Thunderstorm asthma. Forecasting and managing the impact in your practice
Asthma
Asthma in children
Thunderstorms can provoke asthma symptoms in patients with allergic sensitisation particularly during pollen season, imposing major burdens on health services at all levels. GPs play an important role in identifying and managing at-risk patients and preparing for thunderstorm asthma events and other environmental disasters.
- Thunderstorm asthma is potentially life-threatening.
- Almost all patients who experience thunderstorm asthma in Australia have allergic sensitisation to ryegrass pollen.
- Some people who experience thunderstorm asthma have not previously been diagnosed with asthma.
- People with a history of wheezing and hay fever who live in southeastern Australia should be considered at-risk for thunderstorm asthma. They should: – take regular inhaled corticosteroids during the spring and early summer – have, know and follow their asthma action plan – remain indoors with windows closed before and during thunderstorms.
- General practices should review procedures to follow in the event of a thunderstorm asthma event or other external emergency.
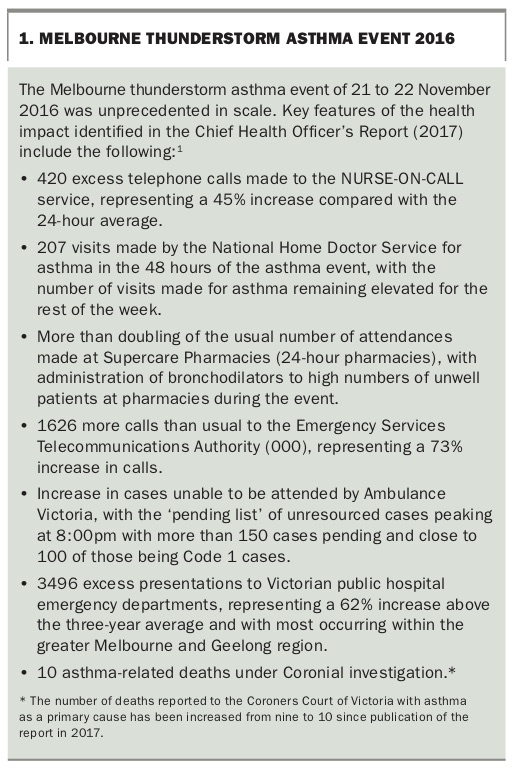
Thunderstorm asthma occurs when the interaction between aerobiological, environmental and meteorological conditions triggers the rapid onset of asthma symptoms in susceptible individuals. A key concern regarding thunderstorm asthma relates to the risk of health-related services becoming overwhelmed by the synchronous presentation of multiple patients with respiratory symptoms, which was observed in Melbourne during November 2016 (Box 1).1 Although further research is required to inform interventions directed at prevention and management, we present an overview of current knowledge including the potential role of GPs in the practical care of patients who experience thunderstorm asthma.
{kind=link}
Epidemiology
Thunderstorm asthma has been observed in many countries, including Australia, the UK, Italy, Canada and Iran.2-6 The spatial and temporal clustering of events reflects the importance of local environmental factors, even within Australia. Melbourne has experienced at least seven thunderstorm asthma events in the past 40 years,2,7-10 whereas Sydney has experienced none. Furthermore, although thunderstorm asthma in Australia appears almost entirely associated with ryegrass allergy, this is not a universal observation. For example, those affected by a thunderstorm asthma event in the UK were sensitised predominantly to the mould Alternaria species rather than to grass pollens.11 Identifying common features of the observed epidemics has allowed for postulation of underlying mechanisms, although the cause of geographical susceptibility remains unclear.12
Most thunderstorms are not associated with severe epidemics of asthma attacks. However, they may occur more commonly than recognised. For instance, a study in Melbourne suggested that in a population of about four million people, thunderstorms during days of high pollen count were associated with about three to five additional asthma-related hospitalisations.13 Furthermore, in a case-controlled study conducted using emergency department data from six towns on the western slopes of the Great Dividing Range in NSW, thunderstorm outflows were observed on 33% of asthma epidemic days, compared with only 3% of non-epidemic (control) days. When the analysis was restricted to the months of October to January (late spring and early summer), 48% of asthma epidemic days and 8% of control days, respectively, were associated with thunderstorm outflows.14 (Thunderstorm outflows are described in further detail in the following section.) Hence, although severe epidemics of thunderstorm asthma are uncommon, less severe episodes may be more common than previously recognised, particularly during late spring and early summer in the affected areas.
Mechanisms
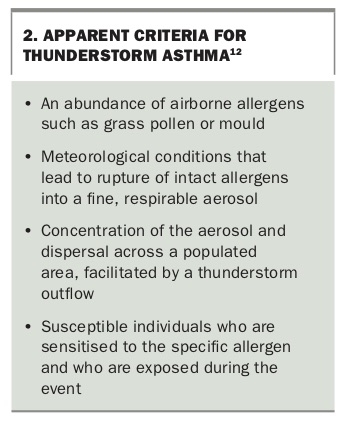
There are several apparently prerequisite conditions for thunderstorm asthma to occur (Box 2). The first criterion is elevation in concentrations of airborne allergens, the best example of this being pollen. Unlike flowers such as wattle, which attract birds and insects to assist pollination, grasses and other plants rely on windborne transfer of genetic material and are far more likely to contribute to the atmospheric pollen burden. Ryegrass, for instance, is an introduced species common in southeastern regions of Australia; one hectare of perennial ryegrass pasture may produce more than 400 kg of pollen per season.15 Ryegrass, implicated in almost all of Australia’s thunderstorm asthma epidemics, is the major contributor to the grass pollen burden in Melbourne. In contrast, Australia’s northern regions feature a separate peak in pollen concentrations during the year attributable to subtropical native grasses (e.g. indigenous Sorghum).16 Although grass pollens represent the major aerobiologically significant allergen at least in the Australian setting, there is substantial variation in the timing and severity of ‘pollen season’ depending on the typical flowering periods of prevalent culprit species.17
{kind=link}
The second and third criteria for thunderstorm asthma are meteorological conditions able to modify the allergen into a potent, respirable aerosol and facilitate rapid dispersal of this aerosol across a wide area. Multiple parameters such as wind speed, lightning, water (rain) and sudden changes in temperature and humidity have been associated with thunderstorm asthma; a combination or a change in these factors, particularly moisture, are implicated in promoting aerosol formation.18 Ryegrass pollen swells then ruptures on contact with water, releasing hundreds of paucimicronic starch granules able to reach the lower airways when inhaled.19 Evidence of bioaerosol formation is suggested by foreshadowing of thunderstorm asthma presentations by increases in the concentrations of ruptured pollen husks and broken fungal spores.11,14 During thunderstorm maturation, cooled air descends then concentrates this aerosol into an outflow which spreads outwards parallel to the ground, like a ripple from a dropped pebble in a pond. In this manner, thunderstorm outflows are implicated in distributing the allergenic bioaerosol across a wide geographical area.
The final criterion is the exposure of susceptible individuals to the specific allergen. Allergic sensitisation appears almost universal among patients affected by thunderstorm asthma. In southeastern Australia, ryegrass sensitisation is present in more than 95% of cases in comparison to about 60% of control subjects.2,20 In the 2016 Melbourne epidemic, all 81 patients who attended subsequent allergy testing tested positive to ryegrass on skin prick, serum-specific IgE assay or both.21 Hence, although individuals across a wide geographical area are exposed to a massive aeroallergen challenge, only those who are susceptible to this trigger generate an immune response with cough, wheeze and breathlessness. It remains unclear what other features confer susceptibility. Typically, many people affected by thunderstorm asthma deny a previous history of asthma, although some of these report previous episodes of wheeze.20 It seems likely that pre-existing susceptibility of the lower airway is a pre-condition for experiencing thunderstorm asthma. Although the exact nature of this susceptibility remains unclear, the risk seems to be mitigated by regular use of inhaled corticosteroids,20 so it may be related to eosinophilic inflammation and/or airway hyperresponsiveness.
As the thunderstorm outflow passes over a populated area, all people in its path are exposed. However, exposure can be reduced simply by remaining indoors with windows closed, which is associated with reduced odds of symptoms during a thunderstorm asthma event.20
It is worthwhile noting that even though air pollution is, in general, positively associated with exacerbations of asthma, there is conflicting evidence regarding the effect of air quality in contributing to thunderstorm asthma events.22
How can GPs help patients?
Identify high-risk individuals
Symptoms of seasonal allergic rhinitis (hay fever) are strongly associated with sensitisation to ryegrass pollen and, therefore, are a strong predictor of risk for thunderstorm asthma. Allergic rhinitis is a clinical manifestation of IgE-mediated allergic sensitisation. It occurs in almost one in five Australians and is observed in up to 90% of patients presenting during thunderstorm asthma events.20
The diagnosis of allergic rhinitis may be made on clinical grounds among patients who experience typical symptoms such as sneezing, rhinorrhoea and nasal congestion in response to common aeroallergen triggers. Skin prick tests or serum-specific IgE testing (previously called RAST) may help to confirm sensitisation to ryegrass and other aeroallergens. However, given that most patients with allergic rhinitis self-manage symptoms with over-the-counter treatments, the benefits of screening for allergic sensitisation among patients without asthma, particularly in a primary care setting, are unclear.
A significant proportion of patients who present during thunderstorm epidemics do not have a previous history of asthma.23 However, it is important to note that some patients with allergic rhinitis do experience wheeze and attribute this to their ‘hay fever’, rather than to asthma. These patients are, potentially, at risk for thunderstorm asthma, and should undertake recommended precautions. Few other risk factors of note have been identified; smoking is not a risk factor for thunderstorm asthma.20
Optimise asthma and allergy treatment
Inhaled corticosteroids are the cornerstone of therapy for asthma. Although there is no direct evidence from clinical trials about the effectiveness of inhaled corticosteroids in mitigating the effects of thunderstorm asthma, there is some indirect evidence from case-control studies. People attending emergency departments with asthma during a thunderstorm have been shown to be much less likely to be taking inhaled corticosteroids than people attending with asthma at other times.11,20 Hence, it is recommended that at-risk individuals – that is, people with asthma or a history of wheeze who also have seasonal allergic rhinitis and who live in southeastern Australia – should be advised to take regular inhaled corticosteroids during spring and early summer. Correct inhaler technique and adherence to prescribed therapy is essential and is more likely to impact asthma control and protection against thunderstorm asthma than the specific type of inhaled corticosteroid prescribed.
In patients with seasonal allergic rhinitis, either alone or in conjunction with asthma, intranasal corticosteroid therapy is recommended, starting at least two weeks before peak pollen season. In southeastern Australia this would mean starting in September and continuing until at least the end of the year.
Provide self-management strategies
Written asthma action plans allow for discussion between clinicians and healthcare providers on self-management strategies and are an essential component of care. The plan may be based on symptoms and/or peak expiratory flow measurements and serves as a prompt for patients to increase their medication dosing and/or frequency, to recognise when to start oral corticosteroids and particularly the need to seek urgent medical attention. Various action plan templates are available from National Asthma Council Australia (www.nationalasthma.org.au).
Specific advice may also be provided in relation to thunderstorm asthma. Patients with asthma, and particularly those with seasonal allergic rhinitis, should be advised to stay indoors with windows closed just before and during thunderstorms especially during the spring and summer months. At-risk individuals should also be advised to self-administer reliever medication followed by oral corticosteroids (in accordance with their emergency plan) at the onset of symptoms during a thunderstorm. If their symptoms do not rapidly respond to self-administration of a rapid-onset bronchodilator (i.e. salbutamol or formoterol- budesonide combination), they should seek urgent medical assistance – again, in accordance with their emergency plan.
Prepare an emergency response plan
The Melbourne thunderstorm asthma of November 2016 was unprecedented in scale, with a significant proportion of the burden of patient management falling on general practices and the after-hours National Home Doctor Service (Box 1).1 While much retrospective analysis has focused on identifying patients at risk and optimising preventive management, contemporaneous media coverage highlighted the potential contribution of system failures from an overstretched health service to adverse outcomes. These included delayed recognition of a disaster and subsequent escalation procedures, an overwhelmed ambulance service with subsequent delays to patient care and transport, and exhausted stocks of critical medications.24
Given the key role of general practice in healthcare infrastructure, it is imperative that preparation for potential future events also involves consideration of disaster planning and crisis resource management. A public health disaster, whether thunderstorm asthma or otherwise, can have a number of impacts on practices. These may include (but are not limited to):
- increased demand for services
- increased acuity of presentations
- limited critical equipment and supplies
- loss of or reduction in capacity of staff
- reduced access to essential systems (such as ambulance transport)
- limited access to key information.
Successfully navigating an event such as a thunderstorm asthma epidemic requires consideration of how a practice will address these factors before, during and after the disaster. Potential considerations are shown in the Flowchart. Templates for emergency planning are available on the RACGP and CDC websites.25,26
Conclusion
Thunderstorm asthma reflects one of the most dramatic ways in which the environment can impact on the health of a susceptible group of individuals. The GP plays an important role in identifying and managing at-risk patients and preparing for thunderstorm asthma events and other environmental disasters. Given the association between climate change and extreme weather events, further research is required to determine the effects of the environment on respiratory health, and the health of the population in general. MT