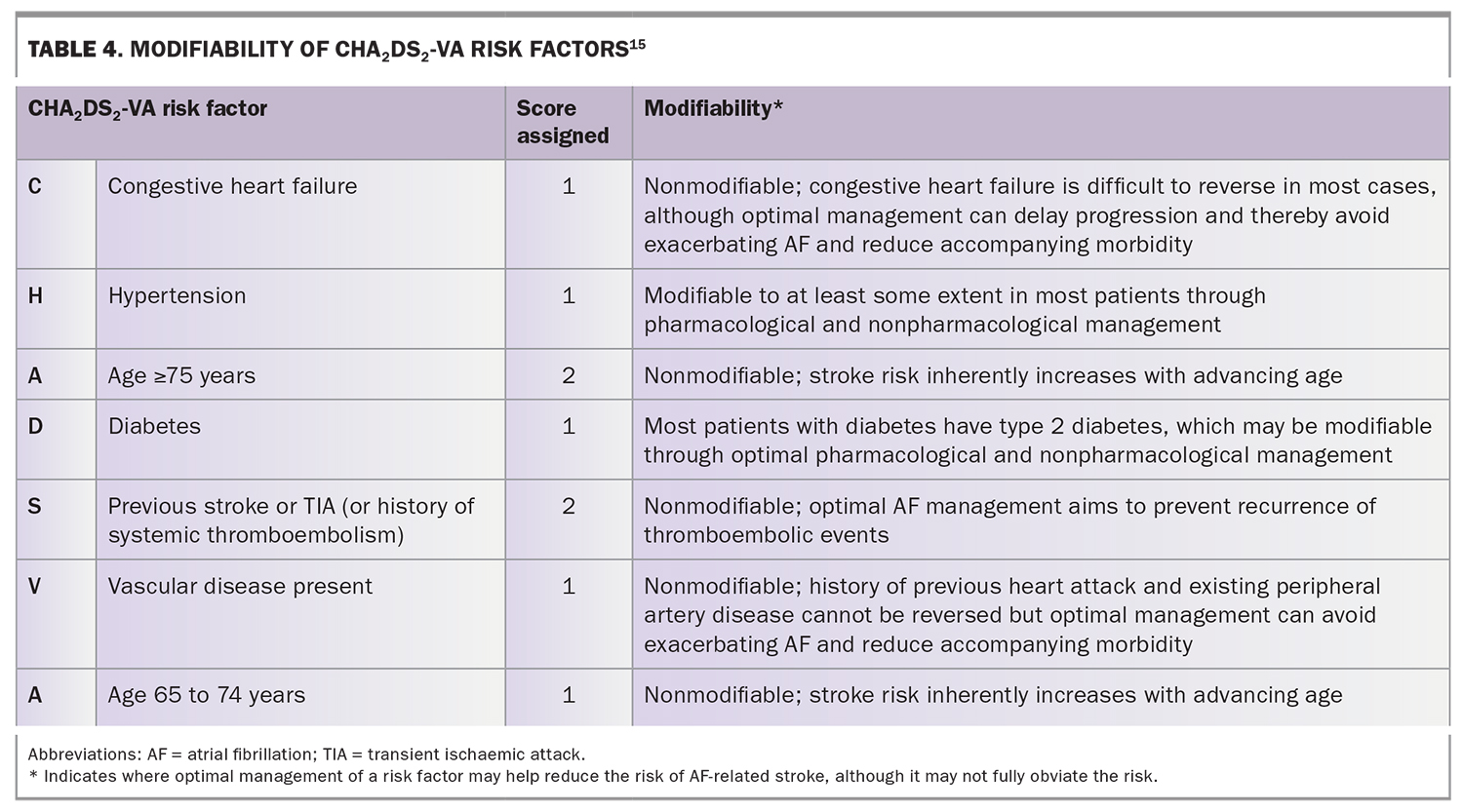
Antiarrhythmic strategies do not obviate the risk of atrial thromboembolism and therefore do not reduce the risk stroke in patients with AF. The risk of stroke remains high in older people as advancing age itself is a core risk factor. Using the guideline-advocated CHA2DS2-VA stroke risk prediction score, where a threshold of 1 to 2 points confers a higher risk of stroke and 1 point is assigned for age 65 to 74 years and 2 points for age 75 years or over, then anticoagulation is indicated, or at least should be considered, in almost all older people with AF (Table 4).15
{kind=link}
With stroke risk following a continuum rather than a dichotomous classification, risk scoring systems such as the CHA2DS2-VA score can reliably identify patients who should not receive anticoagulants because of a low risk of thromboembolism. They can also identify modifiable risk factors for management, although even well controlled risk factors still contribute to the overall risk of stroke.
The failure to assess and recognise the high risk of stroke in older people with AF, while overestimating any potential risk of treatment-related bleeding has resulted in continued underutilisation of prophylactic anticoagulants, leaving patients susceptible to devastating AF complications.32-34 Cautious prescribing has been underpinned by fears of bleeding after decades of reliance on the pharmacologically complex and practically challenging vitamin K antagonist, warfarin. There are specific concerns about iatrogenic intracranial haemorrhage and life-threatening major bleeds in older people in whom frailty, falls risk and multimorbidities complicate decision-making.32,35 However, although studies have shown that frail older patients with AF are significantly less likely to receive an anticoagulant, they have also shown that these same patients are more vulnerable to adverse clinical outcomes (embolic stroke, higher mortality), with or without therapy.36,37 Therefore, clinical guidelines reinforce that old age, frailty and falls risk per se are not absolute contraindications for anticoagulation in AF.38 Nevertheless, Australian GPs have also expressed concern about medication safety and its likely impact on patient adherence as a major determinant in decision-making.39
Recommendation on stroke prevention – anticoagulation
Oral anticoagulation therapy to prevent stroke and systemic embolism is recommended in patients with nonvalvular AF whose CA2DS2-VA score is 2 or more, unless there are contraindications to anticoagulation (GRADE quality of evidence, high; strength of recommendation, strong).15
Recommendation on stroke prevention – prediction and minimisation of bleeding risk
Reversible bleeding factors should be identified and corrected in AF patients for whom anticoagulation is indicated (GRADE quality of evidence, low; strength of recommendation, strong).15
Choice of anticoagulant
The direct-acting oral anticoagulants (DOACs), also known as non-vitamin K antagonist oral anticoagulants (NOACs), have expanded the treatment armamentarium. They include dabigatran, rivaroxaban and apixaban. DOACs offer more pharmacodynamically and pharmacokinetically predictable treatment, without the need for routine monitoring of coagulation parameters, and with relatively lower potential for interactions with drugs, herbs and food, overcoming previously cited concerns.
Importantly, in patients aged 75 years and over, DOACs are as effective as warfarin for stroke prevention and in some cases superior, with a better safety profile overall, including lower rates of intracranial haemorrhage.40 Limited evidence also suggests that DOACs might be superior in preventing cognitive impairment, which confers additional advantages in avoiding dementia-related treatment nonadherence.38 DOACs are therefore recommended as first-line agents for stroke prevention in AF.15
Recommendation on oral anticoagulation
When oral anticoagulation is initiated in a patient with nonvalvular AF, a DOAC – apixaban, dabigatran or rivaroxaban – is recommended in preference to warfarin (GRADE quality of evidence, moderate; strength of recommendation, strong).15
Other considerations regarding anticoagulants
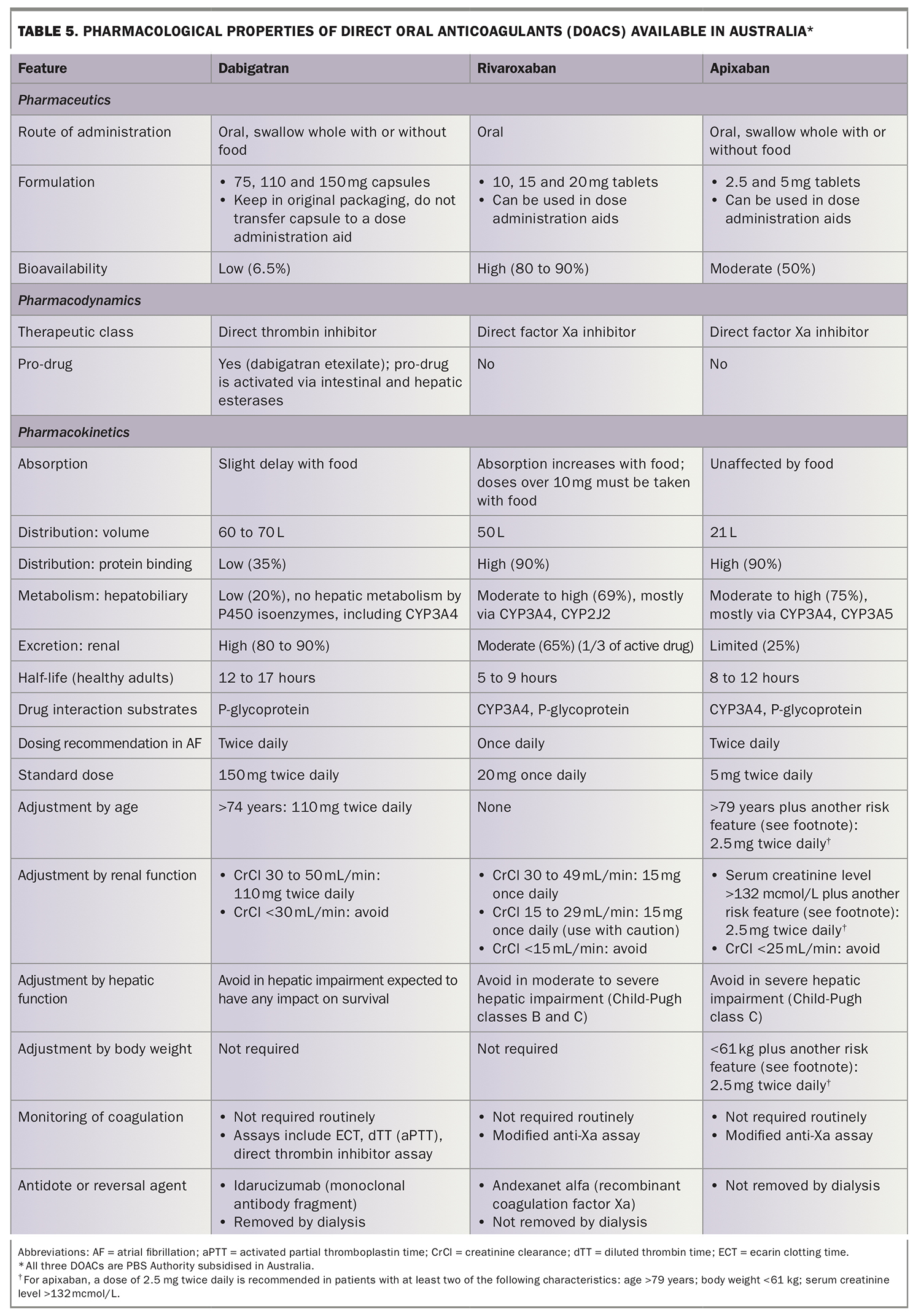
Other considerations regarding the use of DOACs in older people are shown in Table 5. They include:
{kind=link}
- dosage adjustment by age (e.g. dabigatran and apixaban) and renal impairment (more so with dabigatran, less so with rivaroxaban and apixaban)
- contraindications in patients with severe liver impairment (e.g. apixaban and rivaroxaban)
- limited access to specific antidotes for treating DOAC-related overanticoagulation
- the need for twice daily dosing (dabigatran and apixaban), which may reduce adherence, especially in older patients taking many medications.
Further, the DOACs dabigatran and rivaroxaban are not as well tolerated as warfarin in patients with gastrointestinal disease.
In summary, the DOACs are not devoid of risk.41 Further, knowledge gaps exist regarding optimal dosing in very old patients, especially those with mild-to-moderate renal failure or very low or very high body mass index, and those concurrently taking medications predisposing to metabolic drug interactions (all DOACs are eliminated by either CYP metabolic enzymes or permeability glycoprotein transporters).38
In practice, optimal patient-centred, individualised anticoagulation decisions in older people require comprehensive assessment, meaningful engagement, integration into existing systems and processes, and possibly overcoming health professional and patient misperceptions about treatment options.33,42-44 An integrated, multidisciplinary care approach can help overcome some of these challenges to individualised, risk-based decision-making (Figure).32,41
Drawing on multidisciplinary expertise can facilitate:
- full assessment of the patient’s AF-related stroke risk to ascertain the benefit of anticoagulation in the individual relative to treatment risks
- rigorous assessment of the potential for bleeding, identifying and addressing any modifiable risk factors (e.g. underlying conditions, drug interactions)
- thorough review of the patient’s medical history (comorbidities, baseline kidney function, cognitive status, mobility and falls risk, nutritional status and life expectancy)40 and medication history (drug regimen, polypharmacy and medication adherence) to identify potential treatment contraindications, drug interactions and adverse events and any need for dosage adjustment
- careful consideration of the pharmacological properties of all available anticoagulant options against the individual patient’s characteristics
- ongoing review of the patient’s predicted treatment risk versus benefit profile, taking into account changing risks and treatment goals over time as the patient ages from ‘young’ old to ‘old’ old, as well as the occurrence of any strokes and bleeds and coagulation parameters
- identification of alternative approaches, such as percutaneous left atrial appendage closure in older patients with contraindications to oral anticoagulants.42
Recommendations on integrated management
An integrated care approach is recommended; such an approach aims to provide patient-centred comprehensive treatment delivered by a multidisciplinary team (GRADE quality of evidence, high; strength of recommendation, strong).15
Targeted patient education is recommended throughout the continuum of AF management (GRADE quality of evidence, high; strength of recommendation, strong).15
Shared decision-making should consider patients’ beliefs, values and preferences, with a goal of empowering patients to undertake self-management (GRADE quality of evidence, moderate; strength of recommendation, strong).15
Treatment goals should be developed in partnership with patients, and communicated with all members of the multidisciplinary team (GRADE quality of evidence, low; strength of recommendation, strong).15
eHealth tools and resources should be used by patients and health professionals, to support the integrated management of AF (GRADE quality of evidence, high; strength of recommendation, strong).15
All patients prescribed pharmacotherapy for the management of AF, including core rhythm control and anticoagulation therapies, should have their treatment adherence and persistence regularly monitored and supported using accessible and patient-centred strategies (GRADE quality of evidence, low; strength of recommendation, strong).15
Treatment goal: medication management to support therapeutic strategies
Initiating treatment for AF significantly increases the medication burden for patients. In addition, the risk of medication misadventure is heightened by the trilogy of old age, use of high-risk medications (antithrombotics and antiarrhythmics) and polypharmacy.45 Polypharmacy (regularly taking five or more medicines) and hyperpolypharmacy (10 or more medicines46) particularly affect the oldest patients with AF, not only because of multiple comorbidities but also because of the polypharmacy required for AF alone.
Both antiarrhythmic and anticoagulant strategies comprise agents that:
- although specifically indicated for AF, are also regarded as potentially inappropriate medications (e.g. anticoagulants and digoxin as per the Beers Criteria Medication List)
- may interact with each other (e.g. amiodarone and warfarin, digoxin and warfarin, amiodarone and DOACs, calcium channel blockers and DOACs).47
Polypharmacy is also associated with an increase in cardiovascular death and hospitalisation, reduced quality of life and poorer physical function in older people with AF.48 For this reason, the decision to initiate pharmacotherapy for AF must consider not only the risks of stroke, bleeding and medication misadventure but also increasing polypharmacy. Further, older patients may have physiological changes that affect drug pharmacokinetics and pharmacodynamics, homeostasis and risk of falls and bleeding, alongside increasing stroke risk.
Six- to 12-monthly re-evaluation of very old patients, including risk-benefit profile, is imperative because of their likely frequent and acute changes in clinical status.38 Treatment adjustments may reduce patient adherence, especially if cognition is declining. Importantly, changes in one medication, whether deliberate or inadvertent through nonadherence, may significantly affect other concurrently used medications. An integrated care approach should thus support not only decision-making and monitoring of clinical outcomes but also medication management, including assessment of adherence and regular comprehensive medication review, such as a pharmacist-led home medicines review or MedsCheck.49
Conclusion
Optimising the management of AF in older people has significant clinical benefits, including reducing symptoms, improving functional capacity, reducing cognitive decline, preventing stroke, reducing mortality and improving quality of life. However, management decisions are complex, both in terms of treatment options, as there are no ‘risk-free’ agents, and in terms of the characteristics of the target population, with many potential medical, cognitive, functional, social and iatrogenic factors. There are risks and challenges along the disease management pathway, including screening for AF, dysrhythmia management and stroke prevention, compounded by concerns around medication misadventure. An integrated care approach utilising multidisciplinary expertise can support GPs in facilitating comprehensive robust risk assessments, patient-centred individualised treatment plans and therapeutic processes. Importantly, regular re-evaluation of risks and review of treatment plans as patients age, including documentation and communication of these to both patients and the broader healthcare team, will ensure that treatment goals and strategies for AF align with patients’ changing needs. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.