Evolving therapies for severe asthma: the role of the GP

Asthma
GPs have a key role in optimising asthma treatments, recognising patients with severe or refractory asthma and referring them for specialist review and consideration of emerging treatments. Long-term use of oral corticosteroids should be avoided if possible. New therapies recommended in guidelines on severe asthma include tiotropium and biological therapies such as omalizumab and mepolizumab.
- In Australia, asthma affects about 10% of people, and 3 to 10% of these have difficult-to-treat or severe disease.
- Severe asthma is defined as asthma that is inadequately controlled despite maximal doses of inhaled corticosteroids and long-acting beta2 agonists or asthma that requires oral corticosteroids in addition to maximal inhaled therapy to remain controlled.
- Patients with severe asthma should be referred to a specialist for evaluation and institution of biological treatments if appropriate.
- Emerging therapies for severe asthma include biological treatments that target specific inflammatory pathways, such as omalizumab and mepolizumab.
Picture credit: © Portra/iStockphoto.com Model used for illustrative purposes only
Asthma is a chronic inflammatory disease of the airways that develops from complex interactions between the innate and adaptive immune systems and airway epithelial cells, leading to bronchial hyper-reactivity, increased mucus production, and structural airway remodelling.1 This results in the clinical manifestations of asthma, which include variable symptoms such as wheeze, shortness of breath, cough and chest tightness, owing to the significant variability in lung function.2 In Australia, one in nine people have a diagnosis of asthma.3 In most of these, asthma can be well controlled with conventional therapy using preventer and reliever inhalers, but a subset of patients are refractory to maximal-dose inhaler therapies. The prevalence of difficult-to-treat and severe asthma is estimated to be 3 to 10% of people with asthma, and this group accounts for the major burden of health expenditure for asthma.4,5
Most people with asthma are cared for by their GPs. General practitioners play a crucial role in the diagnosis and assessment of patients with asthma, the prescription of therapy and monitoring of adherence to a medication regimen. They are also responsible for recognising patients with severe asthma. Although not all cases of difficult-to-treat asthma represent severe asthma, identification of patients with uncontrolled symptoms or abnormal lung function is a first step in considering a diagnosis of severe asthma. Because of the high morbidity and mortality associated with severe asthma, it is important to identify at-risk patients and to refer them for specialist advice to improve patient outcomes by preventing overtreatment and providing access to biological therapies.
Severe asthma is associated with a substantial burden of chronic disease caused by inadequate symptom control, comorbidities, medication side effects, especially from systemic corticosteroid use, and the broader implications for quality of life.6,7 Patients with severe asthma contribute significantly to the economic costs of asthma in Australia due to healthcare expenditure and loss of productivity.8 Recognition of the impact of severe asthma has led to the development of evidence-based treatment guidelines that facilitate titration of therapy by asthma severity and provide a framework for the use of emerging treatments such as biological therapies.9
Confirming the diagnosis of asthma
In an individual who presents with symptoms suggesting asthma, the diagnosis is confirmed by lung function tests that demonstrate reversible airflow limitation, with an increase in the forced expiratory volume in one second (FEV1) after administration of a bronchodilator of more than 200 mL and more than 12%. However, normal results on lung function testing do not exclude the diagnosis because of the episodic nature of asthma. An alternative test to demonstrate reversible airway obstruction is a peak flow diary kept over one to two weeks. Specialist referral can also be considered for bronchial provocation testing to evaluate airway hyper-responsiveness if asthma is being considered but lung function test results are normal. Measurement of the fractional exhaled nitric oxide (FeNO) level is also increasingly used in adults to provide evidence of airway inflammation that is suggestive, but not diagnostic, of asthma.10
Lung function tests that show fixed airway obstruction may suggest asthma–chronic obstructive pulmonary disease (COPD) overlap (ACO), which results from chronic airway remodelling from asthma or as a consequence of tobacco smoking.11 The alternative diagnosis of COPD should be considered in patients who present with breathlessness over the age of 40 years and have a history of smoking, passive smoking, exposure to air pollution or occupational exposure to particulate matter such as organic and inorganic dusts.
Treating patients with asthma
Initiating asthma treatment
Improving health literacy with education is imperative for patient self-management of asthma. Selection of an appropriate inhaler device and education on inhaler technique should be provided at the point of care and reviewed regularly (useful video resources are available at www.asthmahandbook.org.au). Ensuring patient comprehension is vital; comprehension can be effectively assessed by requesting the patient to demonstrate what they have learnt.12 For patients with physical or cognitive impairment, the use of certain inhalers can be more challenging. Consider trialling practice inhaler devices and use of a spacer in the GP’s office. Education of family and carers regarding technique and administration may improve adherence. Referral to an asthma educator may also be helpful.2,13 All patients should receive a written action plan. This plan should be regularly reviewed and updated. Simple plans have been shown to work better regardless of the patient’s level of literacy.12 Libraries of such plans are available at the website of the National Asthma Council Australia (www.nationalasthma.org.au).
Barriers to adherence should be assessed, as most patients do not use their preventer as prescribed when symptoms are mild or intermittent. It is estimated that only half of all patients with chronic health conditions such as asthma take their medications at therapeutically effective doses.2,14 Common barriers to adherence include beliefs about treatment, inconvenience and adverse effects. Poor adherence can be unintentional; common failures include forgetfulness or underdosing caused by the prohibitive cost of medication. Strategies to improve adherence include setting phone checklist reminders, rationalising inhalers and shared treatment decision-making.14
Evaluating asthma control
After an asthma diagnosis has been confirmed and treatment prescribed, patients should be reviewed regularly to assess their response and satisfaction with treatment and to titrate the treatment. Symptom control and side effects of medications should be explored and documented. Lung function test results should be recorded at diagnosis, three to six months after commencing treatment and periodically thereafter.13
Patients with well-controlled asthma:
- have no limitation of activities
- use reliever medication less than twice a week to relieve symptoms
- do not have wheeze during the day or night-time
- do not wake at night with asthma.
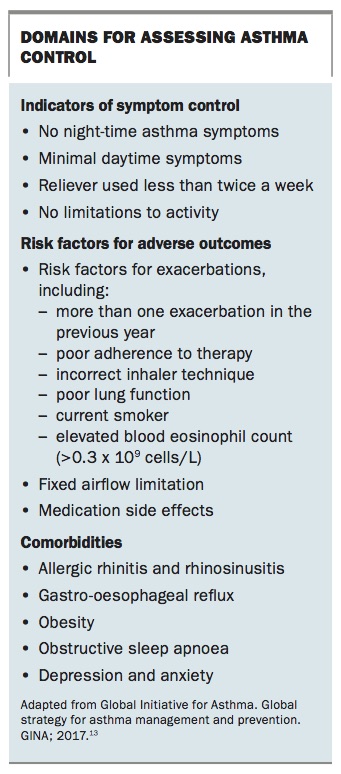
Reliable tools for assessing asthma symptom control include the Asthma Control Test and the Asthma Control Questionnaire. These tools can be used to evaluate asthma symptom control over time. Other domains of asthma control that should be evaluated include the future risk of adverse outcomes, such as exacerbations and their severity. Patients should also be assessed for comorbidities. Domains for assessing asthma control are shown in the Box.13
{kind=link}
In patients with poor asthma symptom control, it is important to consider whether the asthma is refractory to conventional treatment or a result of poor adherence to therapy. Optimising inhaler therapy is essential for effective asthma management.
Adjusting treatment
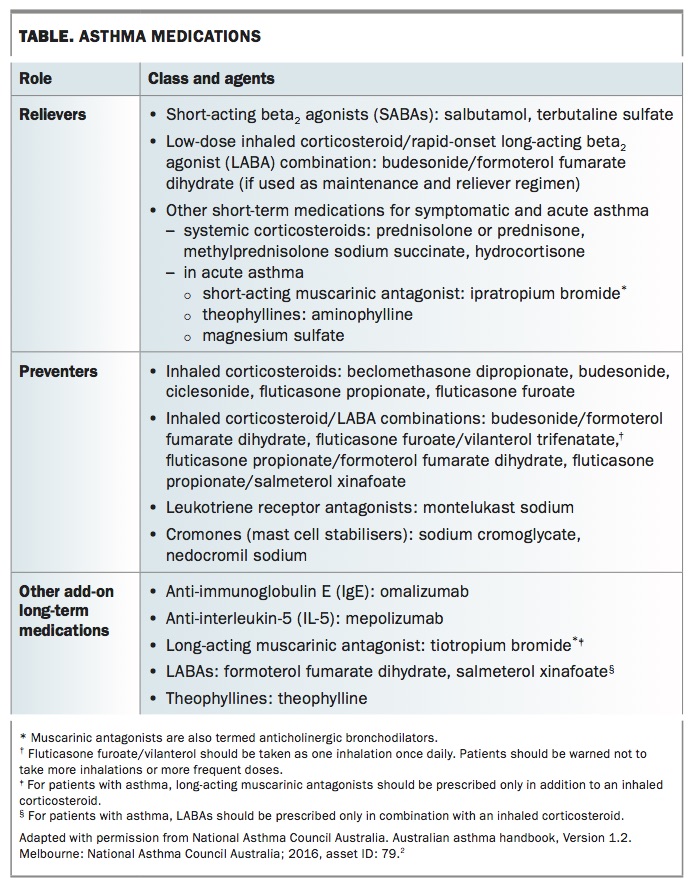
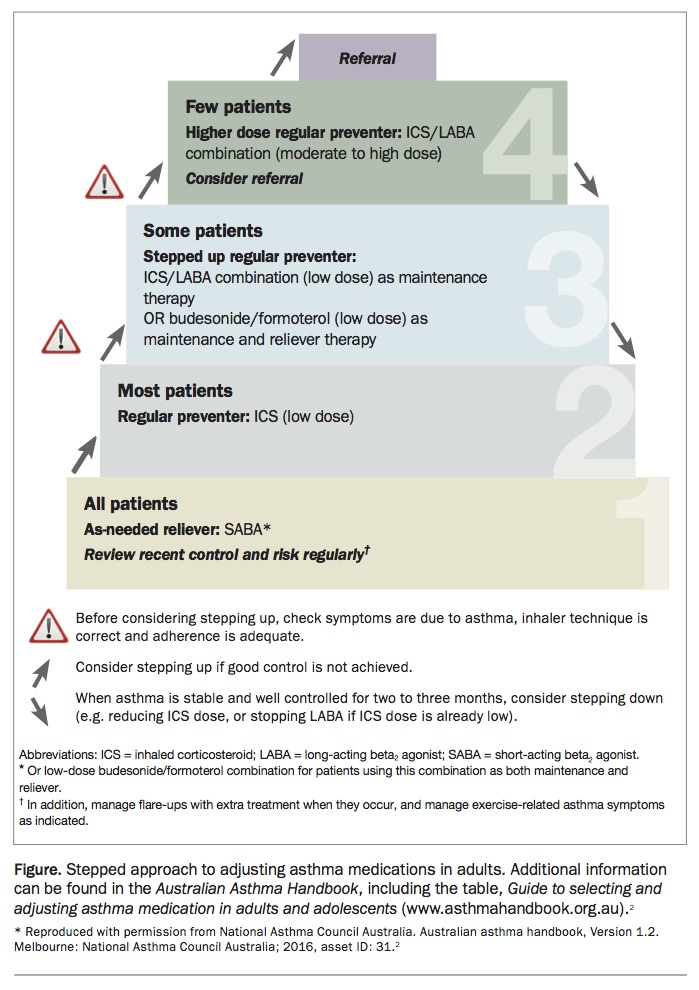
Asthma medications should be adjusted on the basis of regular assessment, with stepping up of treatment when symptoms are poorly controlled and stepping down when good asthma control has been maintained for three months. Available asthma medications are summarised in the Table.2 A stepped approach to adjusting asthma medications in adults is shown in the Figure.
{kind=link}
{kind=link}
Most patients who experience asthma symptoms more often than twice a month should be prescribed inhaled corticosteroid therapy in addition to a short-acting beta2 agonist (SABA) to use as required. In those with more frequent or severe symptoms, the next step is inhaled combination therapy with a corticosteroid and a long-acting beta2 agonist (LABA). Few patients require high-dose inhaled corticosteroid/LABA therapy.
An alternative regimen for patients with moderate to severe asthma is single-inhaler maintenance and reliever therapy. This regimen combines the use of the rapidly acting LABA, formoterol, with an inhaled corticosteroid for maintenance treatment and also for reliever therapy. This mode of therapy may offer advantages in protection from asthma exacerbations.
Patients whose asthma remains poorly controlled despite high-dose inhaled corticosteroid and LABA therapy should be referred for specialist evaluation.
Other management
Annual influenza vaccination is recommended and available free of charge for patients with severe asthma.13 However, it may not reduce the risk or severity of asthma exacerbations.2 Nonpharmacological interventions, such as encouraging physical activity, weight loss and smoking cessation, are also recommended.
Allergies that contribute to upper and lower airway inflammation should be managed, especially when asthma coexists with rhinitis or rhinosinusitis. Allergic disease can be diagnosed by measurement of blood levels of specific IgE to common environmental allergens. Intranasal corticosteroids are first-line treatment for moderate to severe allergic rhinoconjunctivitis and are recommended in addition to regular inhaled corticosteroids for patients with difficult-to-control coexisting allergic asthma and rhinitis. If intranasal corticosteroids are not tolerated and symptoms persist then oral antihistamines should be considered. If allergic rhinitis symptoms continue to be significant then referral for specialist allergy testing and treatment is indicated.2
Recent evidence confirms the efficacy of sublingual immunotherapy for house dust mite (HDM) allergy in improving asthma control.15 Guidelines for asthma care now recommend this form of therapy for HDM-sensitised patients with allergic rhinitis and asthma.13 However, as allergen immunotherapy is not PBS-listed, the cost to patients can be a problem.
Some individuals with poorly controlled asthma describe known asthma triggers associated with environmental airborne irritants, such as cold or dry air, fuel combustion, home renovations materials, household aerosols, moulds, outdoor industrial and traffic pollution, perfumes, smoke and thunderstorms.2 Avoidance of triggers is recommended but is not always achievable.
For patients with a known sensitivity to an allergen, avoidance can also be helpful, if possible. Allergens that can potentially trigger asthma include animal allergens, house dust mites, moulds, occupational allergens, and grass and tree pollens. Recent epidemic asthma events (‘thunderstorm asthma’) highlight the potential of grass pollen allergy to be associated with asthma exacerbations and suggest that treatment of seasonal allergic rhinitis as well as asthma is likely to be important in patients sensitised to grass pollen.
Certain medicines can cause asthma flares, including NSAIDs (in patients with aspirin-exacerbated respiratory disease) and beta blockers (including topical therapies such as eye drops to treat glaucoma).2
Recognising severe asthma
In 2014, the American Thoracic Society and European Respiratory Society collaborated to produce the current guidelines for diagnosis and management of severe asthma.5 Severe asthma is defined as:
- asthma with poor symptom control despite the use of high-dose inhaled corticosteroids combined with a LABA, a leukotriene modifier or theophylline for a year, or
- asthma that requires oral corticosteroids in addition to maximum inhaled therapy to prevent it becoming uncontrolled or that continues to be uncontrolled despite this therapy.
Asthma is considered uncontrolled when there is poor symptom control or frequent and/or severe exacerbations. An additional feature indicating severe asthma is the presence of fixed airflow limitation – an FEV1 less than 80% of predicted despite optimal medication. However, it is important to recognise that uncontrolled asthma is not always severe asthma. A diagnosis of severe asthma should be made only when the asthma diagnosis has been confirmed, medication use has been optimised and possible alternative diagnoses such as gastro-oesophageal reflux and upper airway dysfunction have been investigated and managed.
New therapies for severe asthma
After a diagnosis of asthma is confirmed and the treatment regimen is optimised, patients who still meet the criteria for severe asthma should be referred for specialist review and consideration of biological and other new therapies for asthma. Long-term use of oral corticosteroids should be avoided when at all possible because of the risk of both short- and long-term adverse effects.16
Tiotropium and azithromycin
In addition to inhaled glucocorticoids and LABA therapy, patients with severe asthma may be considered for a trial of tiotropium. This long-acting muscarinic antagonist has been shown to increase the time to the first exacerbation and lead to a modest improvement in lung function in patients with poorly controlled asthma.17
A recently published study from Australian investigators showed that add-on therapy with azithromycin taken three times a week reduced exacerbations and improved asthma-related quality of life in patients with moderate to severe asthma.18 Further studies are required to identify the subgroup of asthma patients most likely to respond to this treatment, and its risks need to be considered (e.g. ototoxicity and prolongation of the QT interval). Azithromycin is not registered with the TGA for this indication.
Biological therapies
Biological therapies, comprising monoclonal antibodies, have been introduced over the past decade for the management of patients with severe asthma. These therapies have been life changing for some patients but are often expensive. Patients should be selected using an integrated approach to assessment of clinical features and biomarkers and careful consideration of adherence to conventional medication.9
Omalizumab
Omalizumab was the first monoclonal antibody to be widely marketed for severe asthma. It is an anti-IgE antibody that binds circulating IgE and thereby prevents it binding to mast cells and basophils, reducing allergic responses. Omalizumab is currently subsidised by the PBS for eligible patients with severe allergic asthma, a total IgE level of 30 IU/mL or higher, and a history of atopy documented by skin-prick or specific IgE testing.
Omalizumab is administered by subcutaneous injection every two to four weeks (depending on the dose) and is added to maximum inhaled therapy. In major clinical trials, omalizumab has been shown to reduce exacerbations by over 25% but to have a minimal effect on FEV1.19,20
Mepolizumab
Mepolizumab is a monoclonal anti-interleukin(IL)-5 antibody that binds to and inactivates circulating IL-5, thereby reducing the concentration of circulating eosinophils. In Australia, mepolizumab is subsidised on the PBS for eligible patients with severe eosinophilic asthma and a blood eosinophil count of 300 cells per microlitre or higher. Although this eosinophil count is within the normal range, it is likely to represent persisting eosinophilic airway disease for an individual taking high-dose inhaled or oral corticosteroids.
Mepolizumab is administered by a monthly subcutaneous injection. In clinical trials, mepolizumab has been shown to reduce exacerbations by more than 40%, to reduce asthma symptoms, to reduce oral corticosteroid therapy and to have a modest effect on FEV1.21-23
Biological therapies not approved in Australia
Benralizumab is a monoclonal antibody directed against the IL-5 receptor. It induces eosinophil apoptosis thereby reducing the concentration of circulating eosinophils. It was recently approved by the US Food and Drug Administration. Benralizumab is administered by subcutaneous injection. Phase 3 clinical trials in patients with one or more asthma exacerbations per year and a baseline blood eosinophil count of 300 cells per microlitre or higher showed that benralizumab reduced exacerbations, asthma symptoms and oral corticosteroid therapy and had a small effect on FEV1.24-26 Reslizumab is another anti-IL-5 agent that has shown efficacy in patients with eosinophilic asthma.27
Dupilumab is a monoclonal antibody directed at the IL-4 receptor alpha subunit, which inhibits both IL-4 and IL-13 signalling.28 Reducing IL-13 has the potential to alter airway inflammation and smooth muscle reactivity.9 Dupilumab is administered by subcutaneous injection. Clinical trials of dupilumab in patients with moderate-to-severe asthma and an elevated blood eosinophil count who used medium- dose to high-dose inhaled corticosteroids plus LABAs showed a 60 to 80% reduction in exacerbations and a clinically significant improvement in FEV1.28,29 Although dupilumab is promising, the results of phase 3 trials are awaited to inform regulatory submissions.
Conclusion
Therapeutic opportunities for patients with severe and refractory eosinophilic asthma are expanding. Given the availability of these therapies, no patient with asthma should be treated with continuous oral corticosteroids, even at a low dose, or frequent bursts of oral corticosteroids without specialist referral for confirmation of the severe asthma diagnosis, optimisation of asthma treatment and consideration of a biological therapy. GPs are key in initiating and optimising asthma treatments, recognising patients with severe or refractory asthma and expediting their referral to a specialist. Once effective biological therapies are initiated, most are continued by the GP with infrequent specialist review.
Therapies for severe asthma are evolving, but their application depends on the GP’s care in instituting effective asthma treatments, promoting medication adherence and recognising the small number of patients who fail to respond to conventional high-dose inhaled corticosteroid and LABA therapy. Unless patients with severe and refractory asthma are recognised and referred then most will remain at risk of exacerbations, consequent decline in lung function and the development of irreversible airflow obstruction and will continue to suffer the burden of severe symptoms. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.