Managing epistaxis – a guide for GPs

Epistaxis is a common presentation in general practice. Although most cases are benign and easily managed, some are more serious and require further assessment. Careful history and examination, especially in patients with recurrent epistaxis, can help identify red flags and prompt further investigation. An understanding of the nasal anatomy and pathophysiology behind the condition will help guide effective management.
- Differentiating between anterior and posterior epistaxis is essential for effective management.
- Red flag symptoms may indicate an underlying condition and should be identified early in the patient’s history.
- Focused examination can identify an anterior bleeding point.
- When managing epistaxis, withholding or reversing any anticoagulants or antiplatelet agents before treatment should be considered.
- Nasal packing is an effective way to achieve tamponade for heavy bleeding.
- Adequate aftercare should be discussed with patients at risk of re-bleeding.
Epistaxis is defined as bleeding from the nasal tissue and is one of the most common presentations seen in ENT and primary care practice. Although most presentations of epistaxis are minor and easily managed, significant bleeding, especially from posterior sources, can be serious if not treated appropriately. Effective management of epistaxis requires an understanding of the nasal anatomy and pathophysiology behind the condition. An algorithm outlining the management from presentation to treatment is presented in the Flowchart.
Anatomy of the nose
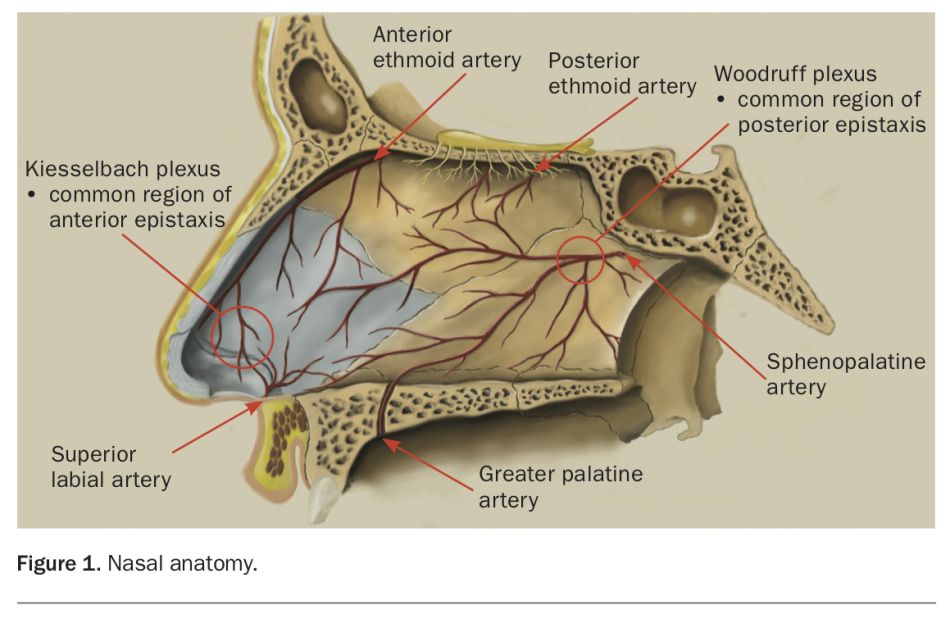
When identifying the source of epistaxis, two important arterial plexuses within the nose should be considered. Anteriorly, the Kiesselbach plexus, located at Little’s area, is a section of the anterior nasal septum where anastamoses occur between the anterior and posterior ethmoidal arteries, sphenopalatine artery, greater palatine artery and septal branch of the superior labial artery (Figure 1). As a significant vascularised portion of the nose that is readily exposed to dryness on inspiration as well as trauma from digital insertion, up to 90% of epistaxis occurs within this area. This plexus is located in the anterior nasal septum and can be readily visualised via anterior rhinoscopy. Posteriorly, the Woodruff plexus is located over the posterior middle turbinate on the lateral nasal wall and is formed by anastamoses between the sphenopalatine artery, posterior nasal artery and ascending pharyngeal artery. This plexus cannot be readily visualised without the aid of nasal endoscopy, but should be suspected when an anterior cause of bleeding is not identified. When describing the location of epistaxis, it is important to characterise not just the side of bleeding but whether bleeding is occurring from a suspected anterior or posterior source.
{kind=link}
Epidemiology
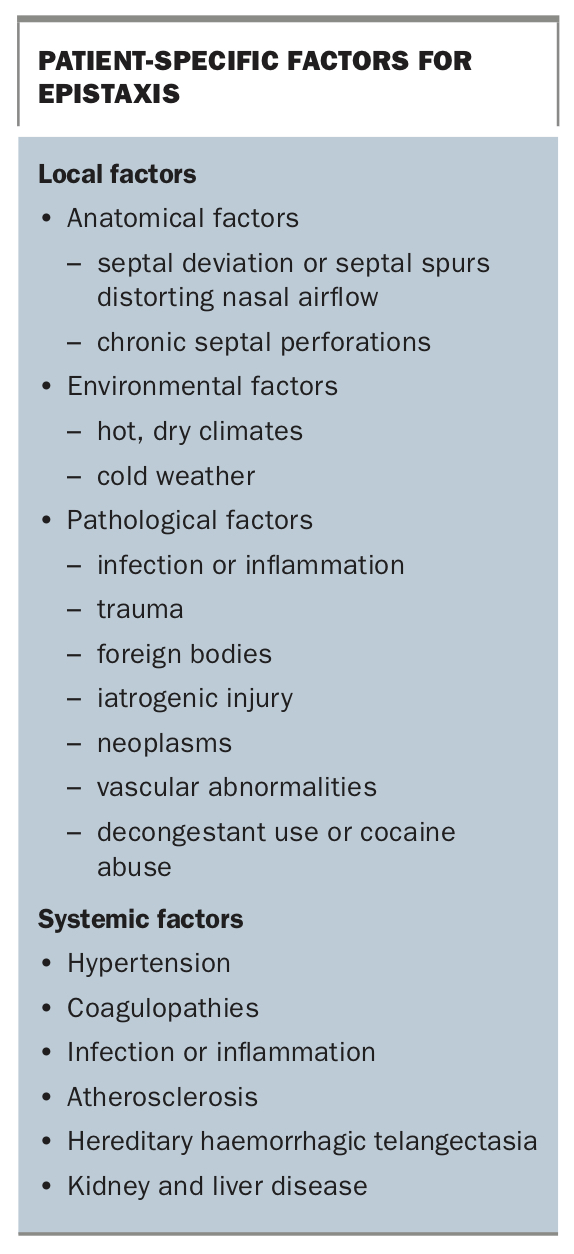
Up to 60% of the population will experience epistaxis at some point in their lives. The incidence of epistaxis is bimodal in age distribution, with peaks among people under 10 years and over 70 years of age.1 It is more common in winter months and appears to follow the circadian rhythm, with higher incidence in the morning and late afternoon. Patient-specific factors that affect the incidence of epistaxis can be broadly divided into local and systemic factors and are summarised in the Box.
{kind=link}
Assessment and first aid
For patients with recurrent epistaxis, or those predisposed to bleeding from underlying comorbidities or medication use, education on effective first aid is imperative. When bleeding occurs, the patient should be encouraged to keep their head elevated and tilted forward with external digital compression of the soft anterior cartilage of the nostrils, achieved by pinching the tip of the nose. If available, ice applied to the forehead, neck or in the mouth can promote vasoconstriction and further decrease the intensity of nosebleeds.
Following presentation, the initial assessment of epistaxis seeks to determine the severity and identify the side of bleeding. Taking a thorough patient history can help to establish important factors, including duration, volume and frequency of bleeding, as well as identify any local or systemic factors contributing to bleeding.
It is worth noting that a thorough assessment of epistaxis and subsequent treatment presents a risk for droplet transmission. In the current setting of ongoing COVID-19 infections, attention should be paid to site-specific policies governing patient assessment, and appropriate policies regarding personal protective equipment should be adhered to.2
Resuscitation
A patient with epistaxis, especially from a posterior source where active bleeding into the airway is common, may need resuscitation. Resuscitation should follow a similar airway, breathing, circulation, disability, exposure (ABCDE) approach as for any other bleeding emergency. To reduce the risk of active bleeding into the airway, position the patient upright with the head tilted forward and encourage them to spit up any blood in the mouth. A Yankauer sucker can also be used to help clear any bleeding in the back of the mouth. Assessing the patient’s vital signs, especially heart rate and blood pressure, can help determine haemodynamic instability. Large bore intravenous access should be established early, with blood samples sent for a full blood count, coagulation profile and blood group typing and screening. This will also allow for the commencement of intravenous fluids for fluid resuscitation. Patients with epistaxis that does not settle with simple bedside intervention should be referred for urgent review to an emergency department or ENT specialist.
Examination
After the patient has received appropriate resuscitation, a focused assessment of the nasal septum and cavity should be performed to identify the bleeding point and guide treatment. With equipment on hand, the patient can be instructed to gently remove pressure from the nose. Examination begins with an anterior examination of both nostrils aided by a good light source, such as a headlight or pentorch. The use of nasal decongestant sprays, such a cophenylcaine (phenylephrine and lignocaine), to vasoconstrict the nose can significantly improve patient comfort during examination and reduce bleeding into the visualised field. In low volume epistaxis, adequate decongestion alone can sometimes settle bleeding. A small bore suction device such as a Frazier or Y-suction catheter can be useful to help clear blood from the nostrils, and a Thudicum speculum can be used to open the nostrils to allow for a clearer view.
Classically, anterior causes of epistaxis present with bleeding visible to the nostrils, whereas posterior causes present with the sensation of blood running down the back of the nose and any active bleeding is more easily visualised via the mouth. All visible surfaces of the nasal septum and lateral nasal wall should be carefully inspected, paying attention for any bleeding or prominent vasculature to Little’s area, as it is the most common site of bleeding. Some actions, such as cocaine abuse, can result in diffuse mucosal ooze, wherein a single bleeding point is not always encountered. When an anterior bleeding point is not visible, the posterior pharyngeal wall should be inspected via the mouth for postnasal bleeding, the presence of which suggests posterior epistaxis, until further assessment can be performed using a nasal endoscope by an ENT specialist.
Red flags
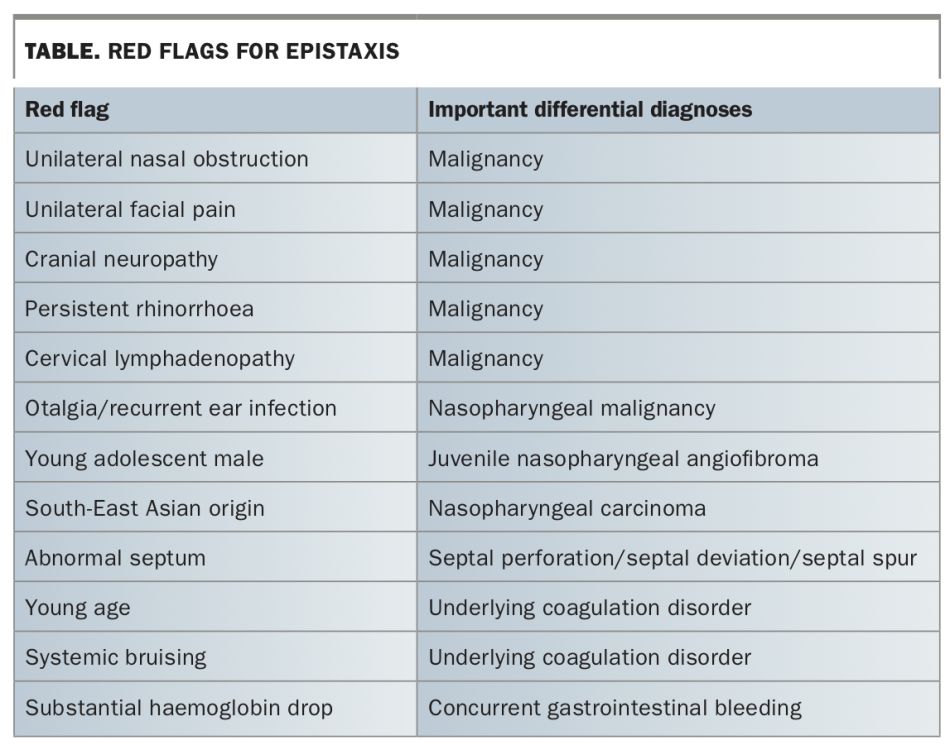
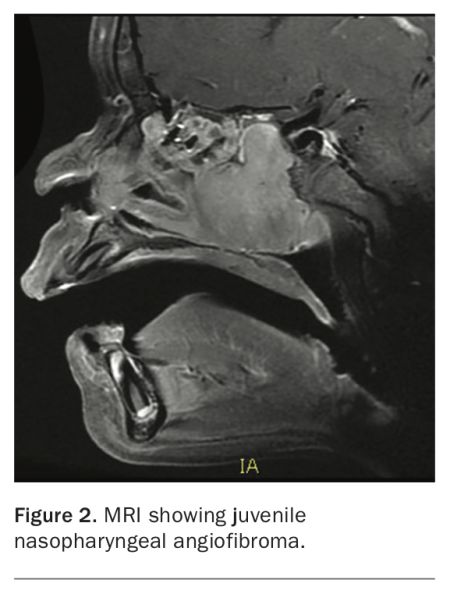
Although many presentations of epistaxis are benign and can be managed conservatively or with cauterisation, for patients with recurrent epistaxis, reviewing for the presence of ‘red flag’ symptoms during history and examination can raise suspicion of a differential diagnosis and prompt further investigation (Table). Most cases of epistaxis tend to be unilateral; however, concurrent nasal obstruction, facial pain, persistent rhinorrhoea, lymphadenopathy or cranial nerve deficits should raise concern early on for the possibility of malignancy. One important diagnosis not to miss is juvenile nasopharyngeal angiofibroma, a benign but highly vascularised tumour most common in young adolescent males, with a median age of onset of 15 years (Figure 2). Patients in this age group who have new onset epistaxis with no clear visualised bleeding source or with recurrent unilateral bleeding should be referred to an ENT specialist for assessment, where formal nasal endoscopic evaluation can be organised.
{kind=link}
{kind=link}
Epistaxis with concurrent otalgia or recurrent ear infection secondary to eustachian tube dysfunction are red flags for the presence of a nasopharyngeal lesion. This is especially so for people of South-East Asian descent, who have a prevalence rate of nasopharyngeal carcinoma five times higher than the rest of the world. For any patient suspected of an underlying malignancy, prompt referral to an ENT specialist for assessment is recommended.
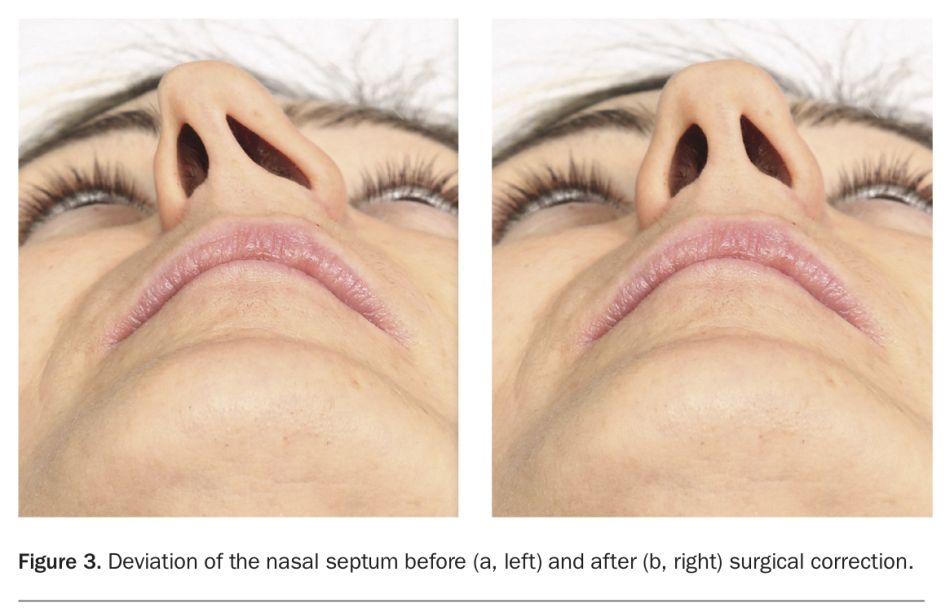
A number of changes involving the nasal septum can be associated with recurrent epistaxis. Any overt deviation of the nasal septum, including the presence of a nasal septal spur, can disrupt the normal passage of air through the nose (Figure 3). This in turn leads to abnormal desiccation of sections of the nasal septum, with drying and subsequent bleeding from sections of mucosa. Chronic decongestant use, cocaine abuse, previous nasal surgery, nasal piercings and recurrent trauma to the nasal septum can also lead to the formation of a chronic perforation of the nasal septum. Small perforations may be asymptomatic; however, larger perforations can lead to recurrent epistaxis in addition to audible whistling, difficulty breathing or pain. For patients with noted septal deformities, referral to an ENT specialist is recommended to review if septal surgery is needed.
{kind=link}
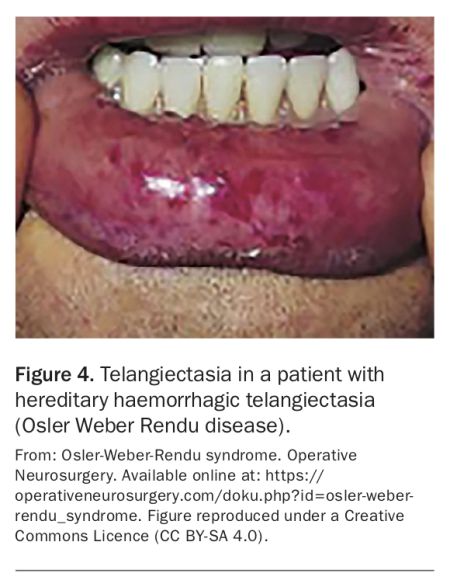
Finally, epistaxis can be a symptom of an underlying systemic coagulation disorder. This is especially important to consider in young patients with no clearly identifiable cause of bleeding or history of nasal trauma. Hereditary haemorrhagic telangiectasia (HHT or Osler Weber Rendu disease) in particular is strongly linked with epistaxis, with recurrent epistaxis occurring in up to 90% of affected individuals. Many of these patients will require definitive surgical or interventional therapy for recurrent bleeding. In patients with suspected HHT, the skin and other mucosal surfaces should be examined for the presence of telangiectasia (small vascular malformations) (Figure 4). The patient should also be examined for any evidence of systemic coagulation disorders, such as unexplained bruising, with blood tests checking for haemoglobin and coagulation profiles often useful in aiding the diagnostic workup. Medication use should be rationalised and a history taken for anticoagulant and antiplatelet use or the regular use of any supplements with an anticoagulant effect (e.g. fish oil or ginkgo). Concurrent occult bleeding, such as from a gastrointestinal source, should be suspected in patients with a substantial haemoglobin drop not fully explained by the nature and volume of epistaxis.
{kind=link}
Management
Cauterisation
When a clear and accessible bleeding point is identified, chemical cautery of the nasal mucosa or vessels using a silver nitrate applicator may be attempted. Direct visualisation can be optimised using a Thudicum speculum, a good light source and suction. Silver nitrate is then applied to the bleeding point or superficial feeding vessels to create a chemical burn. Excess silver nitrate should be removed to prevent injury to the surrounding tissue.
In cases of bilateral bleeding from Little’s area, avoid simultaneous cautery of both sites as this risks significantly compromising the septum and causing a septal perforation. Similarly, in patients who have recently had cautery to Little’s area, avoid repeat cautery or cautery to the contralateral side in the proceeding weeks until the mucosa has healed. After cauterisation, advise patients to use a nasal moisturiser or an antibiotic ointment until the surface has healed.
Reversal of systemic factors
For patients with systemic factors contributing towards epistaxis, reversal should be considered where possible. Given the large number of patients in the community on antiplatelet and anticoagulant agents for stroke and thrombosis prophylaxis, due consideration should be made towards reversing or withholding these agents where possible in recurrent epistaxis. For patients with high thrombotic risk, this decision should be made in consultation with their prescribing specialist. Additionally, patients with an underlying bleeding disorder should be managed in consultation with a haematologist for medical optimisation.
Nasal packing
In situations where no bleeding point amenable to cautery is identified, cautery is unsuccessful or diffuse mucosal bleeding occurs, the nose should be packed to offer direct pressure for tamponade of ongoing bleeding. Several techniques and devices have been developed to aid with nasal packing depending on availability and the suspected site of bleeding. Effective nasal packing has a success rate in controlling epistaxis of up to 70%, and the reported rate of complications, including nasal mucosa scarring, iatrogenic sinusitis and stimulation of the nasopulmonary reflex from posterior packs causing cardiac arrhythmia, varies between 2 and 70%.4
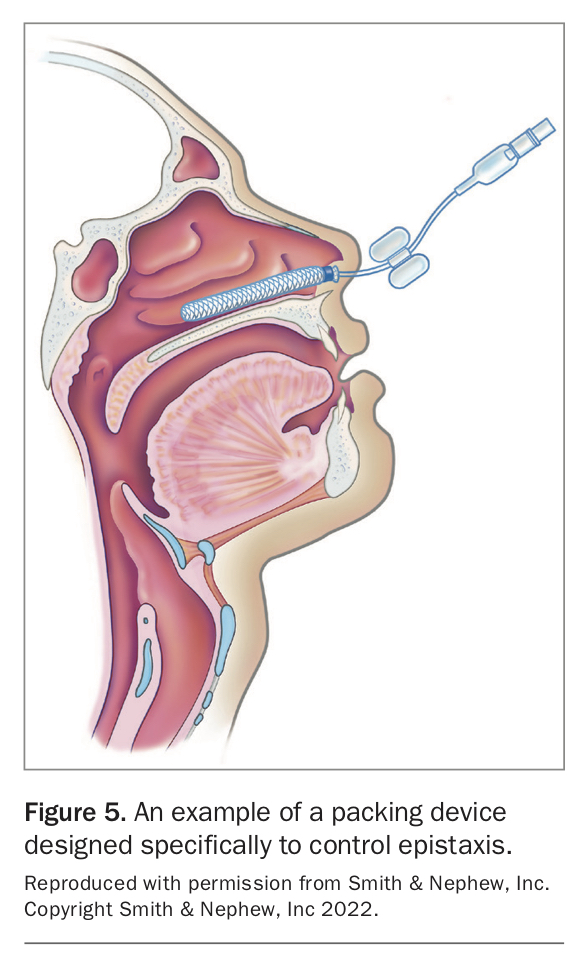
Commercial packing devices designed specifically to control epistaxis are available and consist of an inflatable balloon coated with a haemostatic agent (carboxymethyl cellulose) (Figure 5). Once moistened, the device can be inserted through the nose along the nasal floor and inflated with air to offer direct pressure over the suspected point of bleeding. Several variations in model exist, with separate or different length balloons designed to inflate over the anterior, posterior or both sections of the nasal cavity and the choice of device should depend on the location of suspected bleeding. Special care should be taken to ensure the balloon is fully inserted with only the butterfly guard and cuff remaining outside the nostril and taped gently to the side of the face without pressure on the nasal alar to avoid the risk of pressure necrosis.
{kind=link}
Prophylactic antibiotics have traditionally been recommended for patients with nasal packs in situ to prevent toxic shock syndrome. However, contemporary studies suggest the evidence for routine prophylactic antibiotic use for this purpose is poor.5
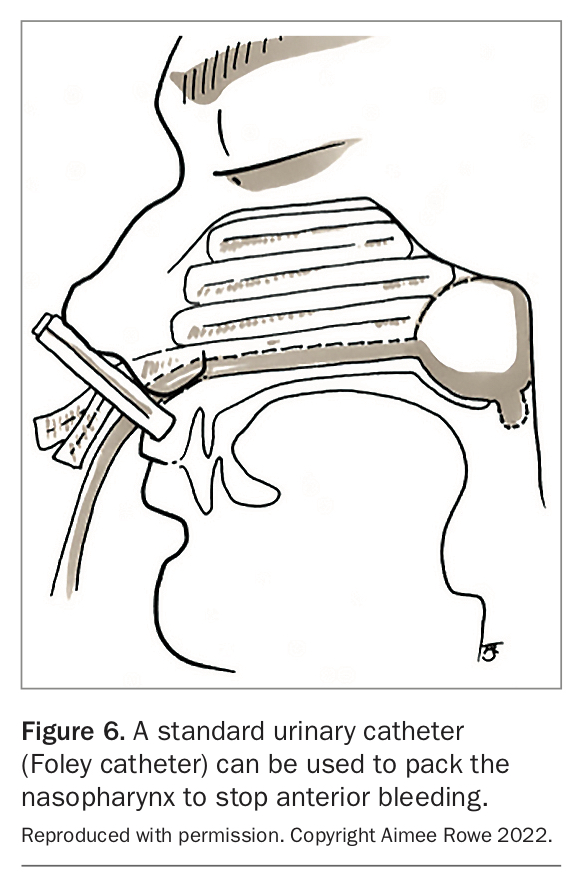
When an epistaxis-specific device is unavailable or when more anterior packing is unsuccessful in stopping postnasal bleeding, a standard urinary catheter (Foley catheter) may be used. The catheter can be passed through the nostril until the tip is visible in the back of the mouth. It is then inflated with water and pulled forward to sit in the nasopharynx. The nose can then be packed anteriorly with ribbon gauze and the catheter secured in position anteriorly using a clamp (Figure 6). Similar to commercial packing products, care should be taken to ensure the catheter and clamp do not cause pressure to the nasal alar and tip.
{kind=link}
In addition to these two methods, a number of absorbable and non-absorbable haemostatic devices are available for nasal packing, with the use and application of these products best guided by an ENT specialist.
Surgery
For bleeding that cannot be managed with nasal packing alone, or when bleeding is persistent after pack removal, an ENT specialist should be involved to assess whether surgical intervention is needed. Although most surgery for epistaxis is performed under general anaesthesia, for patients with significant comorbidities some methods can be attempted under local anaesthesia and sedation.
Surgical control of epistaxis begins with a thorough examination under anaesthesia of the nasal septum and cavity aided by a nasal endoscope and suction device. The improved access in this situation can often aid in identifying a clear bleeding point, and if seen, cautery using a powered device can be attempted.
When epistaxis cannot be resolved by cautery alone, ligation of the feeding artery can be attempted. The most common target for endoscopic ligation is the sphenopalatine, which supplies up to 90% of the blood supply to the nasal cavity, and is up to 89% effective at controlling bleeding when successfully ligated.3 Other potential targets for ligation include the anterior ethmoidal artery and internal maxillary artery. Historically, the external carotid artery has been a target for ligation; however, it is less so with improvements in endoscopic techniques. Nevertheless, it remains a final-line option for managing difficult to control epistaxis.
Although these procedures are definitive in most cases, patients should be informed that, if unsuccessful, further intervention via angioembolisation may be needed. Additionally, surgery carries a risk of injury to the nasopalatine nerve that runs closely to the artery, and can result in palatal numbness.
Angioembolisation
In patients whose epistaxis is not controlled by surgery alone, or who have contraindications for surgery, angioembolisation offers an alternative method for controlling bleeding. The nasal vascular system is accessed peripherally, classically via the femoral artery, under radiographic guidance, with contrast used to identify the bleeding point. The feeding vessels can then be ablated to offer targeted haemostasis. Although the reported success rate of this technique is high, it carries a risk of major complications, including stroke, blindness and tissue necrosis.6 Additionally, as it is a specialised procedure, trained proceduralists are not available at all centres and the procedure may be inappropriate for patients unable to tolerate a large contrast load, such as those in renal failure.
Medical management
Managing the underlying medical risk factors behind epistaxis is an important consideration that should not be neglected. If not contraindicated, systemic adjuncts such as tranexamic acid can be safely given to support control of epistaxis. Local vasoconstrictive agents such as xylometazoline spray can also be given for three to five days to reduce the risk of re-bleeding, but the patient should be advised not to use these sprays long term to reduce the risk of rhinitis medicamentosa. After any intervention, the patient should be advised to avoid aggressive nose blowing and sneezing, strenuous physical exertion and insertion of foreign bodies into the nose as these can all lead to recurrence of bleeding. Additionally, the use of topical agents, such as a sesame seed oil nasal spray or petroleum jelly, to the front of the nose after any procedure should be encouraged to protect from dryness and further decrease the risk of bleeding.
Conclusion
When faced with a presentation of epistaxis, establishing the location and severity of bleeding is important to best guide management and intervention. Recognising ‘red flag’ symptoms early in assessment can raise suspicion for more sinister causes of bleeding that require specialist review. By following a methodical stepwise approach, care can be escalated via first aid, the use of topical agents or cautery, nasal packing and surgical or interventional treatments as needed. Aftercare for high-risk patients is important and can help reduce the risk re-bleeding. MT
COMPETING INTERESTS: None.