The vomiting child. Considerations and red flag symptoms

Digestive diseases
Vomiting is a common and nonspecific sign of multiple illnesses in infants and children, ranging from benign and self-limiting to life-threatening and requiring immediate management. A careful clinical evaluation, with consideration given to the most serious differential diagnoses, is necessary.
- Causes of vomiting in children vary from the benign and self-limiting to life-threatening.
- Distinguishing vomiting from regurgitation that is effortless or rumination that is not forceful is important.
- Consideration of the broad range of diagnostic groups of gastrointestinal/abdominal, neurological/psychological and systemic illnesses that may result in vomiting assists in identifying the principal causes.
- Extra caution should be taken when assessing children with red flag symptoms and signs.
Vomiting refers to the forceful and involuntary expulsion of gastrointestinal contents from the mouth. This requires co-ordinated contractions of the thoracic and abdominal muscles and changes in upper gastrointestinal motility (antiperistalsis). Vomiting is usually associated with nausea. When taking a patient history it is important to distinguish vomiting from regurgitation that is effortless or rumination that is not forceful.
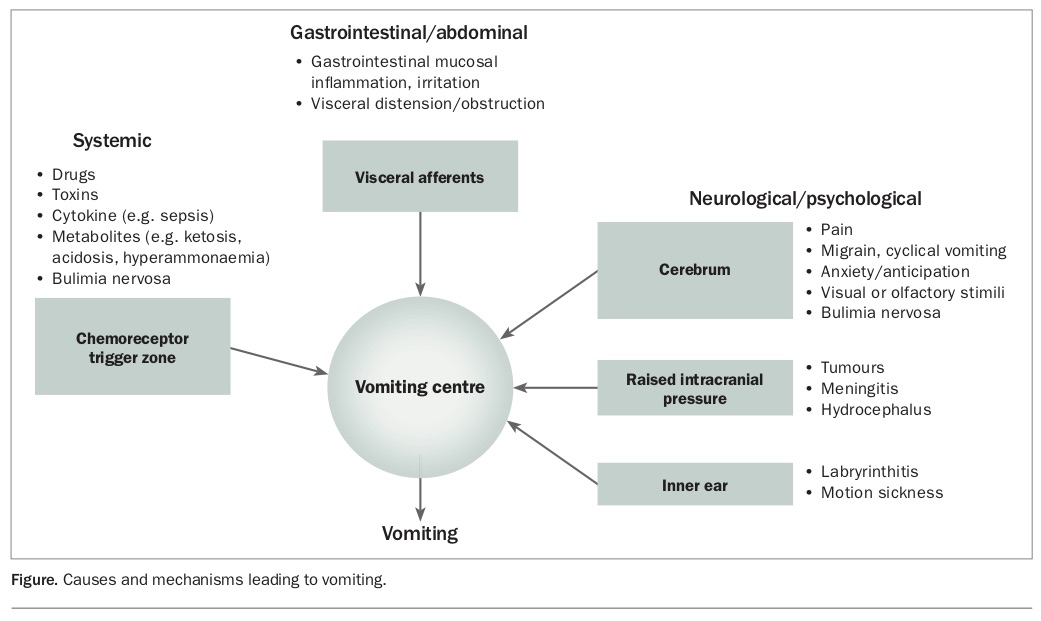
Vomiting can result from several pathophysiological mechanisms that activate the vomiting centre (an area of the medulla oblongata). Afferent neurons originate in the gastrointestinal tract, the cerebral cortex and thalamus, the vestibular apparatus and the chemoreceptor trigger zone.1 Consideration of these various mechanisms will help identify the principal cause of vomiting, which can be broadly classified as:
- gastrointestinal/abdominal
- systemic
- neurological/psychological (Figure).
{kind=link}
Clinical assessment
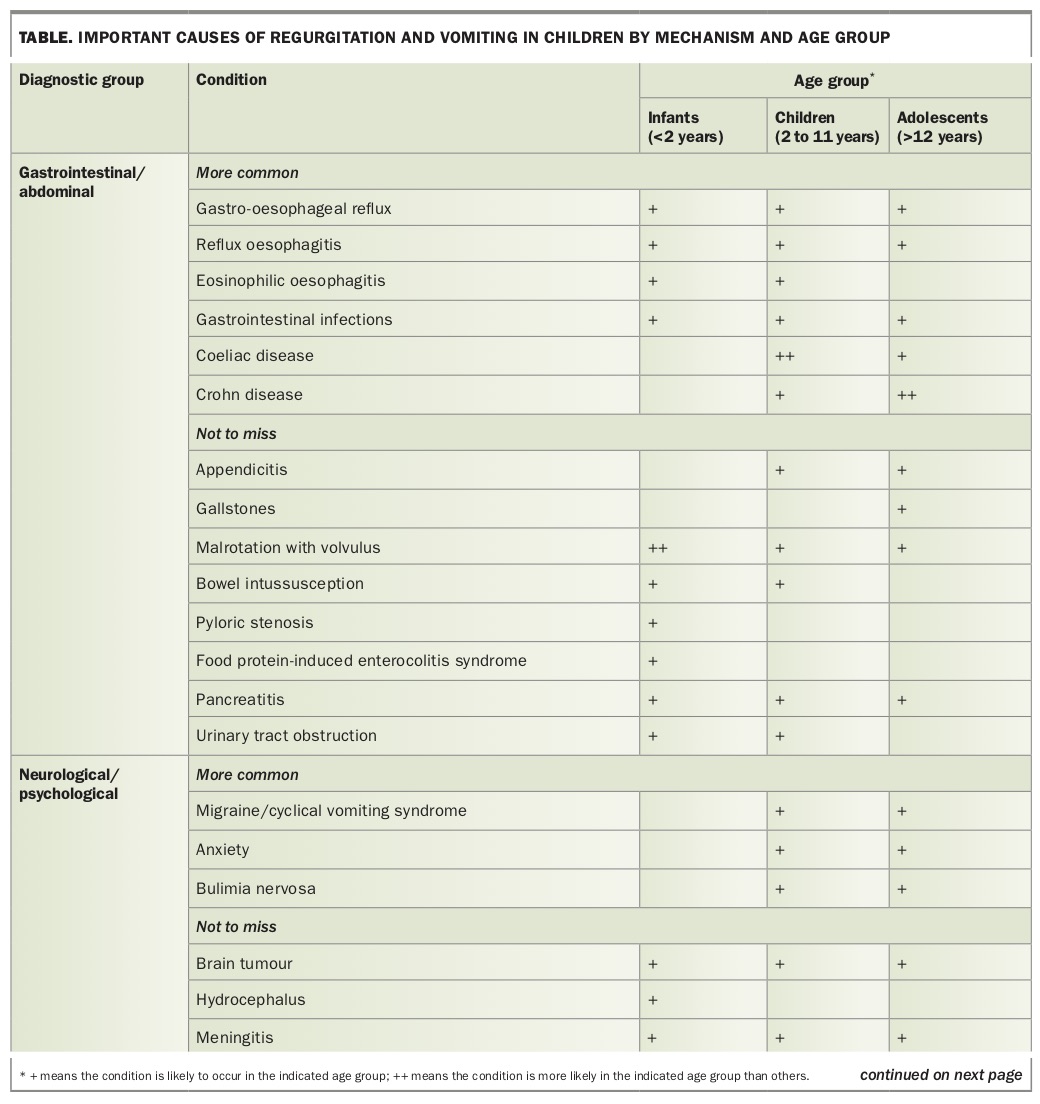
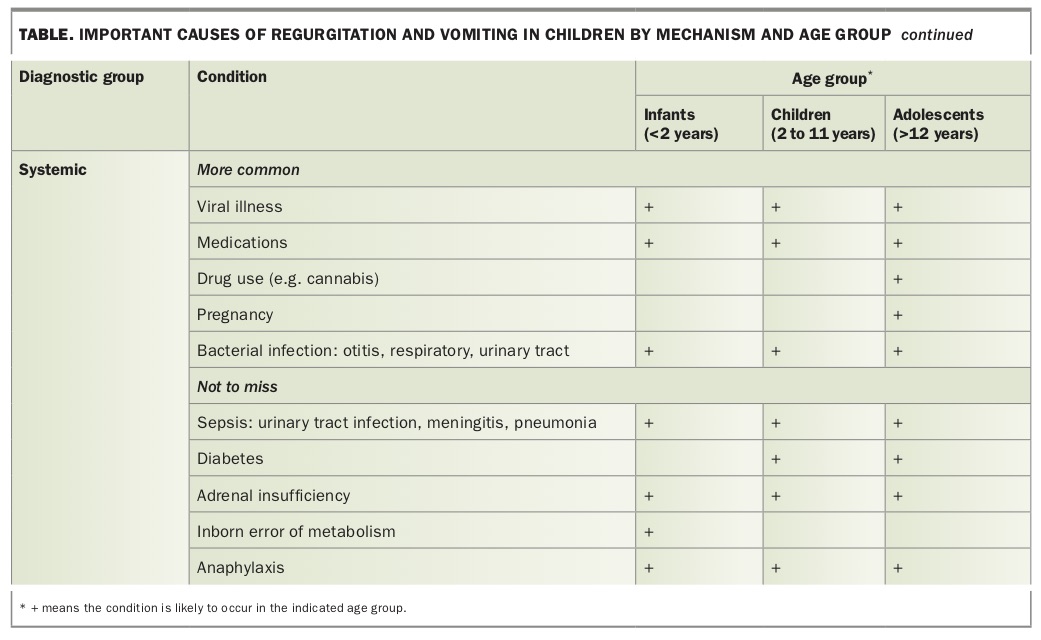
An assessment of the vomiting child is assisted by systematically considering the broad diagnostic possibilities, keeping in mind key ‘not to miss’ diagnoses such as sepsis, surgical emergencies, raised intracranial pressure and metabolic causes (Table Pt 1 and Pt 2). Consideration of the age and past history of the patient, acuity of presentation and associated symptoms can assist in reaching a provisional and differential diagnosis that directs investigations and initial management.
{kind=link}
{kind=link}
Gastrointestinal and abdominal causes
Gastrointestinal causes of vomiting in infants and children include commonly encountered conditions such as acute viral gastroenteritis. Fever or diarrhoea may be associated at the time of presentation and sick contacts are common, but be aware that sepsis can initially present with these nonspecific symptoms. Care should be taken in ascribing a diagnosis of acute gastroenteritis when vomiting presents without diarrhoea.
Inflammation of the upper gastrointestinal tract may also occur with chronic conditions such as coeliac disease, eosinophilic oesophagitis, reflux oesophagitis or less commonly, Crohn disease. Oesophagitis is suggested by heartburn, epigastric discomfort or dysphagia. When associated with weight loss, lower gastrointestinal symptoms or iron deficiency anaemia, coeliac disease or inflammatory bowel disease should be considered.
Surgical conditions such as acute appendicitis should be considered when vomiting is associated with abdominal pain, particularly if fever is present. Infantile hypertrophic pyloric stenosis typically presents at about 5 to 6 weeks of age, with persistent, profuse vomiting that is nonbilious and poor weight gain or weight loss. A small epigastric mass may be palpable in about half of cases seen, with visible peristalsis in the upper abdomen seen in one-quarter of cases.2 These infants can become dehydrated and develop profound electrolyte disturbances quickly (typically hypochloraemic alkalosis) and require urgent referral to hospital. Congenital gastrointestinal lesions such as malrotation and small bowel volvulus can present at any age. An important clue is bile-stained (green) vomitus, which mandates urgent referral to a hospital that has a paediatric surgeon as this condition can lead to devastating intestinal infarction.3
Abdominal causes outside the gastrointestinal tract include acute pancreatitis (accompanied by pain that is epigastric in children who are old enough to articulate this) and ureteropelvic junction obstruction, which presents as chronic vomiting and abdominal or flank pain, and an abdominal mass that may be felt.
Happy, thriving infants with effortless regurgitation of milk feeds and a normal physical examination have gastro-oesophageal reflux (GOR), although their parents may call it ‘vomiting’. Parents require reassurance of the benign nature of this condition and the tendency for it to be ‘outgrown’ by 12 to 18 months of age. GOR becomes pathological (GOR disease [GORD]) and requires treatment only when the infant has failure to thrive, haematemesis, poor feeding or pulmonary aspiration.4
Children and adolescents may present with rumination syndrome. This is distinct from vomiting in that there is repeated, nonforceful regurgitation of gastric contents into the mouth. The material may then be spat out or swallowed. Both the child and parents may refer to this as ‘vomiting’ but it is important to make the distinction. Usually there is no pain, preceding nausea or other symptoms and the child does not lose weight or become dehydrated, despite rumination occurring many times each day (usually soon after eating or drinking). Rumination syndrome is a functional gastrointestinal disorder that is thought to be a subconscious habit and responds to behavioural management strategies such as distraction and diaphragmatic breathing.5
Vomiting associated with difficulty swallowing or drooling can occur in young children who have ingested foreign bodies in the oesophagus. An oesophageal button battery is a medical emergency due to the risk of perforation or fistulisation to the aorta or trachea, which can occur within hours.6 Urgent referral to hospital for immediate x-ray followed by endoscopic removal (if found) is required.
Food protein-induced enterocolitis syndrome typically presents in infants at about 6 months of age when first exposed to new food antigens. It presents with profuse vomiting, lethargy and pallor, and sometimes, diarrhoea.7 Immunoglobulin E-mediated food allergies can manifest with profuse vomiting in children, but these are usually associated with other symptoms or signs such as flushing, urticarial rash, pruritis or respiratory tract symptoms.
Neurological and psychological causes
Raised intracranial pressure always needs to be considered as a cause of vomiting. Typically, the vomiting occurs early in the morning, and may be associated with other neurological symptoms. Acute onset of fever, drowsiness and nuchal rigidity suggests meningitis. Subacute or gradual onset of unsteady gait, headache, personality change or irritability, eye signs (e.g. nystagmus) and developmental regression can all occur with intracranial tumours. A history of recent head injury should prompt consideration of an intracranial haematoma.
Cyclical vomiting syndrome is characterised by repeated bouts of stereotyped severe vomiting lasting hours to days (often causing dehydration) with intervening periods of normal health.8 These children are often of primary school age and there may be a prodrome of pallor and profound lethargy, and a family history of migraine. The diagnosis is made by careful history taking and recognition of a recurring pattern with relevant investigations to exclude other causes, particularly since bile-stained vomiting and abdominal pain is frequently present. Anxiety can mediate nausea and vomiting, which is usually situational (e.g. when confronted with situations or thoughts that are unpleasant or distressing). Purging associated with bulimia nervosa should be considered in chronic vomiting in older children and adolescents.
Systemic causes
The chemoreceptor trigger zone is a unique area of the brainstem that is not protected by the blood-brain barrier, so it is exposed to circulating drugs, toxins, cytokines and other chemicals. A medication history (including complementary and alternative therapies) is therefore important. Antibiotics such as erythromycin, NSAIDs, opiates, anticonvulsants, antiarrhythmics, oral contraceptives commonly prescribed for acne or menstrual cycle control and azathioprine are the more common medications used in children that are associated with nausea or vomiting. Of course, some of these medications may cause nausea or vomiting by actions outside the chemoreceptor trigger zone (e.g. NSAIDs causing gastrointestinal irritation), therefore it is convenient to remember ‘medications’ as under the category of systemic causes.
Taking a recreational drug history in adolescents is also important as chronic cannabis use (and withdrawal) can result in nausea and vomiting. Remember that adolescent girls may have an undiagnosed pregnancy, which could present initially with hyperemesis.
Systemic infections in children as diverse as self-limiting viral illnesses and serious bacterial infections can all result in vomiting. In young children, localising symptoms of sepsis may be confusing, for example:
- pneumonia or urinary tract infections may present with abdominal pain rather than cough or dysuria
- a septic joint may present with refusal to walk
- meningitis may present with floppiness and no ‘meningism’
- bacteraemia may present with no localising signs.
Metabolic illnesses (e.g. type 1 diabetes) can present with vomiting and are usually accompanied by polyuria, polydipsia and weight loss. Inborn errors of metabolism are uncommon but can present with intermittent profuse vomiting and mimic cyclical vomiting syndrome. Clues to these conditions include developmental delay, epilepsy, encephalopathy during the vomiting spells, or spells that are precipitated by fasting or high-protein meals.9 These infants and children are often sick enough to present to hospital, where blood tests show acidosis or hypoglycaemia that leads to further investigation.
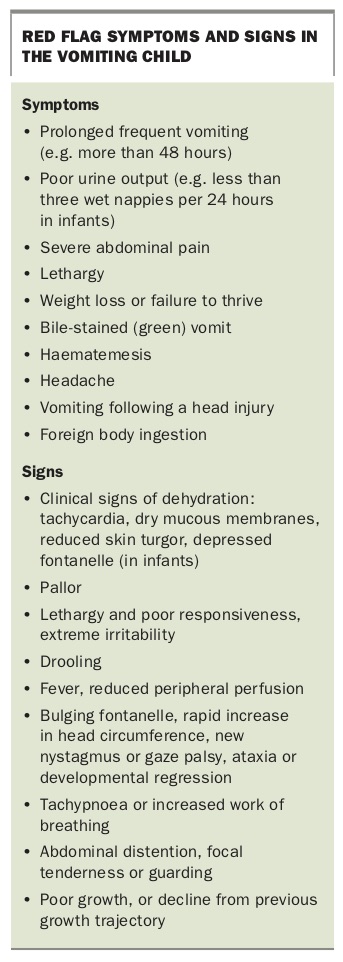
Red flag symptoms and signs
Important presenting symptoms or signs that should alert the GP to consider a serious underlying illness that requires prompt or emergency referral are outlined in the Box.
{kind=link}
Assessment of hydration
After consideration of differential diagnoses, a clinical assessment of the hydration status of the vomiting child is required. Thirst and reduced urine output are the earliest signs of dehydration so enquiring about the number of wet nappies in the past 24 hours or when the child last urinated is helpful.
Infants and children with mild dehydration usually have no signs or symptoms. Those with moderate dehydration will have slightly reduced peripheral perfusion (demonstrated by prolonged capillary refill time of more than two seconds), increased respiratory rate and mildly reduced tissue turgor. Those with severe dehydration will have markedly prolonged capillary refill time (more than three seconds), mottling, signs of shock (such as tachycardia and lethargy), deep acidotic breathing and markedly reduced tissue turgor.10,11 Infants and children with severe dehydration require hospitalisation. Acute changes in body weight can also indicate degree of dehydration if recent weight measurements are available.
Investigations and referral
Infants and children with acute presentations usually either require:
- no investigations, because they are suspected to have a benign cause such as acute gastroenteritis with no red flag signs or symptoms, or
- urgent investigation, which is best done after referral to hospital.
In remote or rural settings, the GP may need to administer parenteral antibiotics for suspected sepsis before transport or retrieval to hospital. Blood and other cultures (e.g. urine) should be collected (where possible) before antibiotic administration, but their collection should not cause undue delay.
Patients with suspected surgical conditions or an oesophageal foreign body should be urgently referred to a hospital that has paediatric surgical or gastroenterology expertise. In most cases, investigations such as imaging are best performed in hospital.
Patients with subacute presentations can be investigated and reviewed by the GP before referral if a more chronic disease process is suspected. Such investigations are guided by history and examination. For example, vomiting with weight loss, diarrhoea and abdominal pain in an older child warrants stool cultures, a full blood count, iron studies, inflammatory markers and coeliac serology. Ultrasound of the abdomen can be helpful in diagnosing suspected gallstones, uretero-pelvic junction obstruction or subacute appendicitis. Urine or serum measurement of human chorionic gonadotropin levels should be considered in adolescent girls who have vomiting without a clear cause.
Some suspected conditions, such as rumination syndrome, anxiety-induced vomiting, bulimia nervosa or acute viral gastroenteritis often require no investigations but may need referral to a paediatrician if a diagnosis cannot be confidently made.
Conclusion
Vomiting in children is a nonspecific symptom, and the differential diagnoses are broad. An awareness of the principal mechanisms of vomiting (considering the systemic, abdominal and neurological/ psychological causes), a careful history and examination (looking for red flag symptoms or signs) and consideration of important life-threatening causes will assist the GP to make a thorough assessment of the vomiting child. In particular, bile-stained vomiting, severe abdominal pain, neurological symptoms and signs of sepsis mandate immediate referral to a hospital that has paediatric support. MT