Rhinoplasty: an illustrated overview

Rhinoplasty is a technically challenging procedure that can address both functional and cosmetic complaints. It can be performed by a closed or open (external) approach, the latter providing wide access for restructuring.
The Greek origins of the term rhinoplasty (‘rhino’, nose; and ‘plastos’, mould) help describe the surgical process of altering the form and function of the nose. Colloquially known as a ‘nose job’, rhinoplasty is increasing in popularity, fuelled by media and celebrity influences. The aesthetic aims of rhinoplasty are well known, but rhinoplasty can also be performed to improve function or for a combination of reasons.
The approach to rhinoplasty can be closed or open (external). In the external approach, the skin jacket is lifted and reflected off the nose via a small columella incision between the nostrils, providing access to the underlying bones and cartilage to enable restructuring. The formal name of this procedure, an external septorhinoplasty, acknowledges the key role of septal reconstruction.
This article outlines the indications for rhinoplasty, the different approaches, and their application in management of acute nasal injury and nasal obstruction. Key technical principles are discussed, along with the patient ‘journey’ and rhinoplasty after-care.
Indications for rhinoplasty
In functional rhinoplasty, the shape and structure of the nose are altered to improve the nasal airway and relieve obstruction. A patient with a visibly ‘crooked’ nose often has a bowed septum blocking one side, unsupported nostrils and a droopy nasal tip. Many patients report lifting up the tip with their thumb or ‘pulling out’ their nostrils to help them breathe. Functional rhinoplasty corrects these issues through a combination of surgical bone fractures (osteotomies), cartilage graft supports and septal reconstruction to unblock the nose.
Cosmetic rhinoplasty aims to achieve an aesthetic appearance of the nose that is balanced with the patient’s facial proportions without compromising function. Almost all patients seeking cosmetic rhinoplasty are women, and they often have specific concerns such as a hump, droopy tip or a broad nose. Most often these issues can be corrected, but in some cases the patient’s wishes are unrealistic considering their anatomical limitations, presenting another challenge for the surgeon.
Functional and cosmetic rhinoplasty may be combined, to improve nose shape and function in a single operation. Detailed examination, photography, computer imaging and discussion with the patient are essential before surgery to set realistic aesthetic and functional goals.
In revision rhinoplasty, the patient has had one or more previous rhinoplasty or septoplasty procedures. Revision rhinoplasty is performed to address the patient’s cosmetic and functional needs but requires cartilage graft material, which is often not available after multiple operations. Therefore, cartilage grafts from the ear or rib are used to reconstruct the nose.
Contraindications to rhinoplasty
In patients seeking cosmetic rhinoplasty, body dysmorphic disorder is a particular consideration.1 A low threshold for psychologist assessment is advised, as patients with body dysmorphic disorder are rarely satisfied, even by a good surgical outcome. Smoking is considered a relative contraindication to rhinoplasty as nicotine causes vasoconstriction, which reduces blood flow to the skin and impairs healing.
Management of acute nasal bone fracture
The nasal bones are the most common facial bones to fracture, and injury often results in swelling, epistaxis and nasal deformity. In patients with a nasal bone fracture, it is important to remember that other facial injuries may be present, and some of the sequelae are not evident on external examination.
Acute assessment and imaging
Patients with acute nasal bone fracture are usually assessed in the emergency department. The priority is to control epistaxis, examine for septal haematoma and assess for other facial injuries. Coincident midfacial injuries may require CT of the facial bones, but x-ray or CT is not necessary or useful in the context of an isolated nasal bone fracture, and the diagnosis is made clinically.
Ear, nose and throat review
Follow-up in an ear, nose and throat (ENT) clinic is needed, ideally five to seven days after the injury, to allow the initial swelling to subside. The nose can then be examined, and management organised where necessary.
Closed fracture reduction or rhinoplasty
When the nasal bones are fractured and acutely deviated after trauma, a closed reduction of the nasal bone fracture can be offered. The window for this procedure is 14 days from injury. A closed reduction addresses deviation of the bony upper third of the nose but does not correct deviation of the lower two-thirds of the nose or the septum. Patients with injuries outside of the 14-day window and those with post-traumatic deviation of the lower two-thirds of the nose or septum will require external septorhinoplasty to address these issues. Their surgery is scheduled electively, rather than emergently.
Management of the blocked nose
Patients presenting with nasal obstruction often complain that it affects their quality of life.2 Many inflammatory disorders of the nose and paranasal sinuses, such as nasal polyps and enlarged turbinates, can cause symptoms that include nasal obstruction. The most common structural factors contributing to a blocked nose are a deviated nasal septum or septal spur, internal nasal valve collapse (pinching of the middle third of nose) and external valve collapse (nostril collapse on inspiration). Often, patients have a combination of issues. As the degree of congestion in the nasal mucosa naturally changes from side to side roughly every four hours, along with the nasal cycle, patients can find it hard to identify a worse side.
Deviated nasal septum and septal spur
The nasal septum provides the central structural support to the nose and divides the nasal airway in the midline. A septal spur is an outcrop or shelf of bone or cartilage that arises from the septum. It narrows the nasal airway and contributes to the sensation of a blocked nose. A deviated septum has often been displaced by trauma or has grown into malposition (Figure 1). The septum frequently bows and tilts under the pressure of the surrounding tissues so that one side is convex and the other concave. The convex side typically blocks as it narrows the nasal airway.
{kind=link}
A simple septoplasty aims to address a deviated septum by removing a window from the bowed cartilage but must retain the cartilage supporting the nasal bridge and tip. Therefore, a significant bowed septal deviation, especially an anterior and high deviation, cannot be corrected by septoplasty alone. These patients require open reconstruction by external septorhinoplasty, to straighten the entire septum and support the nose.
Typically, the inferior turbinate on the concave side of the septum hypertrophies to occupy the space left by the concavity, and the inferior turbinate on the convex side is hypoplastic. An inferior turbinoplasty is routinely performed with a functional rhinoplasty to alleviate this obstruction.
Internal valve collapse
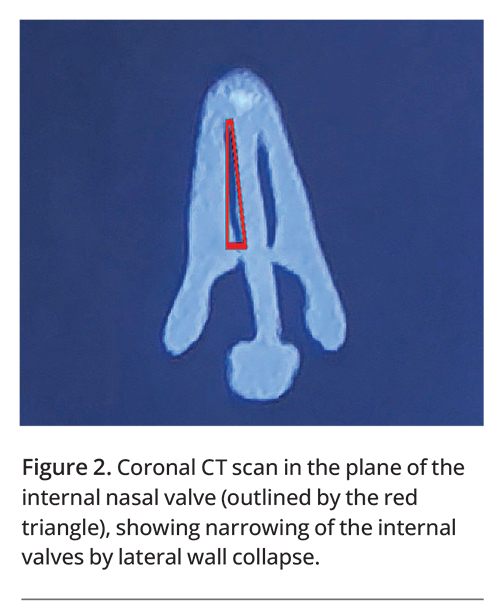
The triangle formed by the inferior turbinate, septum and lateral nasal wall represents the narrowest point of the nasal airway and is termed the internal nasal valve (Figure 2).3 The sensation of obstruction is caused by narrow dimensions at this point. It can be addressed only by manoeuvres involving graft placement to open the apex of this triangle and increase the cross-sectional area.
{kind=link}
External valve (nostril) collapse
Dynamic collapse of the nostril, known as the external nasal valve, can occur on inspiration in a deviated and unsupported nose.3 This change contributes to nasal obstruction (Figures 3a and b). It is remedied by structural cartilage grafts that support the nostril rim and prevent collapse on inspiration (Figure 3c).
{kind=link}
Technical principles of rhinoplasty
Open vs closed approach
A closed rhinoplasty is conducted through incisions inside the nose, allowing access to the nasal bridge. This approach is often used to correct a nasal hump. It has the disadvantages of limited exposure and limited ability to add structural support to the nose, which therefore cannot be corrected to the same extent.
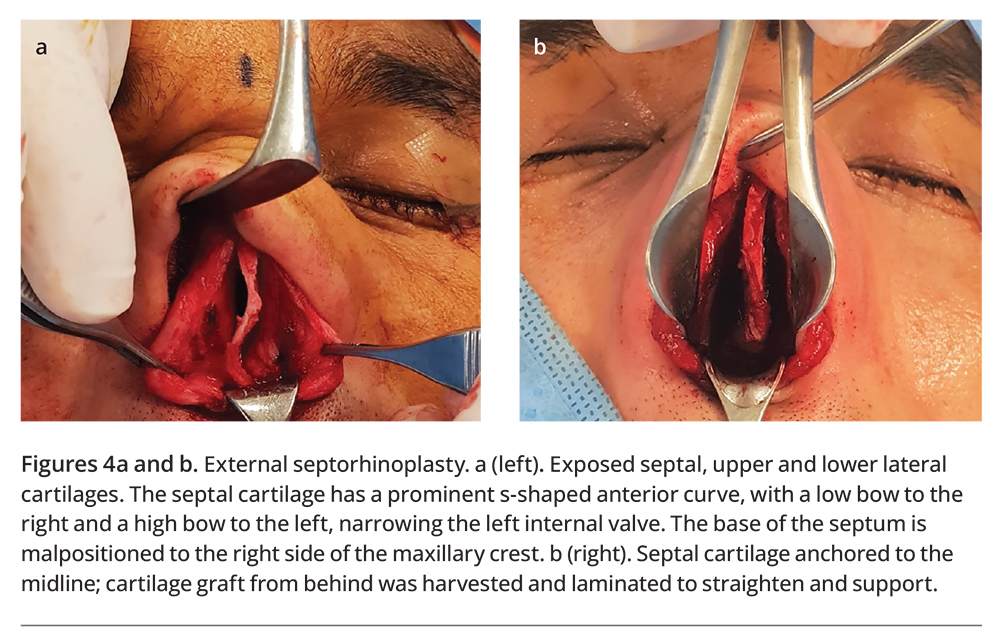
An open approach (external septorhinoplasty), through lifting and reflecting the skin jacket off the nose via a small incision in the columella, offers wide exposure of the lower and upper lateral cartilage, the cartilaginous and bony septum and nasal bones (Figure 4a). This enables the use of a wider variety of reconstructive techniques to restructure the nose.
{kind=link}
Graft material
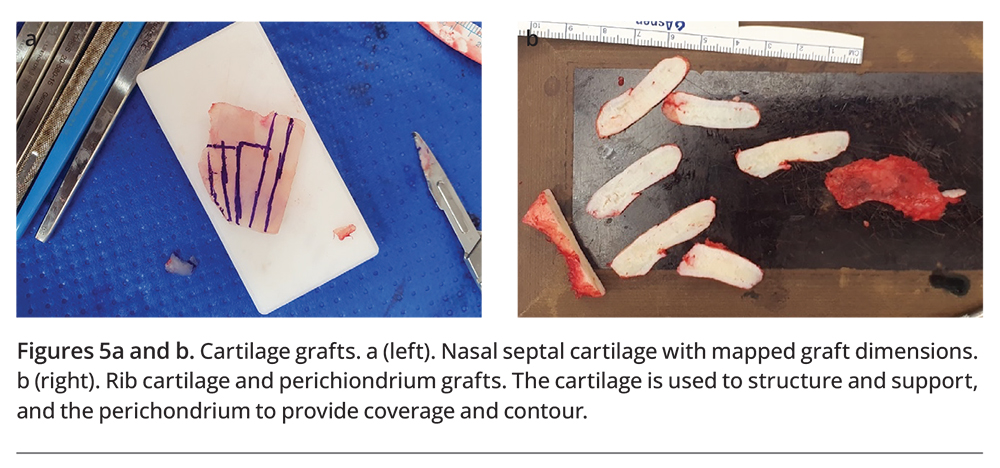
Septal cartilage is harvested, and the required graft dimensions are mapped onto the cartilage before the grafts are fashioned and placed (Figure 5a). Rib cartilage provides an alternative graft material for reconstruction and is often required in patients undergoing revision rhinoplasty (Figure 5b). Excess septal height can worsen the septal bow and tilt. This can be reduced at the time of cartilage harvesting to allow the base to be fixed in the midline (Figure 4b). With the septum now straight, it can be reinforced with cartilage grafts.
{kind=link}
Reconstruction
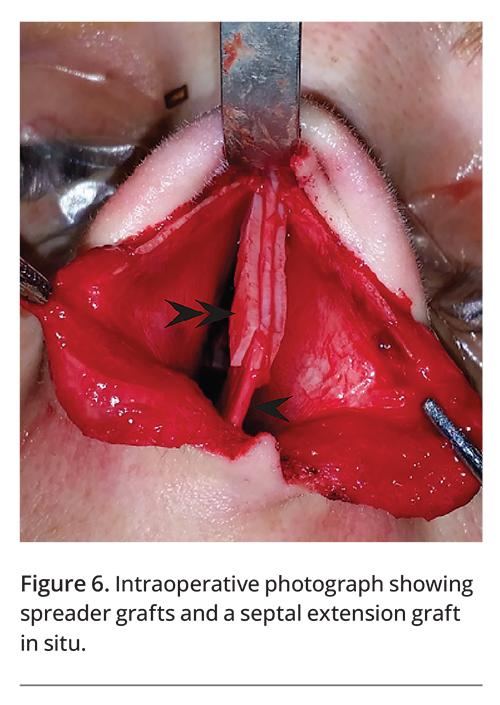
The internal nasal valve area can be increased by grafts placed from the nasal bridge to the tip (Figure 6). These ‘spreader’ grafts are sutured to the upper septum and support the bridge (middle vault), helping to keep the dorsum straight and preventing future deformity.3
{kind=link}
Reinforcement or extension of the anterior septal cartilage is often required to ensure the tip is supported and the nasal airway remains open. Septal extension or lamination grafts are used for this purpose and provide long-term support (Figure 6).4
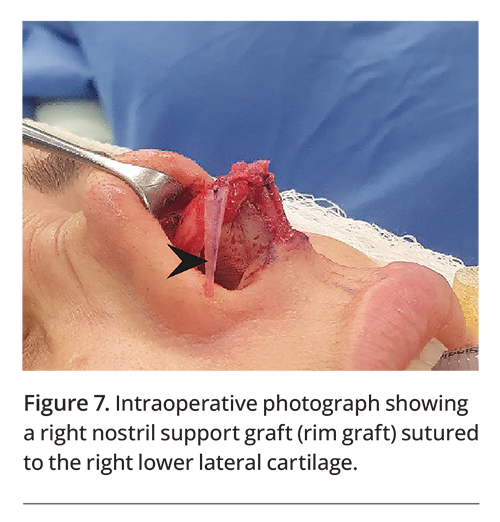
Nostril support grafts sutured to the lower lateral cartilages brace the external valve and prevent nostril collapse on inspiration (Figure 7).3 These ‘rim’ grafts have the added benefit of providing desirable nostril contouring.
{kind=link}
Bone fractures (osteotomies)
Sharp chisels (osteotomes) or ultrasonic tools are used to remove a nasal hump and to mobilise the bony structure of the nose through surgical fracture lines. The mobilised bones can be manipulated to narrow a broad nose and achieve a thinner front view. This step explains the postoperative periorbital bruising seen in patients who have undergone rhinoplasty.
Refinement
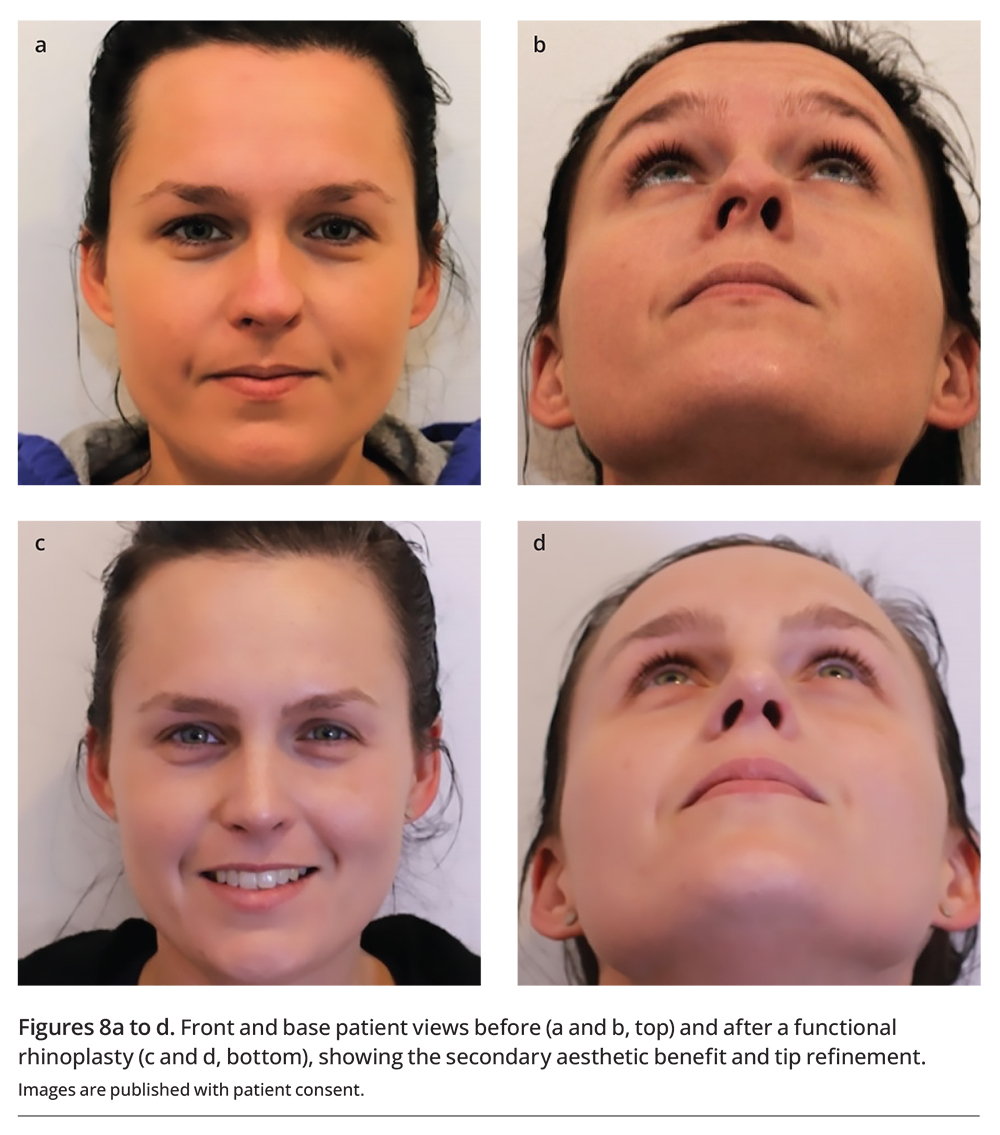
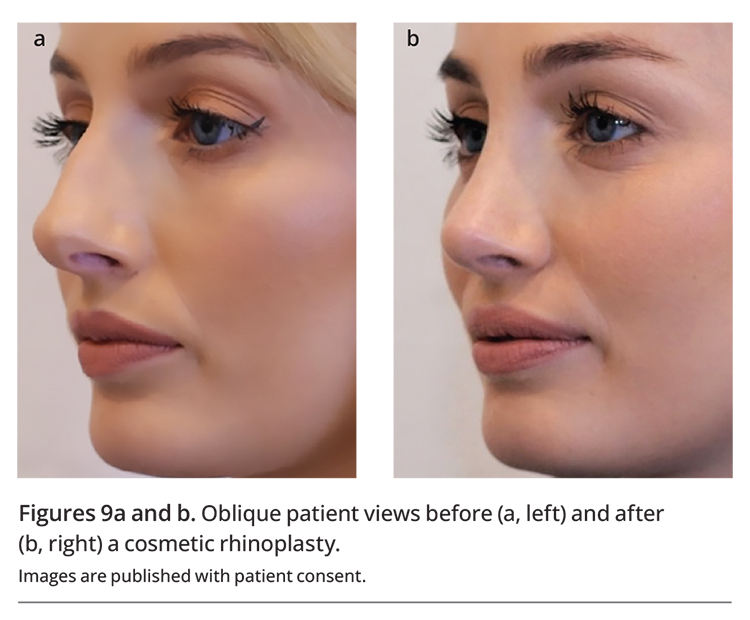
Functional rhinoplasty often achieves a more aesthetically appealing result by restoring the nasal form (Figures 8a to d). Aesthetic appearance is a key aim of cosmetic rhinoplasty; however, it is also imperative that the nasal structure is functional and supported to minimise the risks of future collapse and revision surgery. The many different techniques to refine the shape of the nose are beyond the scope of this article. An example of cosmetic rhinoplasty, nasal hump removal and tip and nostril refinement, is shown in Figures 9a and b.
{kind=link}
{kind=link}
After care and the patient journey
Rhinoplasty can be performed as day surgery, but some patients require an overnight hospital stay. Patients are discharged with a moulded splint taped onto their nose and internal nasal splints; both are usually removed one week after surgery. Patients are instructed to rinse the nose from postoperative day 1 and to complete a short course of oral antibiotic therapy.
Postoperative pain is typically mild and controlled by simple analgesia with the addition of mild opiates for the first week. Facial swelling and periorbital bruising are common if osteotomies have been performed. Bruising and swelling usually peak on postoperative day 3 and often subsides over the next seven days. The swelling can track with gravity to the cheeks and jowls.
Patients are instructed to take two weeks off work and exercise and are followed up closely over the first year after surgery. Postoperative corticosteroid injections can help nasal swelling subside more quickly and are used if required.
The outcome of the surgery can be assessed after a year, when all swelling has resolved and healing is complete.
Conclusion
External septorhinoplasty is a complex procedure that can address patients’ functional and aesthetic needs. This procedure requires thorough patient assessment, detailed planning and effective communication to ensure that patient expectations meet the anatomical and technical limitations of surgery. In some cases, psychological assessment is required to evaluate for body dysmorphic disorder. Close postoperative follow up is essential, and the result can be assessed when the swelling has completely subsided. MT
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.