Anal disorders – haemorrhoids, abscesses and fissures

Anal disorders are a common presentation to general practice and can be distressing for patients. Common disorders include haemorrhoids, anorectal abscesses or fistulas and anal fissures. For some patients, management can involve simple strategies and reassurance; however, others, particularly when in the presence of red flags, require specialist assessment and further investigation.
- Perianal disorders are common and have a significant impact of the patient’s quality of life.
- Fissures, perianal abscesses and haemorrhoids can often be distinguished based on the patient’s history of presenting complaint.
- Most anal disorders are benign but neoplastic causes of the symptoms should be excluded with physical or endoscopic examination.
- GPs can provide reassurance to patients with benign conditions and should identify red flags that require early definitive care by a surgeon.
- Referral to a surgeon is indicated in patients with advanced pathology or who are not responsive to non-surgical treatments.
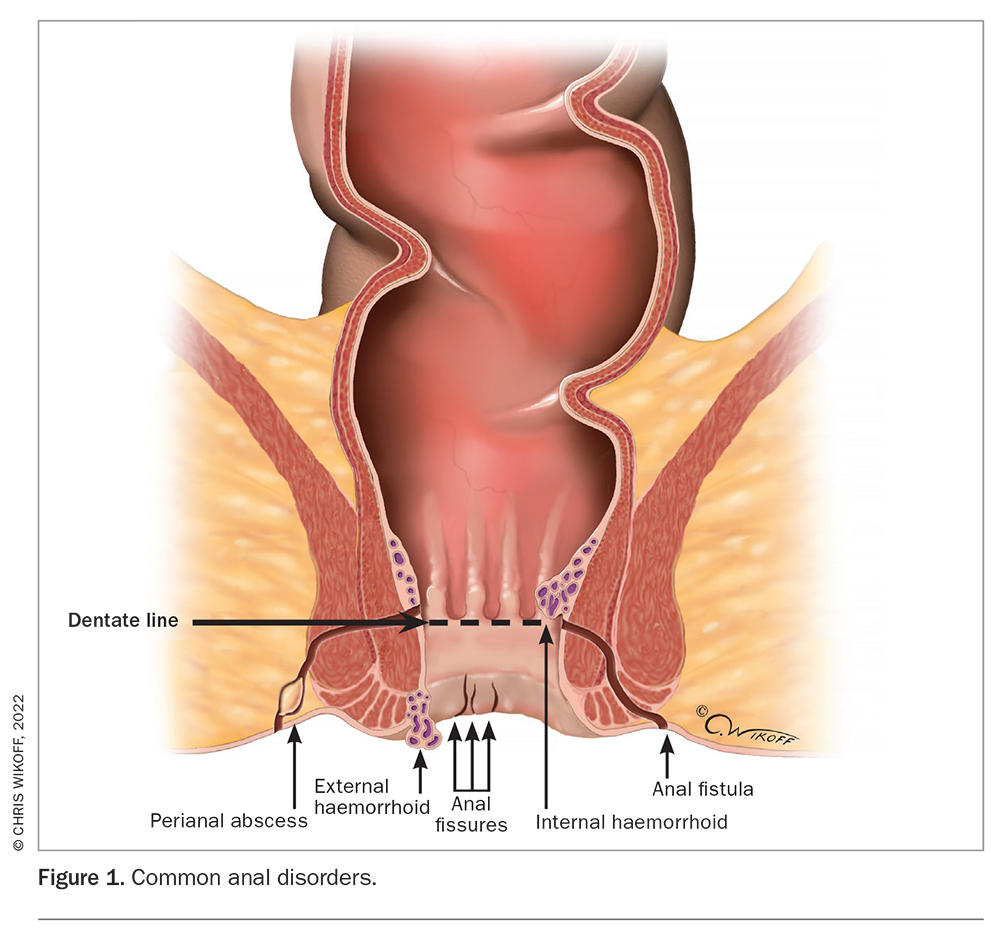
Anal disorders affect one-third of the Australian population, particularly middle- to older-aged individuals, with a similar incidence between men and women.1 Anal disorders can be debilitating and have a significant impact on a patient’s quality of life. This article focuses on the most common anal disorders that frequently cause anal irritation and pain: haemorrhoids, anorectal abscesses and fistulas, and anal fissures (Figure 1).
{kind=link}
Haemorrhoids
The haemorrhoidal plexus is a normal anatomical structure, located at the upper anal canal. It is important to recognise that haemorrhoid plexi are essentially the rectal veins forming a plexus.2 In the condition known as haemorrhoids, these vascular cushions (typically in the left lateral and right anterior and posterior positions), become distended and enlarged, which can result in prolapse or typically painless bleeding.2
Risk factors for the development of haemorrhoids include constipation and straining, especially if this results in prolonged periods sitting on the toilet; ageing; pregnancy; obesity; and heavy lifting.3 These risk factors result in fragmentation of connective tissue, combined with increased intra-abdominal pressure, with reduced venous return and an engorged haemorrhoidal plexus.3
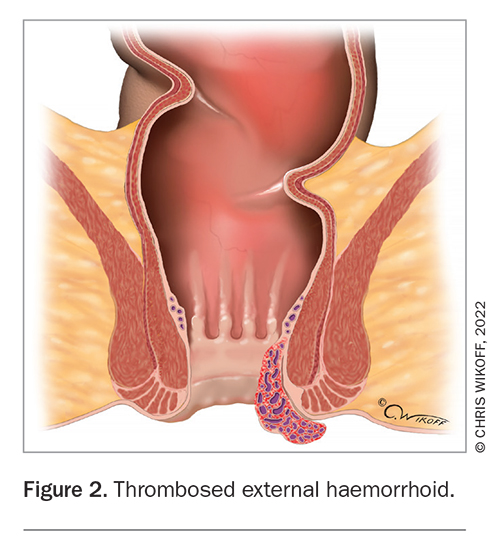
There are two types of haemorrhoids: internal and external, depending on their location in relation to the dentate line (also known as pectinate line). The dentate line approximates the level of change in the epithelium within the anal canal.3 Embryologically, anything above the dentate line is endoderm in origin and anything below it is ectoderm in origin. Above the dentate line, pain tends to be diffuse and poorly localised.3,4 Below the dentate line, the pain is more readily localised.3,4 The signs and symptoms differ between internal and external haemorrhoids. Internal haemorrhoids are generally painless, but patients can also experience the feeling of rectal fullness or discomfort and mucous discharge.4 External haemorrhoids may be painful and can cause sudden severe perianal pain with a sensation of a perianal mass.4 Additionally, there can be pain on defecation, particularly if thrombosis occurs within the external haemorrhoids, more accurately known as thrombosed external haemorrhoids or perianal haematoma (Figure 2).
{kind=link}
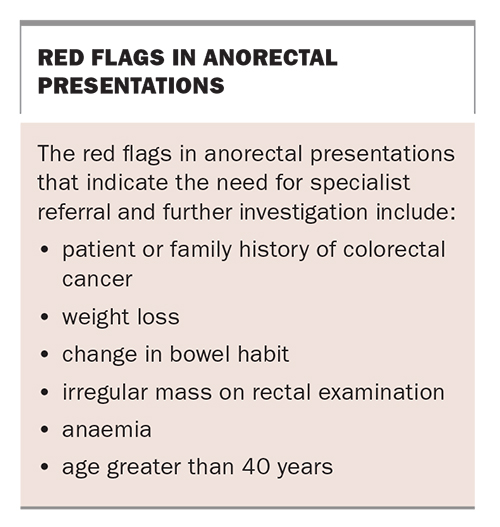
If the patient presents with rectal bleeding, neoplastic lesions should be excluded. The history should include evaluation for the presence of risk factors for colorectal cancer, such as family history, change in bowel habit and weight loss (Box). If the patient reports perianal pain, anal fissures or abscesses should also be considered.5 Patients are typically examined in the left lateral position. Haemorrhoids are maximally engorged when sitting, causing the patient to be symptomatic while sitting on the toilet but not during clinical examination because of patient positioning. On general inspection, external haemorrhoids may be visible. Assessment of internal haemorrhoids should include asking the patient to bear-down or strain as this can make haemorrhoids more prominent. Internal haemorrhoids are not palpable on digital rectal examination.5 A proctoscope is useful to visualise any internal haemorrhoids.
{kind=link}
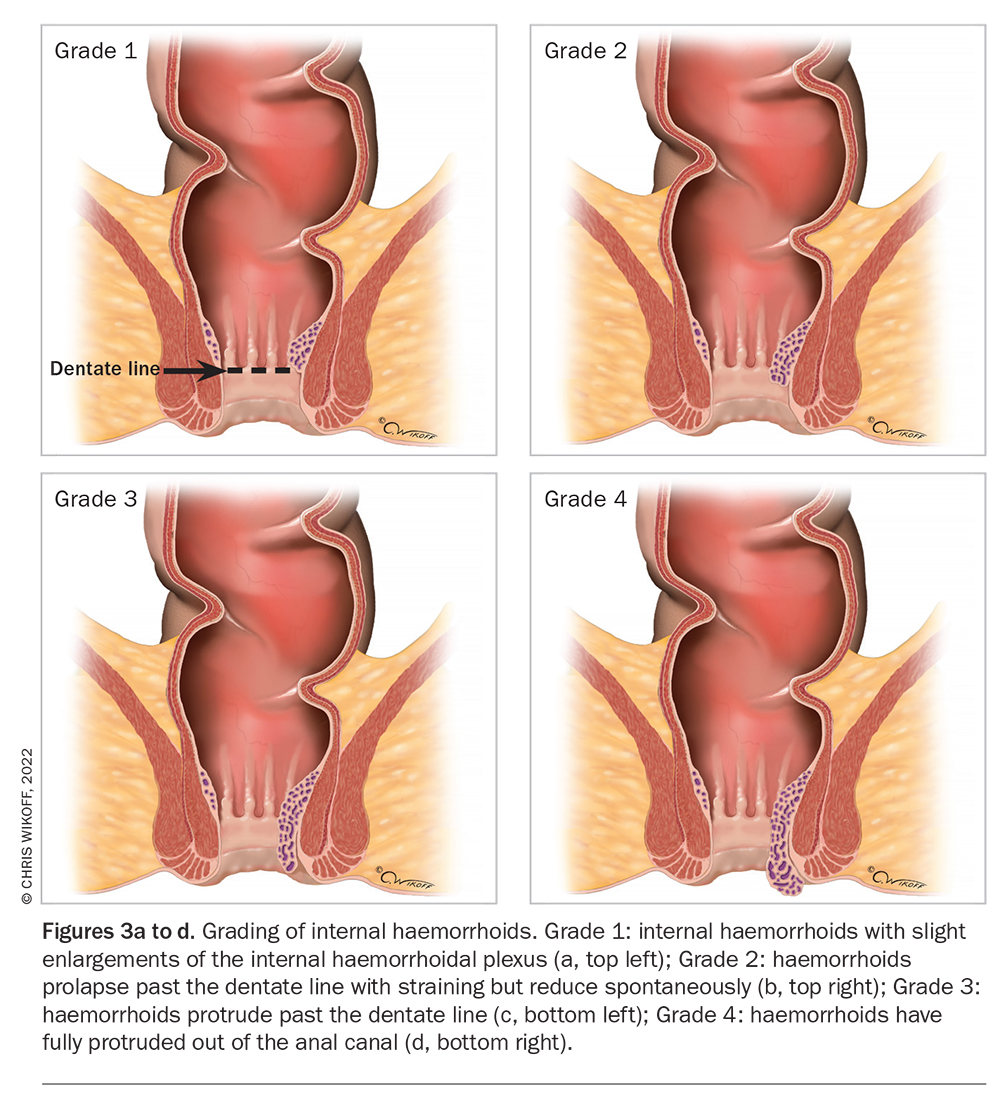
Internal haemorrhoids can be classified as Grade 1 to 4 (Figures 3a to d). The grade helps guide treatment selection but may not reflect the severity of symptoms.5,6 Grade 1 haemorrhoids are defined as slight enlargements of the internal haemorrhoidal plexus.6 Grade 2 haemorrhoids prolapse past the dentate line with straining but reduce spontaneously.6 Grade 3 haemorrhoids protrude past the dentate line and are visible in the anal sphincter, and must be manually reduced.6 Grade 4 haemorrhoids have fully protruded out of the anal canal and cannot be reduced.6
{kind=link}
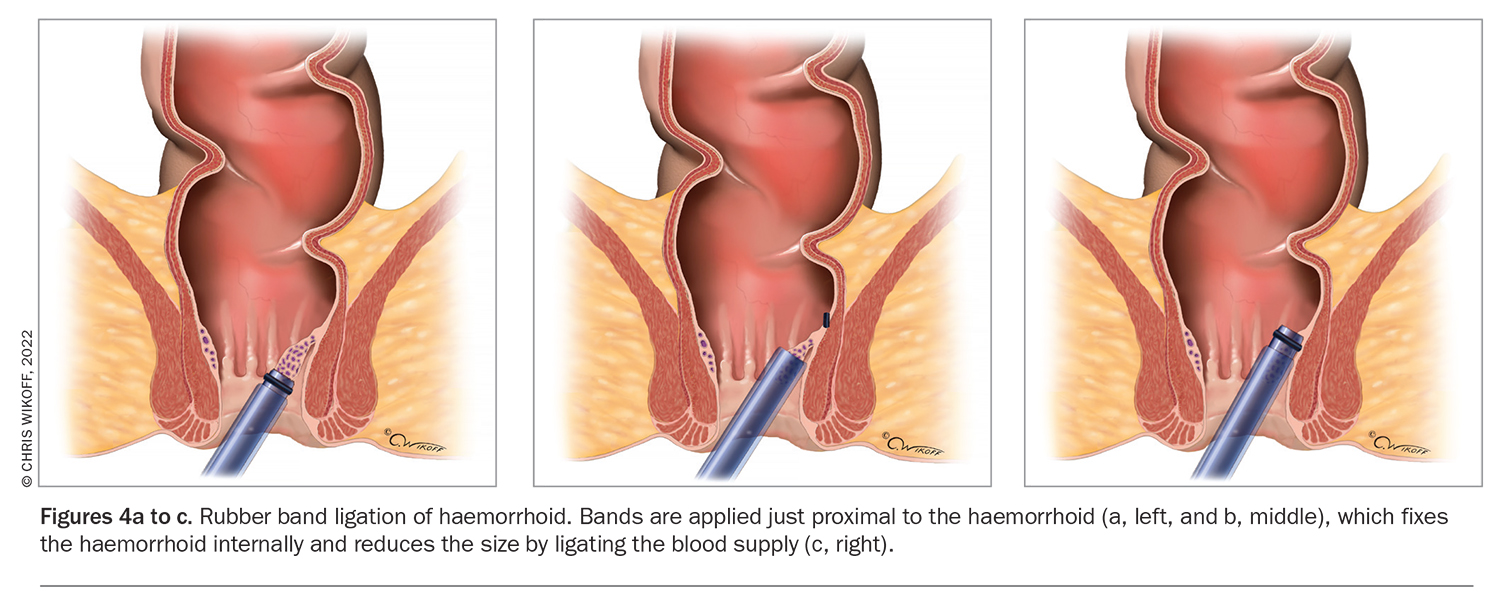
The initial treatment for external and internal haemorrhoids of Grade 1 and 2 focuses on optimising bowel function with soluble fibre supplements (e.g. sterculia), aperients (e.g. regular macrogol laxatives or lactulose) to avoid constipation and straining, increasing water intake to 2 to 3 L per day and avoiding long periods sitting on the toilet.7 Doses of soluble fibre and laxatives need to be titrated to achieve a soft but formed stool (Bristol Stool Chart Type 4). Sitz baths and topical steroids are not supported by evidence.7,8 Many patients improve with these measures; however, if symptoms persist, rubber band ligation should be considered (Figures 4a to c).
{kind=link}
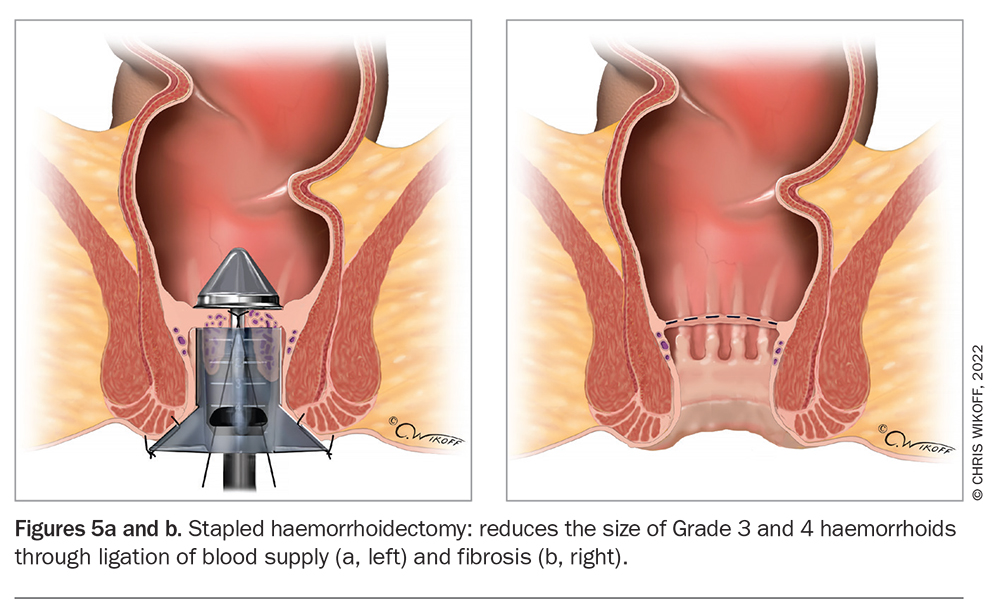
For Grade 3 and 4 haemorrhoids, surgical options include Doppler-guided haemorrhoid artery ligation and haemorrhoidopexy or haemorrhoidectomy (excision or stapled) (Figures 5a and b).9 Haemorrhoid artery ligation, haemorrhoidopexy and stapled haemorrhoidectomy reduce the haemorrhoid size by ligating the blood supply and reduce the haemorrhoidal tissue through fibrosis.9 Excision haemorrhoidectomy, as the name suggests, involves excising redundant haemorrhoidal tissue and ligating the haemorrhoid pedicle. All procedures can be done as a day procedure and are very effective in preventing further formation of haemorrhoids, with success rates of 93% for stapled haemorrhoidectomy, 92% for haemorrhoidopexy and 85% for excision haemorrhoidectomy.9 Patients should be counselled that they will experience two to four weeks of postoperative pain, as well as intermittent rectal bleeding for 24 to 48 hours.9,10
{kind=link}
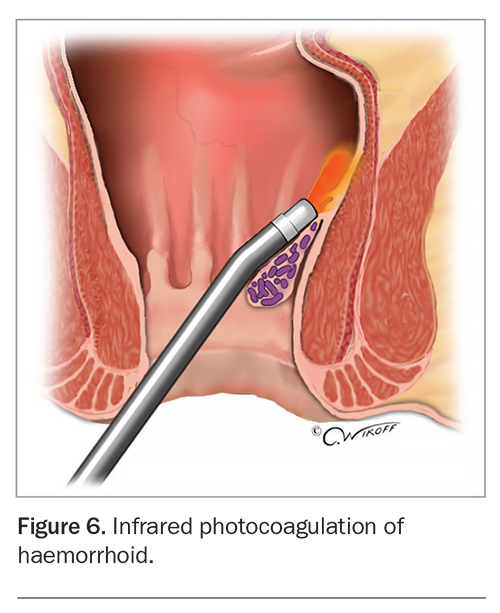
Newer and relatively novel treatment options include photocoagulation, where infrared light is used to break down the haemorrhoids by thrombosis and scar formation (Figure 6).9 It is effective for small- to medium-sized haemorrhoids, with a 60 to 85% success rate.10 A caveat is that only one haemorrhoid can be treated at a time and other haemorrhoids may be treated at 10- to 14-day intervals.10
{kind=link}
Thrombosed external haemorrhoids should be treated by evacuating the thrombosis. This can often be performed using local anaesthetic in consulting rooms. However, if there are signs of sepsis, patients should be referred urgently to the emergency department for anal examination under anaesthesia and incision or excision of the thrombosed external haemorrhoids. After drainage, patients should be prescribed oral metronidazole for seven days, which can reduce inflammation by twofold and provide symptomatic relief.11
Anorectal abscesses and fistulas
Anorectal abscesses are thought to originate from an infected anal crypt gland.12 Anal crypt glands are tiny mucous glands situated along the dentate line that provide lubrication to aid defecation. Contraction of the anal sphincter muscles stimulates the crypts to produce mucous. About 90% of perianal abscesses originate from these crypts.12 Bacteria spread via the crypts through the anal duct and infect the glands, resulting in abscess formation.12,13
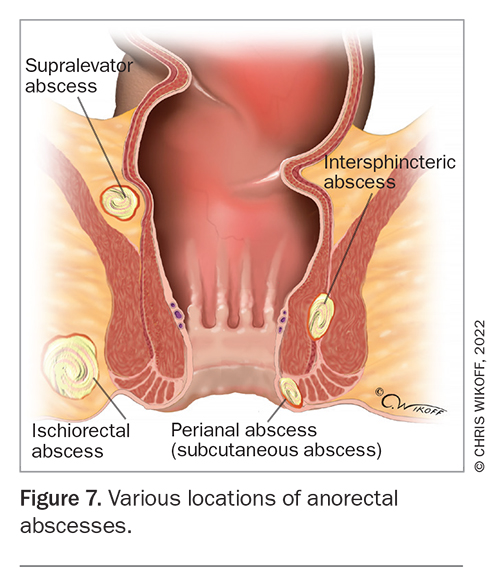
Anorectal abscesses can be deep or superficial and can occur in four areas (Figure 7). The most common are perianal abscesses, which occur just below the perianal skin and are confined to the superficial subcutaneous region.14 The second most common type is an ischiorectal abscess, which is located in the ischiorectal space.14,15 Supralevator abscesses are uncommon and are located above the levator ani muscle.14 If the abscess forms between the internal and external anal sphincters, it is known as an intersphincteric abscess.14 Posterior intersphincteric abscesses may transverse the deep postanal space bilaterally, forming a horseshoe abscess.14
{kind=link}
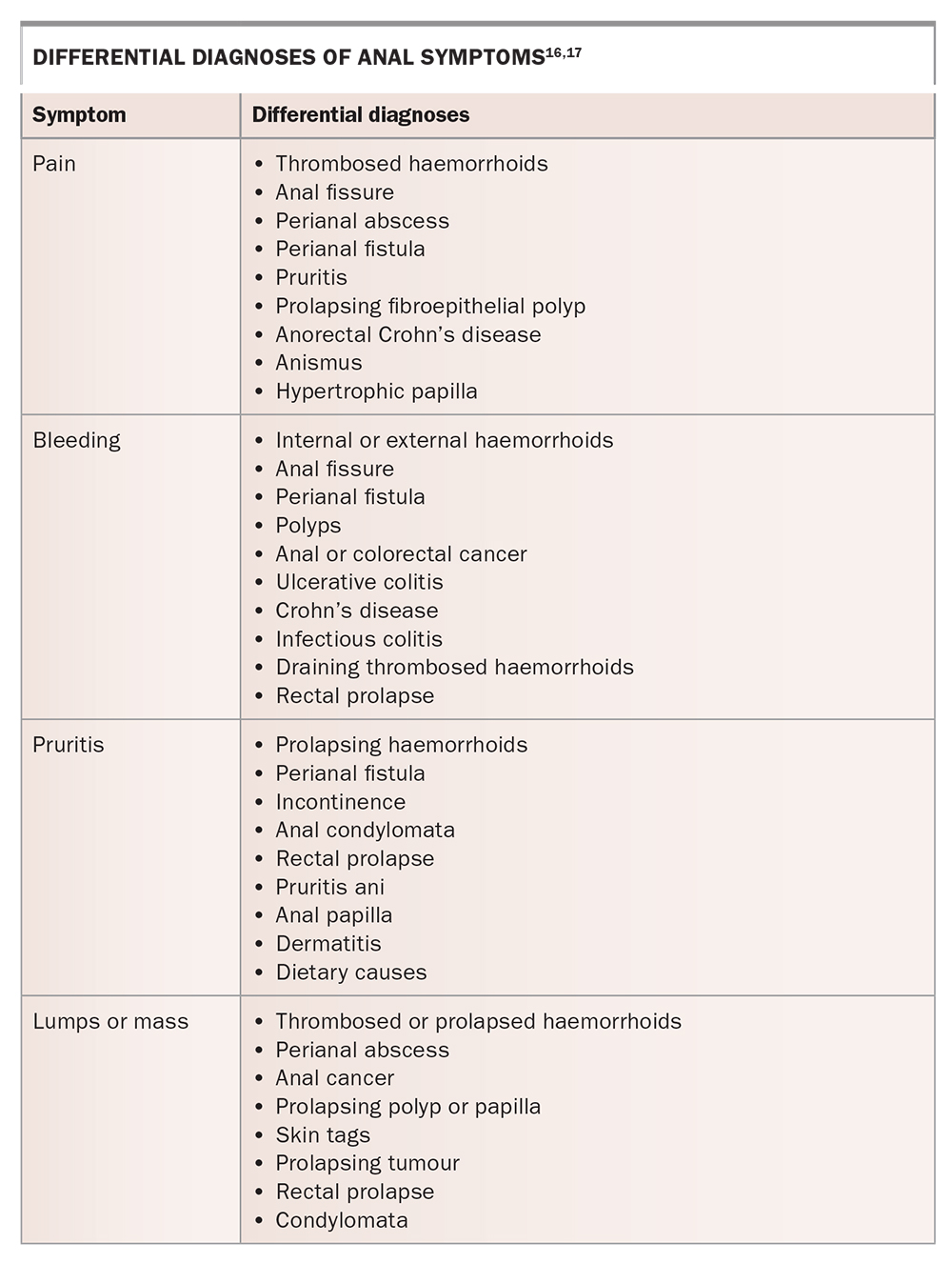
Anorectal abscesses typically present with constant anal pain and, unlike anal fissures, the pain is usually not associated with bleeding.14 Patients can also experience systemic symptoms such as fever and malaise.14,15 The diagnosis of an anorectal abscess can be made by clinical history and examination. On examination, a fluctuance to or a patch of erythema on the skin within the buttock area may be found. Deep ischiorectal abscesses may not be obvious on inspection, although induration at the site of pain can indicate a deep abscess. If skin changes are absent, a palpable boggy swelling just above the anorectal junction on digital rectal examination may suggest a supralevator abscess.15 Inflammatory markers are usually elevated. Imaging is not routinely required; however, if there is a high index of suspicion and the clinical examination is unremarkable, a CT pelvis can be considered.16 Patients with diabetes or who are immunosuppressed have a higher risk of developing soft tissue infection, such as necrotising fasciitis.16 This can progress rapidly and such patients should be referred for early surgical review. The differential diagnoses for anorectal abscesses and anal symptoms are listed in the Table.16,17
{kind=link}
The management of an anorectal abscess is drainage, using either general or local anaesthetic.16,18 The role of antibiotics in the initial or as the sole management of anorectal abscesses is controversial. Antibiotics may be used to treat small abscesses (1 to 2 cm); however, there is a risk of recurrence and a fistula may still develop.18 Complications of anorectal abscesses include the spread of infection to other tissues, sepsis and development of an anal fistula.18 Oral metronidazole after abscess drainage reduces the risk of an anal fistula developing by twofold.18
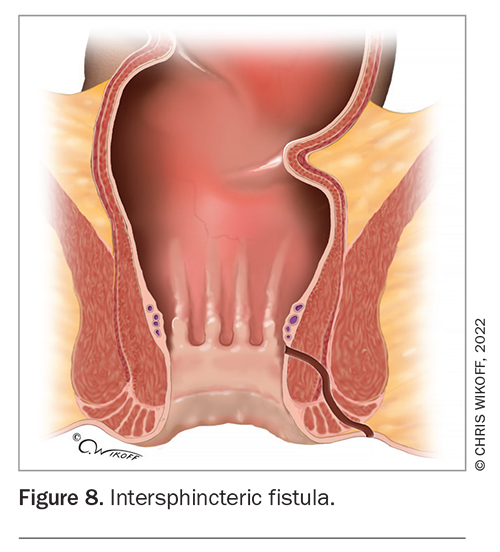
An anal fistula is the development of a small tunnel that connects the perianal skin to the anus (Figure 8).18 About 50% of patients develop an anal fistula after anorectal abscess drainage.19 If the fistula persists, a seton may need to be inserted to prevent recurrent abscesses.19 A seton is a thin piece of silastic or suture that is placed through the entire fistula tract, forming a ring around the anus involving the fistula tract.19 The seton acts as a drain and facilitates planning of a definitive fistula treatment. An MRI scan is usually performed to assess the amount of sphincter involved, which will determine the safest procedure.19
{kind=link}
There are multiple options for definitive treatment of an anal fistula, perhaps indicating that there is no ‘gold standard’ treatment. The surgical options include fistulotomy, mucosal advancement flap, ligation of the intersphincteric fistula tract procedure, over-the-scope clips, video-assisted anal fistula treatment and fistula laser closure.20 All the procedures can be done as a day procedure and the documented rate of success varies between procedures: 90% for fistulotomy, 60 to 70% for ligation of the intersphincteric fistula tract procedure and mucosal advancement flap, and about 50 to 80% for over-the-scope clips and video-assisted anal fistula treatment.21 Although fistulotomy is the most effective treatment, it is only suitable for low or intersphincteric fistulas, where less than 30 to 50% of anal muscle is involved.21
Anal fissures
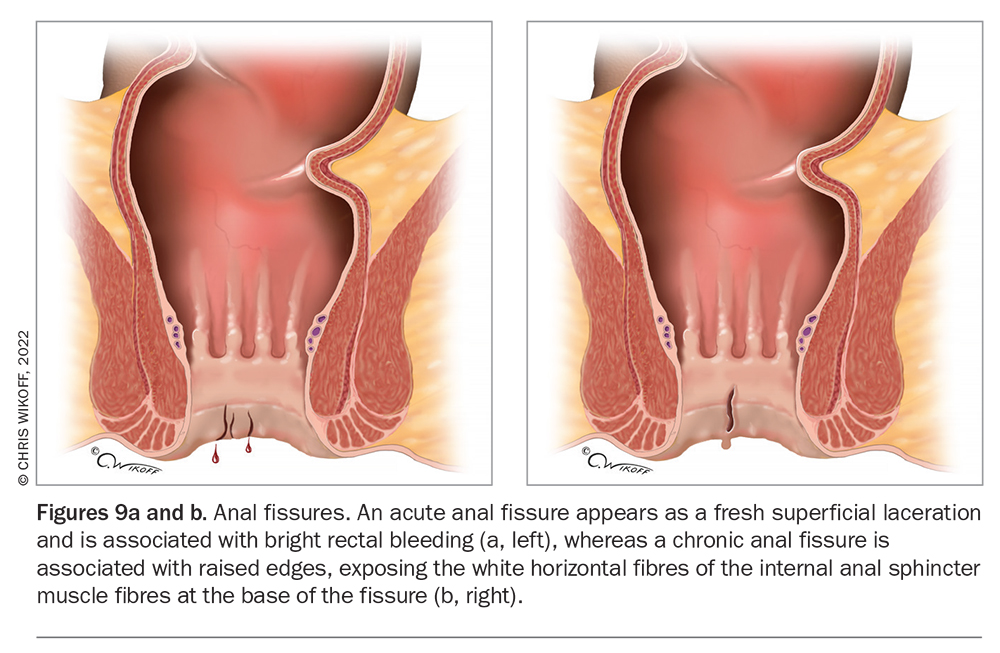
An anal fissure is a longitudinal tear of anoderm distal to the dentate line, exposing the internal anal sphincter (Figures 9a and b).22 About 90% of anal fissures are located in the posterior midline of the anal canal and are caused by local trauma, such as constipation, diarrhoea and, less commonly, anoreceptive intercourse.23 If the fissure is located laterally, it may indicate a secondary aetiology, such as Crohn’s disease, malignancy, communicable diseases (e.g. HIV, chlamydia or syphilis) and other granulomatous diseases (e.g. sarcoidosis and extrapulmonary tuberculosis).23
{kind=link}
Anal fissures may be distinguished from haemorrhoids and abscesses by eliciting a history of anal pain that is constant at rest and exacerbated by defecation, often lasting for hours and is debilitating for the patient.23 The pain is classically associated with bright rectal bleeding.
Anal fissures can be misdiagnosed as haemorrhoids. Physical examination of the patient with a suspected anal fissure involves retracting the gluteal cheeks apart and carefully examining the posterior midline.23 The presence of a sentinel skin tag in the posterior location suggests an underlying fissure.23,24 The distal end of the fissure may only be apparent when the patient bears down. Digital rectal examination is often too painful for the patient. An acute fissure appears as a fresh superficial laceration, much like a paper cut, whereas a chronic fissure has raised edges, exposing the white horizontal fibres of the internal anal sphincter muscle fibres at the base of the fissure (Figures 9a and b).24
Follow-up examinations should be performed when the patient is more comfortable to exclude secondary causes of an anal fissure, such as malignancy.24 A flexible sigmoidoscopy should be considered for patients older than 40 years without any family history of colon cancer. For older patients or those with risk factors for malignancy, a full colonoscopy should be offered.24 Additionally, patients with atypical (lateral) fissures or clinical features of underlying Crohn’s disease should undergo colonoscopy.23-25
The initial management of an anal fissure is topical nitroglycerin or 2% nifedipine ointment, applied three times per day for one month.26 This will result in healing in 60 to 70% of cases.26 The patient should be advised to use gloves when administering topical nitroglycerin or nifedipine as these treatments can cause headache (secondary to vasodilatation) and, in the worst case scenario, syncope in up to 14% of patients.26 Additionally, soluble fibre supplements (e.g. psyllium), topical analgesics (e.g. lidocaine gel), stool softener or laxatives (e.g. macrogol supplements, lactulose, docusate with senna) can be used to optimise bowel function and stool consistency.26 If initial medical therapy fails, surgical management should be considered.26,27 Surgical management options include sphincterotomy, botulinum toxin injection and, less commonly, fissurectomy and anal advancement flap.27 Botulinum toxin injection provides reliable relaxation of the internal sphincter for three to six months and can be performed without an anaesthetic.27 There is a risk of flatus incontinence in about 5% of patients; however, this usually resolves when the botulinum toxin wears off in about three to six months.27,28 The success rate of botulinum toxin injection is up to 85%.28
Lateral sphincterotomy is now reserved for patients with a fissure that persists after treatment with botulinum toxin injection and who have a low risk of incontinence.29 The rate of fissure healing reported in the literature for this procedure is about 95%.29 Patients with a high risk of incontinence should consider botulinum toxin injection, followed by subcutaneous fissurectomy and then a V-Y advancement flap.30 Subcutaneous fissurectomy and V-Y advancement flap are not commonly performed for fissures but are reserved for cases that are resistant to repeated botulinum toxin injection and in instances where lateral sphincterectomy is not appropriate due to the risk of incontinence.30
Conclusion
Patients presenting with anal pain require an accurate diagnosis to guide management. GPs play an important role in the early management of anal pathology. GPs can provide reassurance to patients with benign conditions and should identify red flags that require early definitive care by a surgeon. Referral to a surgeon is indicated in patients with advanced pathology or who are not responsive to non-surgical treatments. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.