Stress-induced asthma – key insights for prevention and management

People with asthma often report stress as a trigger for their asthma symptoms. Educating patients on how stress can affect asthma, helping them to recognise triggers and providing strategies to manage stressors can help prevent stress-induced asthma attacks.
Note
An updated version of this article was prepared for World Asthma Day 2026 and is available here.
- Many people with asthma report stress as a trigger for their asthma symptoms.
- Stress can trigger asthma through multiple physiological and behavioural pathways, including activation of immune mechanisms, changes in breathing patterns and reduced response to asthma medication.
- People with coexisting asthma and mental health problems, as well as people with severe asthma, are more at risk of stress-induced asthma.
- Conditions comorbid with asthma, including mental health problems and dysfunctional breathing, may give rise to symptom misattribution.
- Reducing stress requires multiple strategies, including techniques to deal with an acutely stressful event and long-term solutions to reduce stress levels.
- Patient education and understanding about asthma triggers are important aspects of effective asthma management.
Stress-induced asthma is, as the name suggests, asthma that is triggered by stress. For centuries physicians and philosophers have described a link between emotional state and asthma symptoms.1 Interest in this association has been resurging with evidence that experiencing stress is associated with asthma attacks, poor asthma prognosis and asthma onset in children and adults.
Understanding stress-induced asthma is important as it is likely to be under-recognised yet highly important for symptom management. People with asthma have high rates of stress and anxiety.2,3 The symptoms of asthma overlap with those of stress and anxiety, and can cause symptom misattribution. Correct management of asthma requires identifying symptoms and their causes. Understanding what triggers a patient’s asthma can help practitioners and patients optimise asthma management and prevent asthma attacks.
What is stress?
Stress is the reaction to a potentially threatening or demanding situation (also known as a ‘stressor’).4 A stressor could be an acute, time-limited event, such as seeing a snake during a bushwalk, or a chronic situation, such as ongoing relationship conflict or managing a chronic illness. A stress reaction involves physiological responses (e.g. autonomic and neuroendocrine responses) and psychological responses, including thoughts (e.g. thinking about the stressor as a scary threat or a positive challenge), emotions (e.g. fear, excitement) and coping behaviours (e.g. calling a friend to chat, drinking alcohol).4 When the demands of a situation exceed a person’s coping resources, the stress reaction is often called ‘distress’ and the person experiences sadness, worry and impaired performance.
Having a chronic illness or caring for someone with a chronic illness is a major contributor to an individual’s stress levels.5 Stress can also cause or exacerbate mental illness, including anxiety, depression, compulsive disorders and post-traumatic stress disorder. Anxiety in particular gives rise to stress, as individuals worry about current or future events or recall traumatic events.
Does stress cause asthma attacks?
Between 13 and 23% of people report that stress and other negative emotions (e.g. anger, depression) worsen their asthma.6,7 The relationship between emotional state and asthma symptoms appears to be strong. A recent study found stress and emotion-based triggers were most strongly linked to the development of an asthma attack compared with other triggers including allergens, pollution and infection.8 Various types of stress are associated with asthma symptoms, and include the following.
- Acute stress. A systematic review of laboratory studies on acute stress in people with asthma showed that passive stressors (when the individual cannot control the situation, such as watching a stressful movie or looking at stressful images) produced mild bronchoconstriction.9
- Chronic stress. Defined as ongoing stable stress that lasts weeks, months or even years, chronic stress is associated with asthma attacks, asthma symptoms and a poorer asthma course in children, adolescents and adults.8,10-15
- Major life events. Major and severe life events, such as the loss of someone close, increase the risk of short-term (immediate or within a day or two) and long-term (a month or years after the event) asthma attacks.12,16,17
- Everyday stress. Dealing with repeated minor daily hassles is associated with poor health, particularly if these stresses occur alongside major life events. Everyday stress has been linked to reduced peak expiratory flow rate and asthma symptoms.18
- Combination of acute and chronic stress. Chronic stress may worsen the impact of major life events or acute stress. People experiencing chronic stress have a faster onset of asthma attacks after a severe life event and greater blood and airway inflammatory reactions to acute stressors compared with people not experiencing chronic stress.12,19
- Family stress. In children with asthma, caregiver or family stress and perceived lack of caregiver support are associated with worsened course and altered inflammatory markers.11,20,21
Who is most affected?
People with coexisting asthma and mental health problems may be most at risk of experiencing stress-induced asthma.8 Anxiety, panic and fear are particularly associated with asthma attacks, especially when a person’s fears are related to their asthma.22,23 People with severe or difficult-to-treat asthma may also be at risk of asthma attacks and poor quality of life due to stress.6,14 Higher rates of stress-induced asthma have been reported for people younger than 65 years of age, women and people with atopic asthma.6
What are the symptoms of stress-induced asthma?
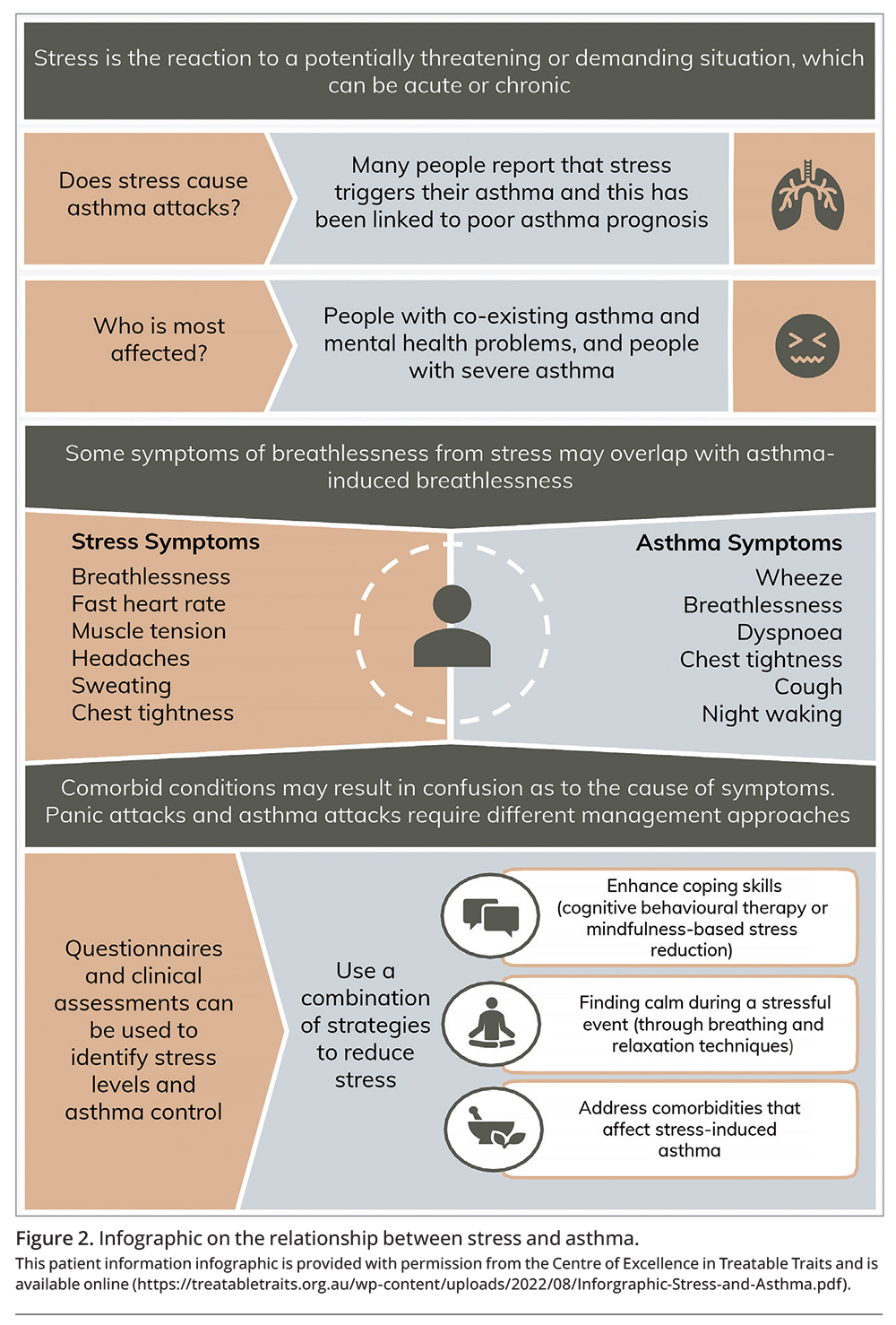
Symptoms of stress-induced asthma are similar to those experienced with other triggers and include wheeze, breathlessness, chest tightness, cough and night waking. However, individuals may also experience symptoms characteristic of the stress response, such as faster or difficult breathing, faster heartbeat, muscle tension, headaches and sweating. Although both stress and asthma can lead to difficulty breathing, the character of the sensation is qualitatively different:
- people experiencing a stress response, anxiety or hyperventilation often say ‘I can’t get a satisfying breath in’ and do not respond to short-acting beta-2 agonists (SABAs)
- people with asthma symptoms often say ‘I can’t breathe out’ and typically respond to SABAs within minutes.
How can stress cause asthma symptoms?
Activation of immune mechanisms
Depending on the stressor, short-term stress – lasting minutes to hours – can either temporarily suppress or enhance the immune response.24 Chronic stress, lasting days to months, can detrimentally affect immune function by disrupting the typical homeostatic functions between inflammatory systems and the neuroendocrine and autonomic stress responses.24
Exposure to chronic stress increases the immune response to environmental asthma triggers (e.g. allergens, irritants, infection) through a sensitisation of the T2 pathway.25-27 The T2 pathway refers to type 2 immune responses, in which type 2 inflammatory cytokines are released via innate and adaptive responses, and promote the effector immune mechanisms, including mucus production, antibody production and IgE-related allergic immune responses. In a classic example of the effect of stress on the health of people with asthma, American college students with asthma had a greater response to an airway allergen test during exam time than during the term.26
Change in breathing patterns
Stress causes irregular breathing, increased respiratory rate and breathlessness in people with asthma.28-30 When someone feels stressed or is anticipating something, using active coping strategies and expending a lot of mental effort results in shallow breathing.28
Hyperventilation – faster, deep breathing – may occur during panic attacks, or in frightening or overwhelming situations in which a person feels they lack control and cannot use their coping skills.28 Laughter, crying and anger can also cause hyperventilation. Hyperventilation is a known asthma trigger, and its presence is used to test for exercise-induced asthma.31 Hyperventilation sets off a chain of physiological responses that affect the airways: the airway mucosa dries out and increases airway osmolarity, triggering mast cell histamine release and sensory nerves, causing cough, bronchospasm, wheeze and breathlessness.29,32
Reduced response to medication
There is some evidence that stress reduces the response to beta agonists and inhaled corticosteroids. Although the mechanisms are not fully understood, stress may induce resistance to the anti-inflammatory properties of glucocorticoid through reduced expression of the genes coding for glucocorticoid receptors.21,33
Ability to self-manage asthma
Complex interaction between environmental risk factors, stressors and individual coping mechanisms can influence disease risk and reduce medication adherence. Populations prone to high levels of stress may have higher exposure to environmental triggers beyond their control; for example, people of low socioeconomic status often live in closer proximity to traffic or have higher exposure to tobacco smoke.27
Enhanced trigger perception
An individual is more likely to correlate intense or unpleasant triggers with asthma symptoms, and distressing events are prime candidates for being identified as triggers.34 When an individual encounters a situation that previously triggered their asthma, they may have a stress response, which further enhances the association between the trigger and asthma symptoms.34 For instance, people with thunderstorm asthma may feel stressed during adverse weather and experience asthma symptoms, regardless of whether environmental conditions that might induce an asthma attack are present.
Is it really asthma?
Asthma is comorbid with a number of other conditions.35 Comorbidities may give rise to symptom misattribution, where the symptoms of one condition are mistaken for another. This is particularly relevant for coexisting asthma and stress or anxiety as these coexisting conditions can also have a cumulative effect on symptom burden.
Accurate diagnosis of asthma, including diagnosing any potential underlying or associated comorbidities, is essential to tailoring the best treatment for each individual at the right time. Figure 1 shows the overlapping symptoms of asthma and three key comorbidities, described below. The Severe Asthma Toolkit has further useful information on these asthma-relevant comorbidities, including their assessment and management (https://toolkit.severeasthma.org.au/co-morbidities/overview/).
{kind=link}
Panic attacks
Compared with the general population, people with asthma have higher levels of anxiety and depression. A subset of people with asthma experience symptoms of panic, characterised by sudden, uncontrollable fear.36 Anxiety or panic are a common reaction to severe breathlessness, and incorporating a ‘respiratory subtype’ for panic disorders has been proposed.37 Experiencing severe breathlessness can lead to avoiding activities that induce breathlessness or an over-reliance on SABA.38,39
Dysfunctional breathing
Dysfunctional breathing describes changes in breathing patterns in the absence or in excess of organic respiratory disease.40 It is common in people with asthma, yet is underdiagnosed.41 Altered breathing patterns have been linked to panic disorder and both cause symptoms that overlap with asthma.42 Since dysfunctional breathing can co-occur with asthma, determining which condition is contributing to the reported symptom burden can be difficult.40
Vocal cord dysfunction
Vocal cord dysfunction, or inducible laryngeal obstruction, is highly comorbid with asthma and characterised by the inappropriate adduction of the vocal cords, leading to breathlessness and tightness in the upper chest or throat region.43 Numerous causes can trigger an episode of vocal cord dysfunction, including coughing, odours and emotional stressors.44 Like dysfunctional breathing and panic attacks, symptoms of vocal cord dysfunction overlap with asthma; therefore, teasing out the cause of symptoms is essential.
Asthma attack or panic attack: does it make a difference?
Although asthma and panic attacks share some symptom commonalities, they are fundamentally different in their underlying mechanisms and, therefore, respective treatments. Careful assessment of the clinical features of an attack is essential for effective symptom management. Some of the warning signs for an asthma attack include increased shortness of breath, increased respiratory rate, increased cough and wheeze, increased use of reliever inhaler and reduced peak flow. An asthma attack can worsen quickly and can include the additional symptoms of difficulty speaking in full sentences, lethargy, gasping for breath, drowsiness confusion and exhaustion. The consequences of ineffective treatment for an asthma attack can be detrimental, and may even result in death. Conversely, providing treatment for an asthma attack when it is a panic attack can also lead to worsened outcomes. For example, SABAs can activate the sympathetic nervous system, causing symptoms of anxiety. This may be a concern for people with stress-induced asthma. If a person finds their inhaler makes them feel more stressed, they should speak with their GP. An infographic on how stress can affect asthma is presented in Figure 2 and is available online (https://treatabletraits.org.au/wp-content/uploads/2022/08/Inforgraphic-Stress-and-Asthma.pdf).
{kind=link}
How to assess stress
Formal questionnaires to assess an individual’s levels of stress or distress include the Perceived Stress Scale (PSS), which focuses on how an individual feels about their current situation and assesses their hopelessness and self-efficacy, and the Kessler-10 Psychological Distress Scale (K-10), which focuses on an individual’s level of distress, and can be a useful indicator for whether further assessment and intervention for anxiety or depression are needed.45,46 The Stress Measurement Network Toolbox has curated a list of questionnaires and checklists for many types of stressors and stress responses, such as life events, caregivers stress, financial strain, relationship conflict and systemic racism (https://www.stressmeasurement.org/measurement-toolbox).
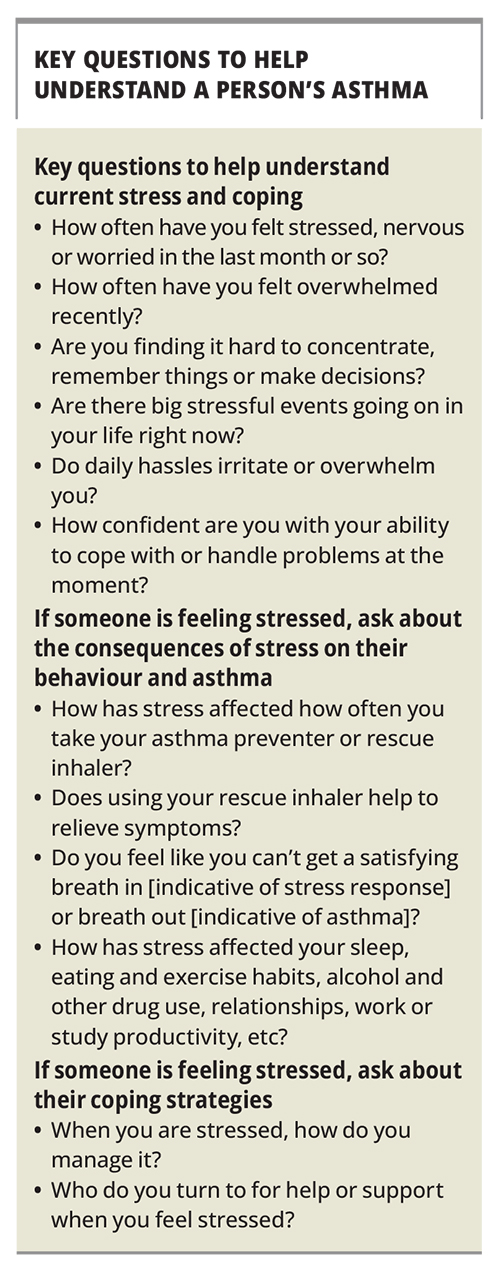
Often, rather than a questionnaire, a conversation can help to gauge an individual’s stress level. Key questions healthcare providers can ask patients are listed in the Box.
{kind=link}
How to assess asthma control and triggers
The Asthma Control Questionnaire is a useful way to assess current level of asthma control.47 The Asthma Trigger Inventory may provide a structured way to assess a person’s asthma triggers, including emotional triggers.48 A diary approach, where a patient records triggers and asthma symptoms between appointments, is another strategy for assessing asthma triggers and control. Healthcare providers may want to have a conversation with patients about their asthma triggers, asking key questions such as:
- What things trigger your asthma?
- What feelings and sensations do you experience when these triggers occur?
- Does using your rescue inhaler help?
Reducing or preventing stress in people with asthma
There is not a one-size-fits-all solution to reducing or preventing stress. One person might find that attending a yoga class enhances their ability to cope with stress, whereas others will despise yoga as a stress-management technique. However, people need to engage in multiple strategies to help buffer the deleterious effects of chronic stress on health. Effective techniques can help to manage symptoms during a stressful situation and provide strategies to improve coping skills and resources long term.24
Acute stress symptom management
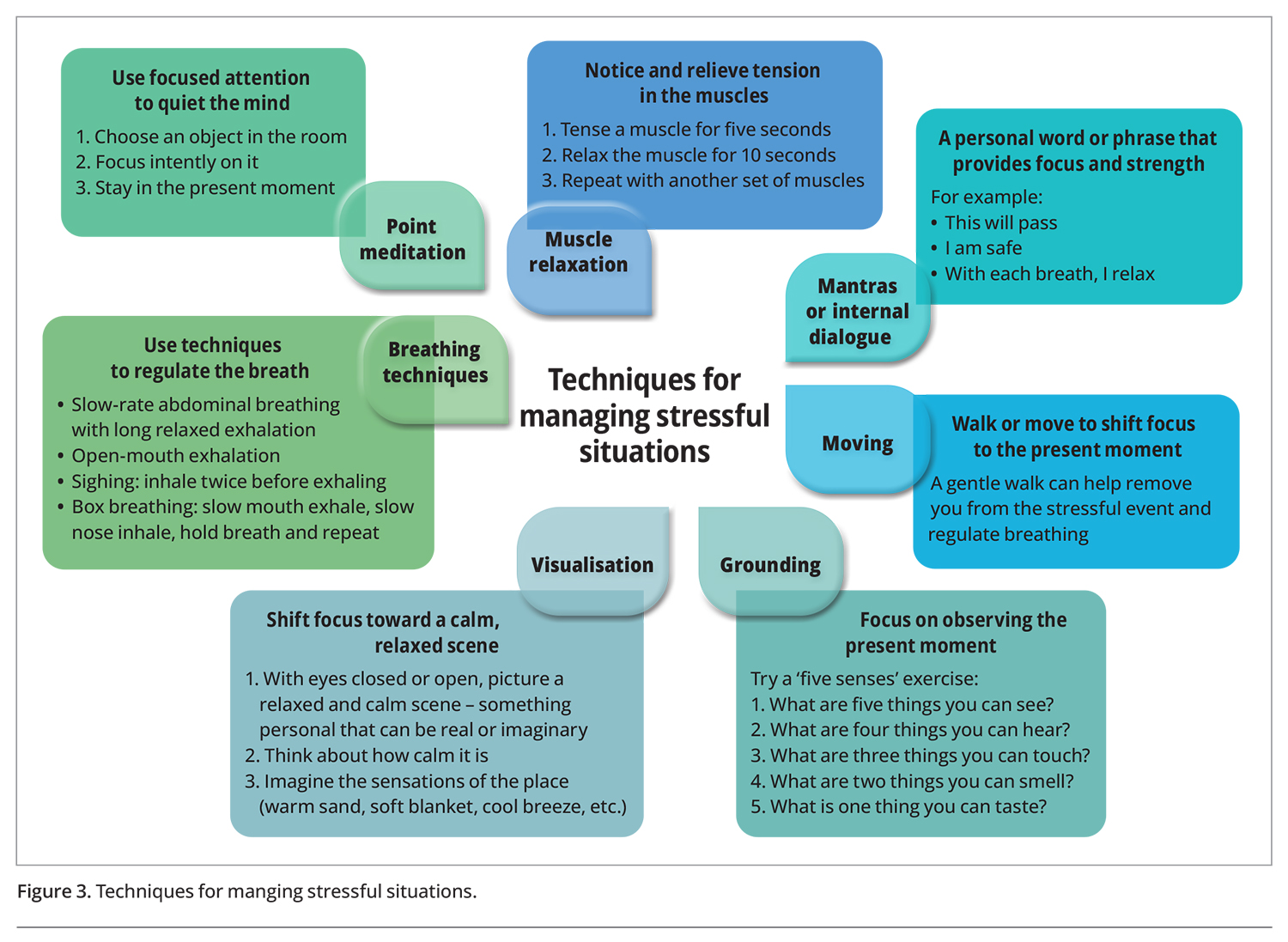
If stress is the suspected cause of symptoms, individuals might try one of the following techniques during an immediately stressful event: point meditation or focus, breathing or grounding techniques, muscle relaxation, visualisation, mantras or internal dialogue, or walking (Figure 3). However, if these strategies do not improve symptoms, and asthma is the suspected cause, acute asthma management should be implemented.
{kind=link}
Long-term stress prevention and management
To improve levels of stress long term, individuals can be advised to look at how they react to stressors, enhance their coping skills and address comorbidities that affect their stress-induced asthma. Components of a comprehensive long-term stress reduction plan are outlined below.
Breathing training
Some well-known breathing training approaches for people with asthma include yoga, the Papworth method, Buteyko breathing and the Southampton approach, and can be delivered by a respiratory physiotherapist. These techniques have shown positive effects on quality of life and hyperventilation.49,50
Relaxation and meditation strategies
Strategies such as progressive muscle relaxation yoga and meditation may be helpful for reducing stress.49,51 One program specifically designed for stress management is mindfulness-based stress reduction therapy, which has been used widely among people with chronic diseases and has shown to improve mental health.52 Trained providers deliver this program throughout Australia.
Adapting mindset
Psychologists, counsellors and other mental health professionals help people restructure how they view and react to the world. This might involve changing how someone evaluates stress, such as viewing stressors as a challenge to be learnt from, or helping someone understand the personal resources and coping skills they can use to tackle stress. Alternatively, patients may like to explore evidence-based self-help materials, apps or online programs that aim to improve wellbeing, stress or resilience. The eCentreClinic has developed online materials that may help people with asthma manage their stressors (https://www.ecentreclinic.org/our-courses).
Activities for enjoyment and relaxation
Scheduling enjoyable activities can help alleviate stress. The specific activity is entirely dependent on the individual; people may find relaxation and enjoyment in Tai Chi, bushwalking, fishing or listening to music, for example.
Social support
Engaging with supportive people can be a good stress buffer. Such contact can provide:
- emotional support (offering empathy, encouragement and validation)
- information (giving advice and helping with decision making)
- practical assistance (help with doing practical things, such as child-minding or mowing the lawn)
- a support network of people with similar experiences, which offers a sense of belonging.
Healthcare providers can also provide information and emotional support, and may know community links for practical and network support.
Lifestyle changes
Good sleep hygiene, a high-quality diet and physical activity may buffer negative effects of stress.53 Sleep goals may include aiming for 7 to 8 hours of sleep per night, having a consistent bedtime and wake-up time, creating a relaxing sleep environment and avoiding caffeine close to bedtime.53 Australian diet and exercise guidelines recommend eating a varied whole-food diet (including fruits and vegetables, whole grains and healthy fats), drinking water, avoiding foods high in saturated fat and sodium, being physically active every day (at least 2.5 hours of moderate activity or 1.25 hours of vigorous activity per week) and engaging in musclestrengthening exercise twice a week.54,55
Asthma management
People with asthma often report that they feel they have a lack of control over their health.3 A quality asthma management plan codeveloped with the patient may help. Monitoring triggers alongside peak flow and asthma symptoms may help detect unidentified or misidentified triggers.34 A personalised written action plan can describe actions a patient should take after exposure to different triggers, such as when to use techniques to manage acute stress (Figure 3) and when to initiate SABA therapy. Co-ordinating care can also assist in improving stress levels for people with chronic illness such as asthma.
Anxiety and depression intervention
Pharmacotherapy and psychological therapies can be used alone or jointly to improve anxiety and depression. People with coexisting asthma and panic disorder may benefit from education and development of strategies to differentiate asthma triggers from triggers of panic attacks.34,56 Exposing patients to misidentified asthma triggers under medical supervision might reduce anxiety related to these triggers and therefore improve asthma symptoms.34
Why patient education on asthma control and triggers is important
Self-management skills and adherence to asthma medication are a central to asthma management. Assessing inhaler device technique and adherence, as well as current level and severity of asthma symptoms are important. Although many clinicians ask about triggers, especially after an asthma attack, providing advice on avoiding triggers is less common and follow-up on adherence to this advice is even rarer.57 Education about asthma control and triggers is an important part of asthma management.51 Understanding a patient’s asthma symptoms and triggers can help to optimise management through development of a personalised written action plan that addresses the triggers as well as the symptoms caused. More information on personalised written action plans is available on the Severe Asthma Toolkit website (https://toolkit.severeasthma.org.au/management/written-action-plans/).
Conclusion
Understanding what triggers an individual’s asthma is important for developing effective asthma prevention and management strategies. Many people report that stress triggers their asthma, which may be due to several biological and psychological mechanisms. Stress is also associated with poor asthma prognosis. Assessment and patient education regarding relevant comorbidities are particularly important to help recognise and manage stress-induced asthma. Conditions that co-occur with asthma, including panic disorder, dysfunctional breathing and vocal cord dysfunction, may lead to symptom misattribution, which is problematic when different symptoms require different approaches to management. Stress-induced asthma can be assessed through questionnaires or conversations. People with stress-induced asthma may benefit from learning skills to manage an acute stress reaction, improving coping skills to reduce stress levels in the long-term, and managing comorbidities that affect stress-induced asthma, including learning to distinguish symptoms of asthma from those due to comorbid conditions. MT
COMPETING INTERESTS: Dr Hiles and Dr Clark: None. Professor Gibson is Co-Director of the NHMRC Centre of Research Excellence in Asthma Treatable Traits; and receives honoraria from GlaxoSmithkline, AstraZeneca and Novartis. Professor McDonald is Co-Director of the NHMRC Centre of Research Excellence in Asthma Treatable Traits; receives funding from GlaxoSmithkline, AstraZeneca, NHMRC, Ramaciotti, MRFF and the JHH Charitable Trust; and is a member of the COPD-X Guideline Committee.
References
dietary_guidelines_summary_book.pdf (accessed October 2022).
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.