Unilateral nasal polyps and other sinonasal lesions: benign or malignant?

Unilateral sinonasal lesions are more likely to be malignant or premalignant than bilateral disease and warrant careful evaluation. GPs play an important role in identifying unilateral disease, initiating management, ordering investigations and arranging specialist review.
Sinonasal polyps are common benign inflammatory lesions that can be single or multiple. Unilateral sinonasal polyps and other unilateral lesions, whether polypoid or solid, should raise significant clinical concern as they are more likely to be malignant or premalignant compared with bilateral disease. Indeed, many clinicians advocate that all unilateral sinonasal masses be considered neoplastic until proven otherwise. This article discusses the differential diagnosis of unilateral sinonasal lesions, including polyps, and presents a framework for GPs to assess and manage patients who present with unilateral sinonasal lesions.
Presentation
The symptoms of unilateral sinonasal lesions can include:
- unilateral nasal obstruction
- congestion
- partial or complete loss of the sense of smell (hyposmia)
- rhinorrhoea
- postnasal drip
- headaches
- snoring.
Epistaxis, orbital symptoms, epiphora (excessive tearing), facial pain, swelling, numbness or a neck mass in the setting of a unilateral nasal lesion are red flag symptoms and signs that should raise suspicion for sinonasal malignancy. This tends to have an insidious course and may cause symptoms only when advanced, due to local invasion.
A recommended stepwise approach to assessing and managing patients with unilateral nasal lesions, including when to refer, is shown in the Flowchart. Referral to an otolaryngologist is essential for all patients with unilateral nasal masses, for nasoendoscopy and often tissue diagnosis.
Examination
The anterior to midnasal passages can be examined with an otoscope and otic speculum. A headlight and nasal speculum, if available, will provide a superior view. Examination begins by gently elevating the tip of the nose to look into the anterior nares. Attention should be paid to the appearance of the mucosa over the nasal septum and inferior turbinates. Normal mucosa is moist and a healthy pink colour, without oedema. Allergy may cause the mucosa to take on a dull, ‘boggy’ appearance. In acute or chronic rhinosinusitis, the mucosa may appear hyperaemic.
The normal structures of the anterior nasal cavity should be distinguished from polyps and other lesions, as follows.
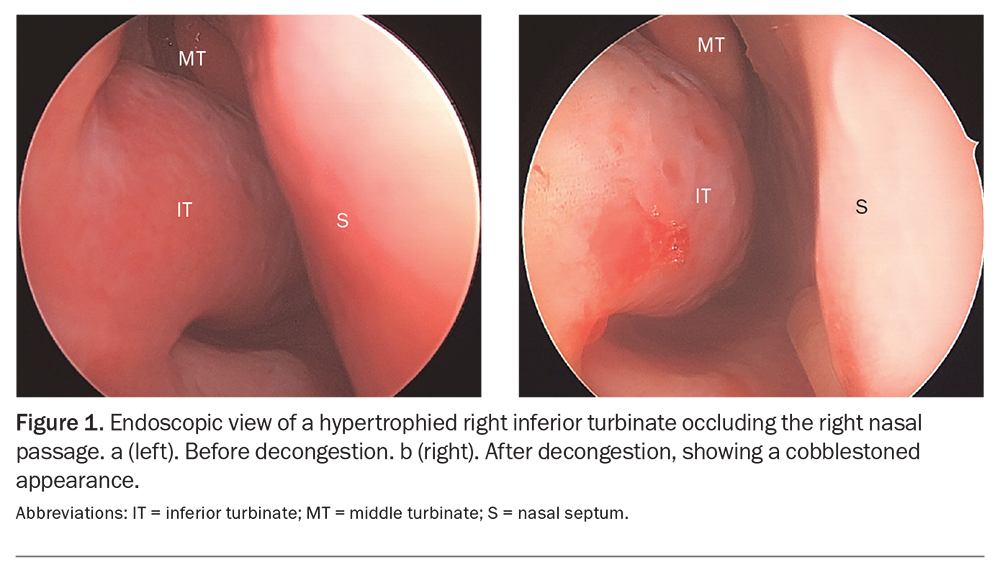
Inferior turbinates
The inferior turbinates arise from the lateral nasal wall and run parallel to the floor of the nose. They can be enlarged because of thick underlying bone or mucosal hypertrophy secondary to allergic or nonallergic rhinitis. Unilateral inferior turbinate enlargement can occur with septal deviation, on the contralateral side to the deviation (i.e. in the more patent nasal cavity).
An enlarged inferior turbinate is often mistaken for a nasal polyp or lesion. Application of an anaesthetic and vasoconstrictor spray, followed by careful examination with an otic or nasal speculum, can help distinguish the two. A hypertrophied inferior turbinate will generally decongest well and be found to be in continuity with the remainder of the inferior turbinate (Figure 1).
{kind=link}
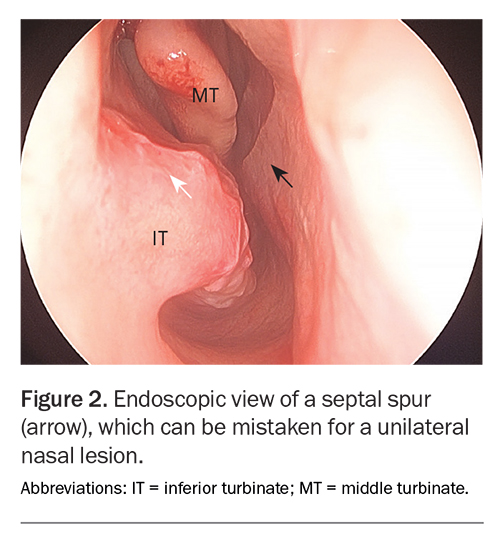
Nasal septum
The nasal septum divides the nasal cavities. The most common septal pathology is deviation, which can be mistaken for a unilateral nasal lesion, particularly when it is anterior. This can be avoided by using the speculum to examine above and below the deflection, as well as examining the contralateral side for a corresponding deformity (Figure 2).
{kind=link}
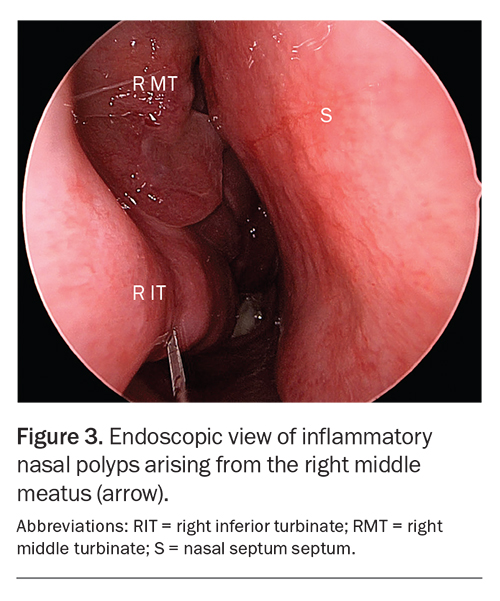
Middle turbinate
The head of the middle turbinate may just come into view on anterior rhinoscopy. The space lateral to the middle turbinate and superior to the inferior turbinate is the middle meatus, which contains the common drainage pathway of the maxillary, anterior ethmoid and frontal sinuses. Nasal polyps often protrude from here as pale, smooth, translucent, round or pear-shaped lesions (Figure 3).1 They have a gelatinous consistency and are insensate to probing. Occasionally, large nasal polyps fully occlude the nasal passage.
{kind=link}
Imaging
All patients who present with unilateral nasal lesions should undergo imaging as part of the workup. Noncontrast CT of the sinuses is the preferred initial imaging modality. The presence of bony erosion on CT suggests malignancy and should prompt urgent otolaryngology review. In the absence of bony erosion, distinguishing between inflammatory and neoplastic lesions on history taking, examination and CT can be difficult, making otolaryngology referral for tissue biopsy essential.2
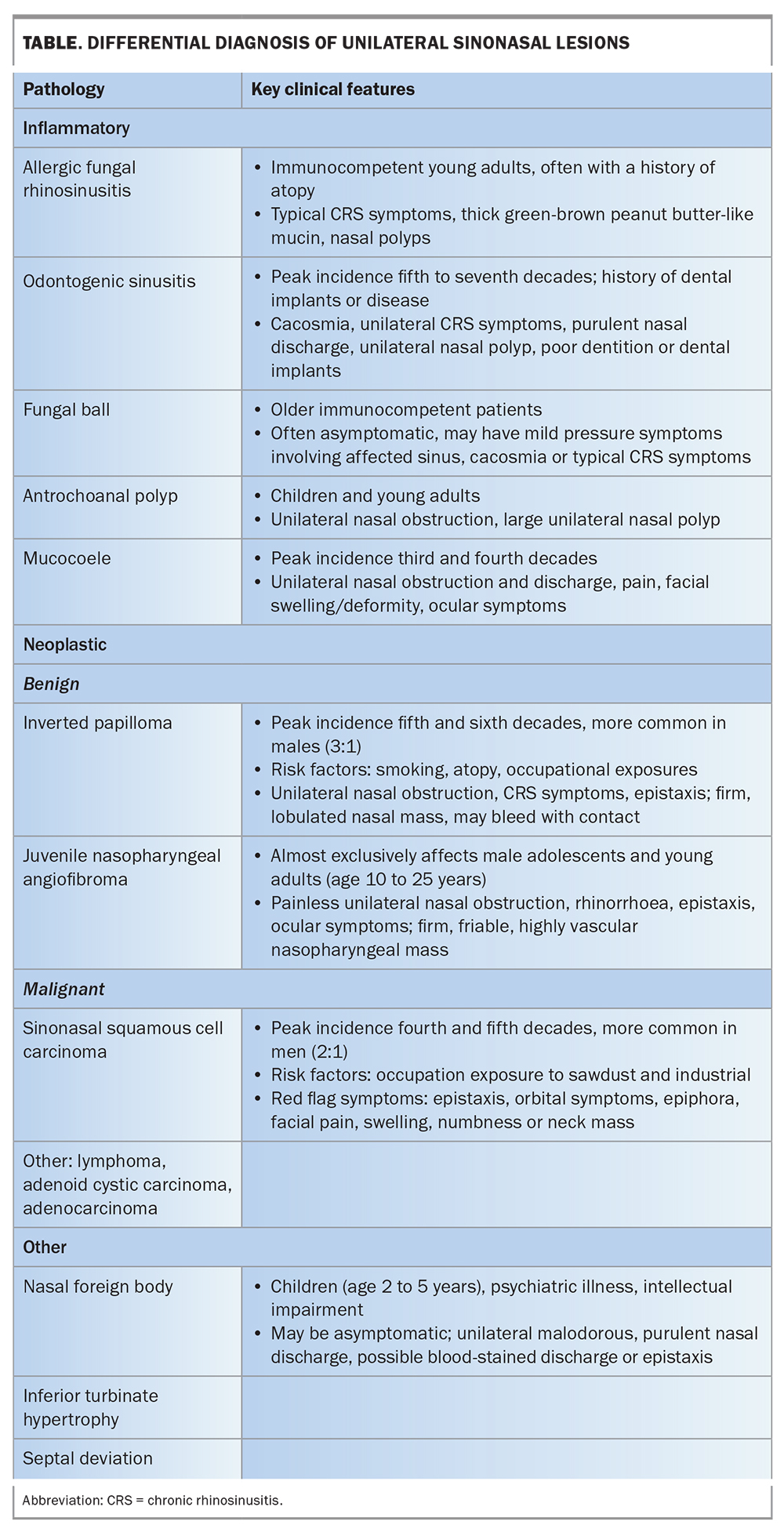
Differential diagnosis of unilateral sinonasal lesions
The differential diagnosis of unilateral sinonasal lesions is shown in the Table.
{kind=link}
Inflammatory polyps
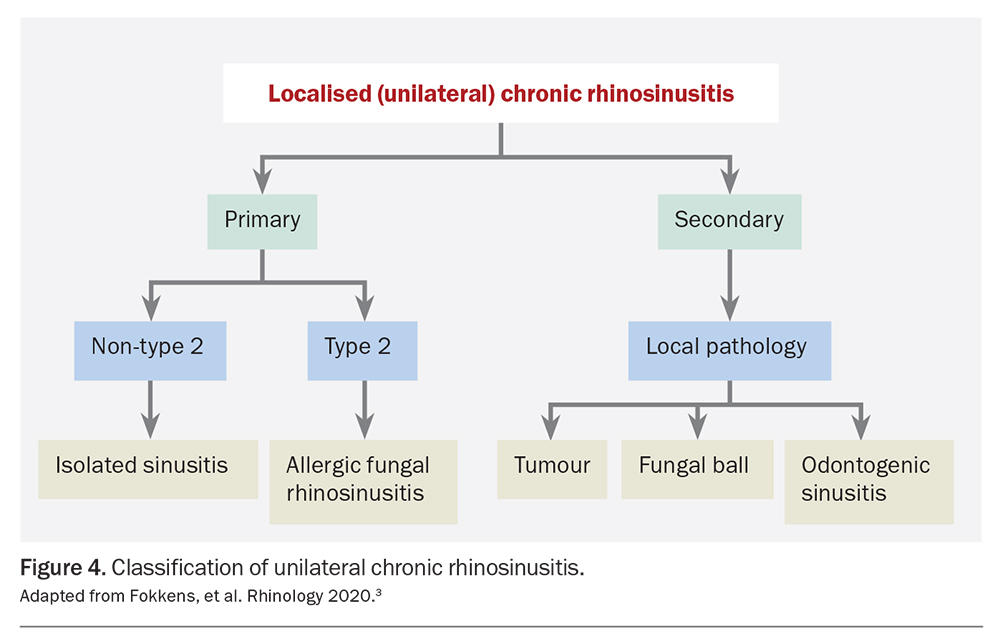
Inflammatory nasal polyps are benign lesions emanating from the nasal or paranasal sinus mucosa. They are found in about 2 to 4% of the population. Inflammatory nasal polyps account for most sinonasal lesions and most commonly arise in the setting of chronic rhinosinusitis, a heterogeneous group of inflammatory sinonasal disorders. Although many subtypes of chronic rhinosinusitis are bilateral, involving multiple sinuses, localised subtypes can cause unilateral sinonasal disease and unilateral nasal polyps. These subtypes include allergic fungal rhinosinusitis, odontogenic sinusitis and fungal mycetomas (Figure 4).3
{kind=link}
Allergic fungal rhinosinusitis
Allergic fungal rhinosinusitis accounts for 5 to 10% of cases of chronic rhinosinusitis. In allergic fungal rhinosinusitis, an eosinophil-driven type 2 inflammatory response occurs, characterised by inappropriate activation of T helper 2 cells, which produce type 2 cytokines that play several roles in the inflammation cascade. This response is targeted towards inhaled fungi, which ordinarily form part of the sinonasal microbiome. Allergic fungal rhinosinusitis typically affects immunocompetent young adults, who present with unilateral chronic rhinosinusitis symptoms.
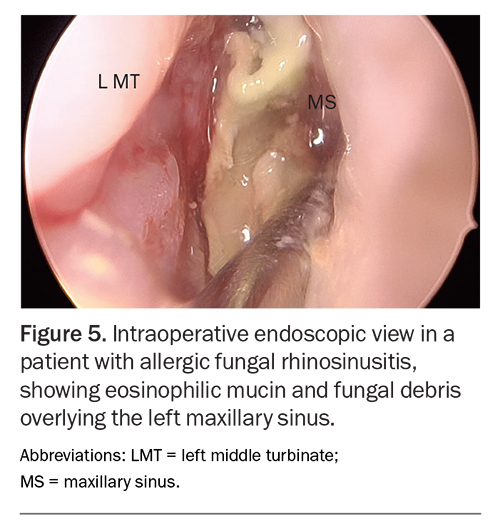
Patients often report a history of atopy and may have a high serum IgE level and type I IgE hypersensitivity to fungi and other aeroallergens. Examination may reveal a unilateral nasal polyp and thick, green-brown, peanut butter-like eosinophilic mucin (Figure 5).4 CT of the sinuses shows opacification of affected sinuses with densely packed hyperdensities. The bony walls may be expanded or thinned. Bony erosion (a feature typically associated with malignancy) can occur, caused by pressure from expanding polyps.3,6,7
{kind=link}
Medical therapy alone is generally insufficient to treat allergic fungal rhinosinusitis, and complete surgical debridement of all fungal elements and eosinophilic mucin within the sinus remains the mainstay of treatment.4 Preoperative oral corticosteroids may be beneficial in reducing inflammation, resulting in polyp and symptom regression as well as improved visibility intraoperatively.3 Topical intranasal corticosteroids delivered by nasal irrigation or nebulisation have been proposed to prevent recurrence after surgery.8
Odontogenic sinusitis
Odontogenic sinusitis is a form of chronic rhinosinusitis that affects the maxillary sinus secondary to underlying dental pathology, trauma or instrumentation. It peaks in incidence in the fifth to seventh decades and is slightly more common in women than men. An increase in observed cases in recent years has been attributed to a rise in dental procedures and the use of dental implants.
Patients with odontogenic sinusitis typically present with unilateral chronic rhinosinusitis symptoms, with cacosmia (unpleasant smell) strongly suggesting an odontogenic cause. Dental pain is present in only about a third of patients. It is essential to note any history of dental procedures or implants (even if many years before) and to examine the oral cavity and dentition.
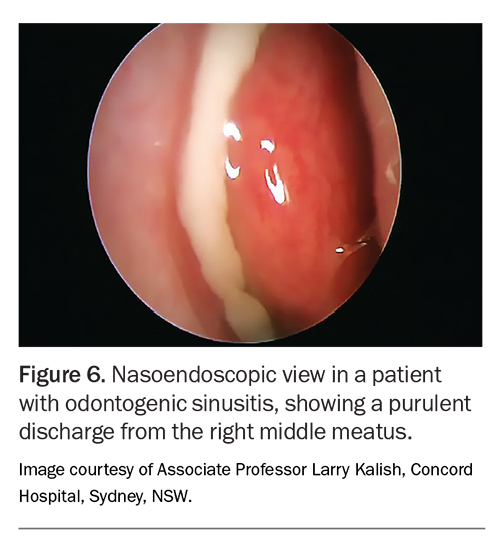
Examination findings include a purulent discharge from the middle meatus and mucosal oedema (Figure 6). A unilateral nasal polyp may be seen. Unilateral maxillary sinus opacification is the most common CT finding, and periapical lucencies strongly suggest an odontogenic cause.
{kind=link}
Multimodal therapy is required. Antimicrobials can alleviate symptoms, with penicillin beta-lactamase inhibitor combinations and quinolones being most effective. Intranasal corticosteroids can also provide symptom relief. Dental and ear, nose and throat referral are necessary for definitive treatment. Root canal procedures or tooth extraction provide source control, and endoscopic sinus surgery clears infection from the sinus, widens the sinus ostium for improved drainage and, in some cases, addresses dental disease via the maxillary sinus.9
Fungal mycetoma
A sinus fungal mycetoma or fungal ball is a slow-growing, noninvasive collection of fungal hyphae, usually in a single sinus cavity. Aspergillus spp. are the most common pathogen. Fungal mycetomas tend to occur in older, immunocompetent patients and are often asymptomatic, detected incidentally. Occasionally, mild pressure symptoms of the affected sinus, cacosmia or obstructive symptoms may arise.
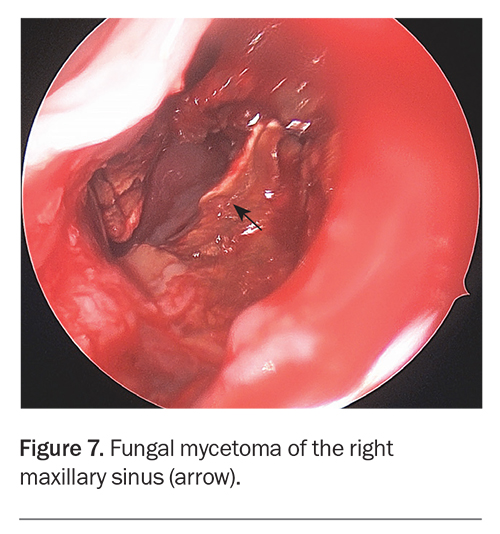
CT shows a high-density, heterogeneously enhancing mass within the sinus, with surrounding hyperostosis (thickened bone) consistent with chronic inflammation (Figure 7). The appearance on anterior rhinoscopy is often unremarkable. There may be mucosal oedema or polyposis around the middle meatus when the maxillary sinus is affected.
{kind=link}
Treatment is purely surgical, with removal of the mycetoma and washout of the sinus cavity.10
Antrochoanal polyps
Antrochoanal polyps are benign, usually solitary, unilateral nasal polyps. They arise from the maxillary antrum and extend to the choanae, and can grow large enough to fill the nasopharynx. Antrochoanal polyps are most commonly found in children and young adults. They account for about 4 to 6% of all nasal polyps in the general population, and up to 35% of all nasal polyps in the paediatric population.11
The most common presenting symptom of antrochoanal polyps is unilateral nasal obstruction, particularly on expiration. CT reveals a unilateral hypoattenuating mass of the maxillary sinus that extends through the middle meatus and posteriorly towards the choana.
Surgical management is required to remove the polyp, open the maxillary sinus and resect the intramaxillary component, without which recurrence is common.12
Mucocoele
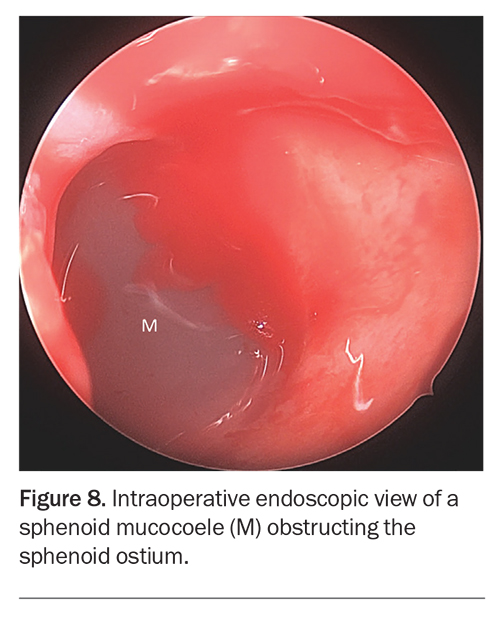
Paranasal sinus mucocoeles are benign, cystic, expansile lesions that share the same secretory respiratory epithelial lining of the sinuses.14 They arise due to sinus ostium obstruction, usually secondary to inflammation, allergy or postoperative scarring, resulting in mucus accumulation and pressure expansion within the sinus. Mucocoeles can occur at any age, peaking in the third and fourth decades. The frontal and ethmoidal sinuses are most commonly affected, although up to 10% arise from the maxillary sinus.
Symptoms of a mucocoele include nasal obstruction, facial pain and facial swelling or deformity. In the case of a maxillary sinus mucocoele, a mass obstructing the middle meatus may be seen with unilateral mucopurulent discharge (Figure 8). Frontoethmoidal and sphenoid mucocoeles may present with ocular complications from mass effect on the orbit, optic nerve or third, fourth, fifth and sixth cranial nerves. CT shows an expanded, airless, homogeneously opacified sinus with thinning or erosion of the bony walls.
{kind=link}
Surgical excision is required to relieve obstruction and restore normal sinus drainage.15 Early diagnosis and treatment are important in the case of frontoethmoidal and sphenoid mucocoeles to prevent visual compromise and other sequelae.
Benign neoplasms
Inverted papilloma
Inverted papillomas are benign epithelial tumours of the sinonasal mucosa and account for 0.4 to 7% of all sinonasal tumours.17 Their behaviour can vary from indolent growth to aggressive, infiltrative lesions with multiple recurrences and malignant transformation; 1.9 to 27% of inverted papillomas become squamous cell carcinoma.18-21 Risk factors for inverted papilloma include smoking, atopy and certain occupational exposures. Human papilloma virus has also been implicated in their pathogenesis.22 Men are more commonly affected (3:1 male to female ratio), and their peak incidence is in the fifth and sixth decades of life.10
Patients with inverted papilloma typically present with unilateral nasal obstruction and chronic rhinosinusitis symptoms. Epistaxis may occur. Anterior rhinoscopy may show a lobulated, raspberry-like nasal mass. Inverted papillomas typically arise from the lateral nasal wall and extend through the maxillary antrum. On probing, inverted papillomas are firmer and more friable than simple inflammatory nasal polyps, and may bleed with contact.17,23
CT of the sinuses shows a homogeneous lesion generally centred on the middle meatus. Bone erosion is often seen, with more aggressive destruction observed with synchronous carcinoma. MR imaging is routinely performed in patients with suspected inverted papilloma, with its improved soft tissue definition enabling better differentiation of inverted papilloma from inflammatory phenomena.
Treatment of inverted papilloma is surgical and requires complete excision of the lesion and reaming of the underlying bone.23 Preoperative antibiotics and corticosteroids may be used for symptom relief and to reduce intraoperative inflammation and bleeding.20 Recurrence is not uncommon and importantly can occur several years after surgery, warranting prolonged follow up.
Juvenile nasopharyngeal angiofibroma
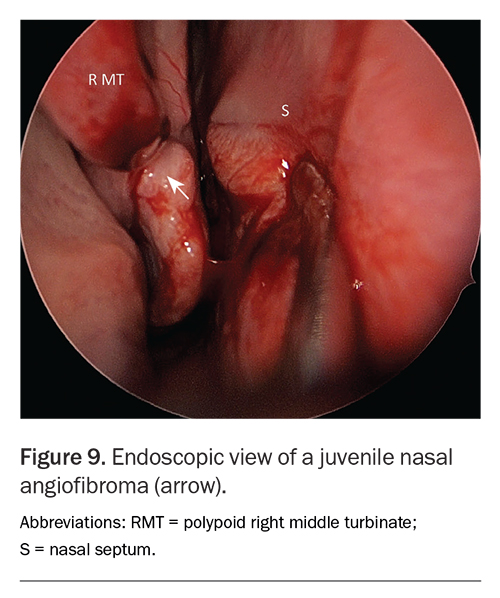
Juvenile nasopharyngeal angiofibromas are rare benign neoplasms predominantly affecting adolescent boys. Although benign, they are locally aggressive and can erode through the skull base or orbit. Presentation is usually with painless, progressive unilateral nasal obstruction. Rhinorrhoea, epistaxis, Eustachian tube dysfunction and ocular symptoms may occur.
On examination, a blue-tinged, firm, friable mass may be seen in the nose (Figure 9). CT shows a heterogeneous, lobulated mass with bone remodelling or resorption. MR imaging is useful for evaluating tissue extension. Treatment is by surgical excision, usually with preoperative angioembolisation, given the vascularity of these lesions.24
{kind=link}
Malignant neoplasms
Sinonasal malignancies account for 3 to 5% of head and neck malignancies, and over 70% of these are sinonasal squamous cell carcinoma (SNSCC). SNSCC most commonly arises in the fourth and fifth decades of life, with a male to female ratio of about 2:1. Risk factors include occupational exposure to sawdust and other industrial chemicals and human papillomavirus infection.26
The presence of epistaxis, orbital symptoms, epiphora, facial pain, swelling, numbness or a neck mass should raise alarm for malignancy. Malignant lesions are characterised radiologically by aggressive soft tissue masses that invade into the adjacent bony walls.
Management of SNSCC depends on the stage and the patient's surgical fitness and comorbidities. Surgical resection with postoperative radiotherapy appears to be the optimal treatment, with endoscopic approaches increasingly being used. Despite this, prognosis remains poor (around 50% survival at five years).27
Conclusion
Unilateral sinonasal lesions require careful evaluation to differentiate benign from aggressive processes. Evaluation of the patient with a unilateral nasal lesion involves a thorough history and examination together with CT. Referral to an otolaryngologist is essential for all patients with unilateral nasal masses, for nasoendoscopy and tissue diagnosis. MT
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.