Dysphagia – an updated guide to investigation

Dysphagia, or difficulty swallowing, is a common presentation in general practice. Taking a thorough history to establish the presence of true dysphagia and identify particular characteristics can help narrow the differential diagnoses and guide investigations and specialist referral. A multidisciplinary approach to management is recommended and should include gastroenterologists, dietitians, speech pathologists, ENT surgeons and upper gastrointestinal surgeons.
Dysphagia is defined as a subjective difficulty in the passage of a food bolus from the oral cavity to the stomach – put simply, a difficulty swallowing.1 It is a common presenting complaint in primary practice, with 15 to 30% of patients with symptoms related to dysphagia presenting to their GP.2,3 This article provides an updated guide to differentiating features in the patient history, appropriate first-line investigations and referrals, as well as initial management strategies for patients presenting with dysphagia, focusing predominantly on oesophageal dysphagia.
Aetiology
Dysphagia can be classified according to the location, along the oesophageal tract. Oropharyngeal dysphagia is the difficulty in initiating a swallow, whereas oesophageal dysphagia is the sensation of food being stuck in the neck and/or chest. These should be distinguished from odynophagia (painful swallowing) and globus sensation (the persistent or intermittent sensation of something being stuck in the back of the throat but which does not impair swallowing). The latter is often present between meals and the sensation alleviated by eating.1,4 Key steps to assessing symptoms of dysphagia are presented in the Flowchart.
History
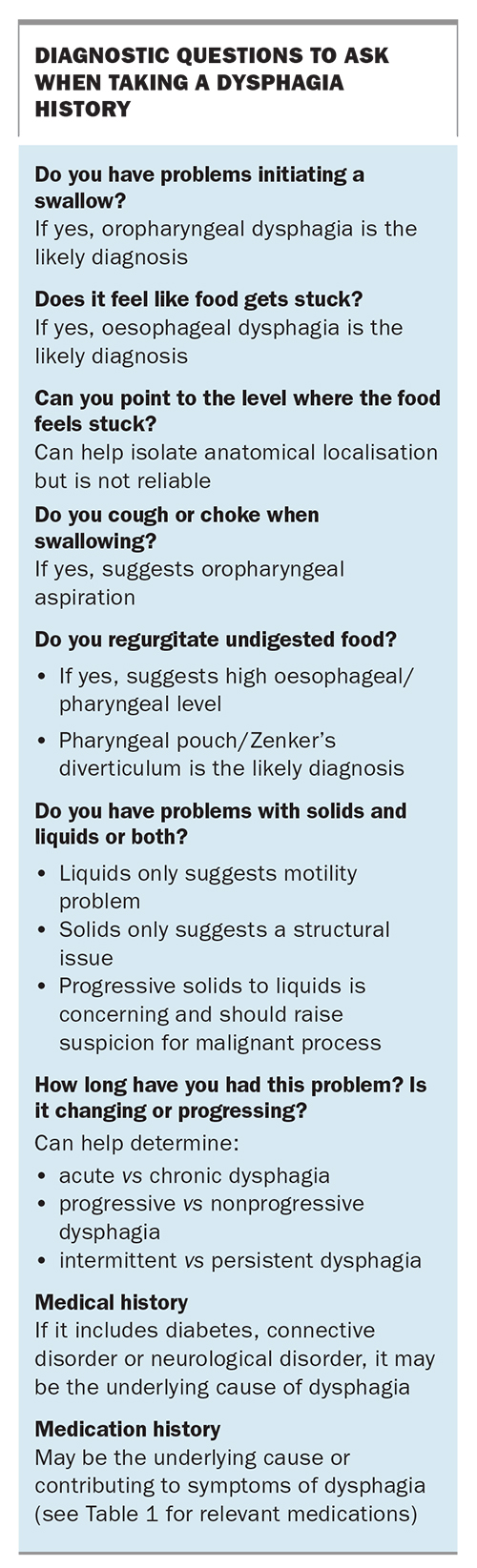
The aim of taking a history is to distinguish dysphagia from other aetiologies, such as globus sensation, to determine if true dysphagia is present. A thorough history can help identify the ‘level’ of dysphagia, that is, whether it is oropharyngeal dysphagia or oesophageal dysphagia, and the likely underlying cause (i.e. a structural cause or motility disorder). Determining the duration and frequency of symptoms can help distinguish acute dysphagia from chronic, and progressive dysphagia from intermittent. Careful questioning to elicit this information can help delineate the underlying cause of dysphagia and inform further investigation and referrals. A summary of key diagnostic questions to ask a patient about their symptoms is presented in the Box.
{kind=link}
Age and sex
The age and sex of the patient can be helpful in narrowing the differential diagnosis as particular aetiologies are more common in different groups. For example, a number of studies have shown that eosinophilic oesophagitis is present in around 10 to 12% of patients presenting with oesophageal dysphagia.5,6 In addition, a US study found that 55.8% of patients with eosinophilic oesophagitis had dysphagia, and eosinophilic oesophagitis was twice as prevalent in men than women, peaking at age 35 to 39 years.7 Achalasia as the underlying mechanism for oesophageal dysphagia is equally prevalent in both men and women, generally aged 25 to 60 years.8 Although older patients often attribute dysphagia to ‘getting old’, physicians should be vigilant for underlying malignancy or neurological events taken in the context of the individual patient’s risk profile. Ageing itself does not usually explain new-onset dysphagia in the elderly.9
Coughing, choking, regurgitating
Coughing, choking and regurgitation are symptoms of oropharyngeal dysphagia. A sudden onset of these symptoms may suggest an acute neurological cause such as a cerebrovascular event, whereas more gradual onset may suggest an underlying myopathic or neurodegenerative cause such as myasthenia gravis, motor neurone disease or Parkinson’s disease. A thorough clinical history and examination can help identify other features of these conditions. Further investigations, such as brain or neck imaging with contrast CT or MRI, should be performed to help confirm or exclude an alternative aetiology. If a neurological or neurodegenerative cause is suspected, the patient should be referred to an appropriate specialist, such as a neurologist, speech pathologist or ENT specialist.
The following questions can help determine the presence of coughing, choking or regurgitation.
- Is there a delay in initiating a swallow?
- Do you regularly cough immediately after swallowing?
- Do you regurgitate food or fluid from the nose or mouth during swallowing?
- Do you have to swallow repeatedly to clear your throat?
Localising the sticking point
Asking patients to point to where they feel food is getting stuck can be helpful but is not entirely reliable to ascertain the precise location of dysphagia. Generally, retrosternal localisation suggests an oesophageal cause; however, localisation to the neck does not exclude an oesophageal cause.10
Solids, liquids or both?
Determining the type of foods – solids, liquids or both – that cause symptoms of dysphagia can help distinguish between motility disorders and structural causes. Dysphagia to both liquids and solids suggests a motility disorder such as achalasia, oesophageal spasm or peristalsis disorder.11,12 Additional features to suggest a motility disorder include regurgitation during and between meals and complaints of chest pain, which is often retrosternal in location, heavy or burning in nature and can be mistaken for cardiac chest pain or reflux and indigestion-type pain.
Structural causes of dysphagia occur when initial dysphagia to solids progresses to dysphagia to liquids. Rapidly progressive dysphagia over weeks or months with associated systemic symptoms such as weight loss is concerning and indicative of an oesophageal malignancy.13 More gradual progressive symptoms may suggest an inflammatory or fibrotic process such as a stricture from chronic reflux disease or oesophageal rings from eosinophilic oesophagitis. A more consistent, nonprogressive dysphagia to solids is suggestive of an anatomical variant such as oesophageal ring. Regurgitation of undigested food raises the suspicion of a structural lesion, such as a pharyngeal pouch or Zenker’s diverticulum, and consideration of a functional condition such as rumination syndrome.
Medical and medication history
Important additional aspects of the history include symptoms suggesting anaemia, such as fatigue or breathlessness, and unintentional weight loss in the past six to 12 months. A systematic review of symptoms relating to possible underlying neurological or connective tissue disease, such as Parkinson’s disease or systemic sclerosis, can be important. Oesophageal candidiasis can cause both dysphagia and odynophagia and is a potential differential diagnosis in patients with a history of diabetes mellitus or immunosuppression.
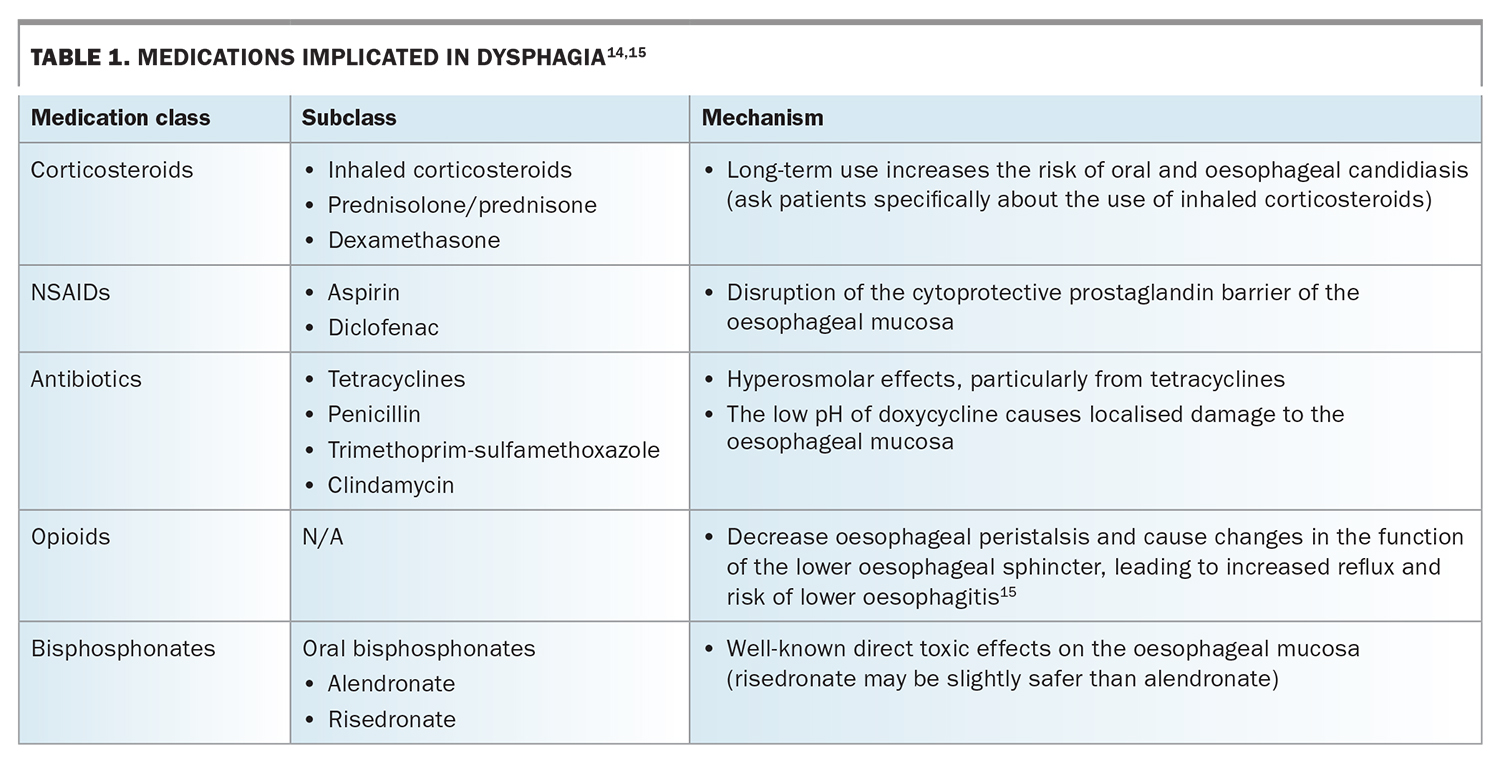
Taking a medication history is vital. Medication-induced oesophagitis is a well-recognised cause of dysphagia. The mechanisms include direct toxic insults to the oesophageal mucosa, such as acidic burns and the effects of hyperosmolar properties of medications, as well as disruption of protective factors.14 Medications that are implicated in dysphagia are listed in Table 1.14,15
{kind=link}
Investigations
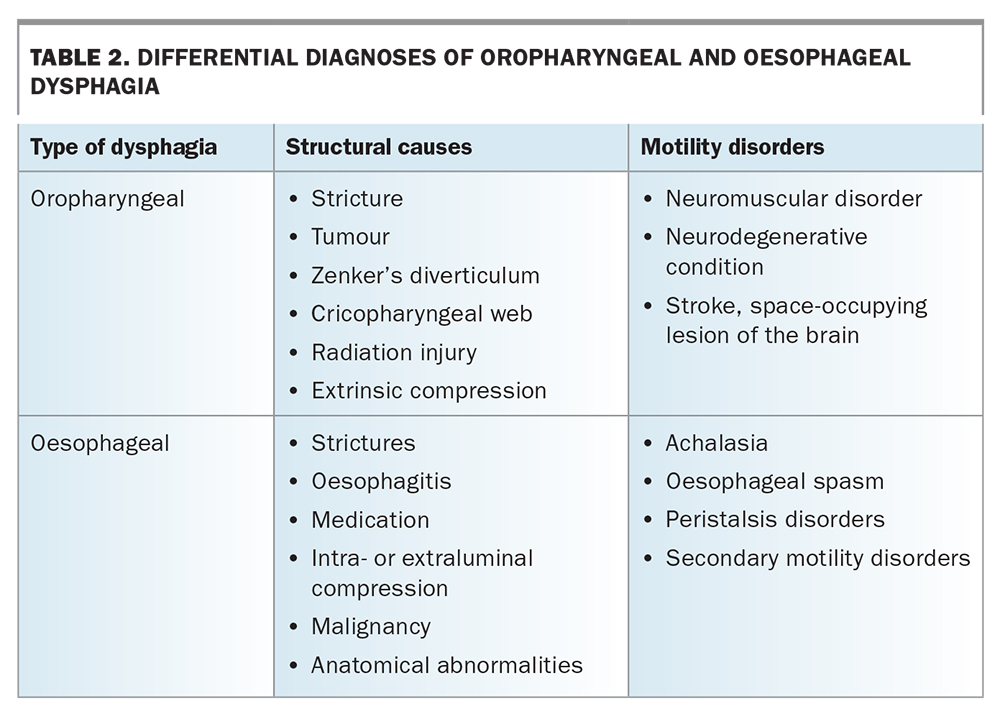
Once the characteristic symptoms of dysphagia have been identified, differential diagnoses can be made to help guide next steps for investigation and referral. Broadly speaking, both oropharyngeal and oesophageal dysphagia can be divided into structural or motility dysphagia and the differential diagnoses for each are listed in Table 2.3
{kind=link}
Oropharyngeal dysphagia
Video fluoroscopy (modified barium swallow)
Video fluoroscopy imaging is the gold standard for investigating oropharyngeal dysphagia.1,4 It provides real-time information about the oropharyngeal phase of swallowing and is often performed and reported by speech pathologists. It involves taking x-rays of the pharynx while a patient swallows barium contrast media of varying consistencies and reviewing the swallowing function. It can be used to guide pharyngeal rehabilitation and diet modifications to reduce pulmonary aspiration.1,3
Oesophageal dysphagia – structural cause
Gastroscopy
Gastroscopy should be the first-line investigation in most patients with a history suggestive of oesophageal dysphagia. Patients with red-flag symptoms of new-onset or rapidly progressive dysphagia, or progressive or new epigastric pain persisting for more than two weeks also require urgent investigation with gastroscopy.16 In patients with no red-flag symptoms and in whom reflux or dyspepsia is the major complaint, it is reasonable to first trial treatment with a proton-pump inhibitor (PPI) for four to six weeks. PPI use must be reviewed after this time or if symptoms change. If symptoms are unresolved or additional red-flag symptoms develop, the patient should be referred for gastroscopy. If symptoms have resolved during the PPI trial, treatment should aim to be withdrawn after eight weeks.4,17
A gastroscopy provides direct visualisation of the oesophageal tissue as well as allowing for biopsies to be taken and potential therapeutic options to be delivered.3,4,13 It is especially useful for the diagnosis of malignant and premalignant lesions, strictures, Barrett’s oesophagus and eosinophilic oesophagitis. Gastroscopy can also identify a physically obstructive cause of dysphagia.4,18,19
An urgent gastroscopy is required for patients presenting with acute-onset dysphagia, usually retrosternal with an associated history suggestive of a food bolus. Prior CT imaging should be considered if a history of pain raises the possibility of oesophageal perforation or complication – from primary practice, such a patient should be referred for urgent inpatient assessment by a gastroenterology team or be seen via the emergency department.4 A CT scan is also useful for excluding extrinsic factors that may be compressing the oesophagus as a cause for dysphagia, particularly in older patients in whom a gastroscopy investigation is normal.
Oesophageal dysphagia – motility disorder
Barium swallow
Although a modified barium swallow is the gold standard investigation for oropharyngeal dysphagia, a dedicated oesophageal barium swallow test can provide invaluable information in conjunction with a gastroscopy.10,11 This test involves taking x-rays of the entire upper gastrointestinal tract, from pharynx to lower oesophageal sphincter, after ingestion of barium contrast liquid or solid. The contrast visualised on x-ray can identify proximal lesions responsible for dysphagia, including pharyngeal pouch, Zenker’s diverticulum, postradiation injury, oesophageal rings or strictures, which may be missed during gastroscopy.11
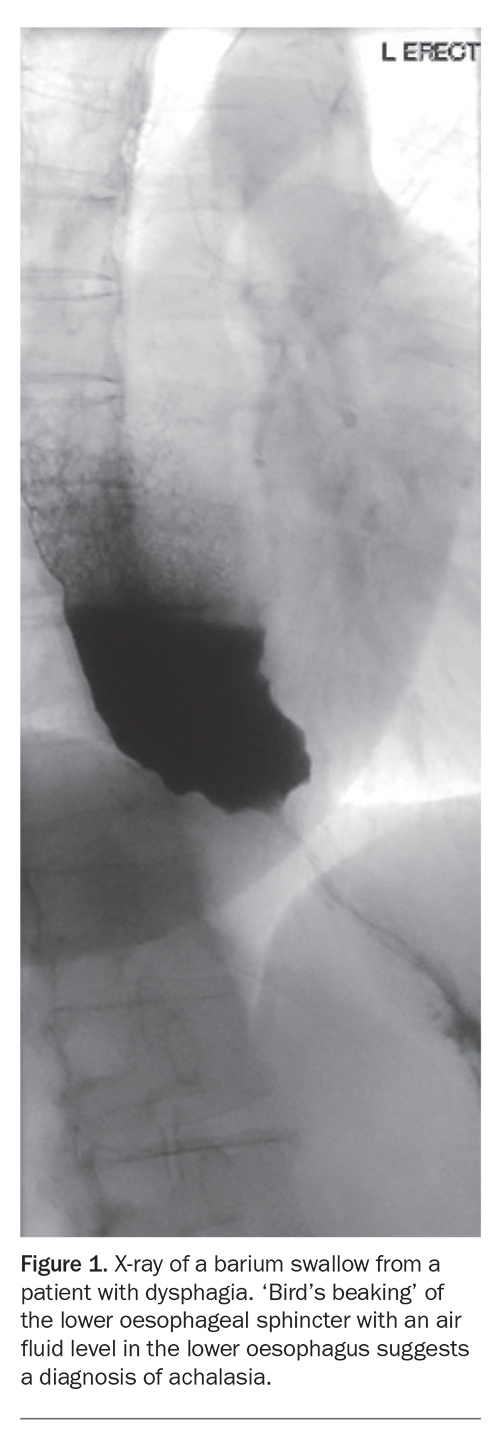
A more specific test is a timed barium swallow; the column of contrast medium is measured at one-, two- and five-minute intervals and provides important information for the diagnosis of motility disorders, such as achalasia, and may prompt further testing with oesophageal manometry.12 A barium swallow suggestive of achalasia typically shows a narrowing towards the lower oesophageal sphincter with a dilated proximal oesophagus resembling a ‘bird’s beak’ (Figure 1).
{kind=link}
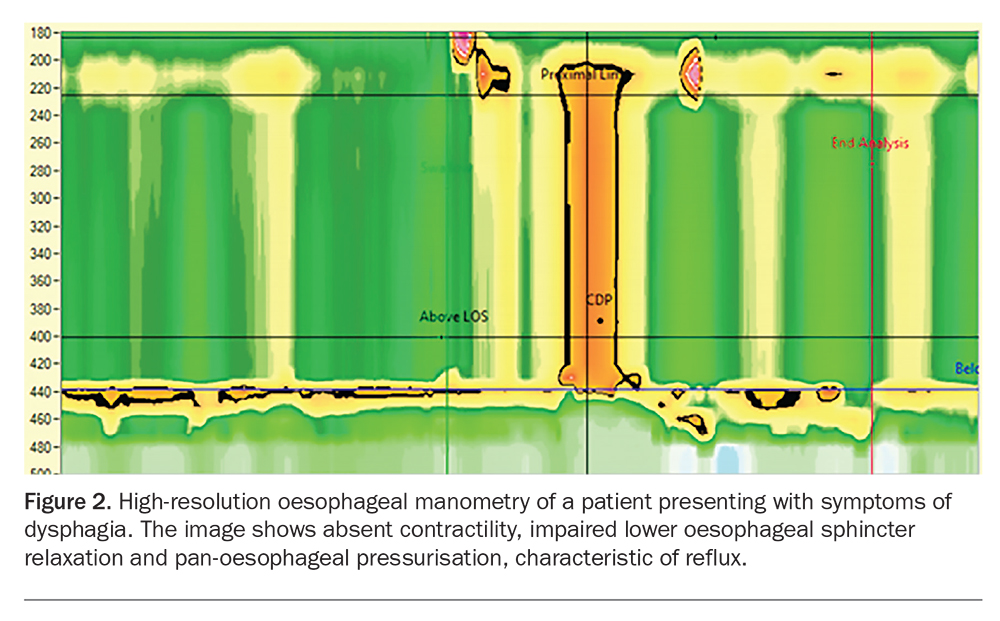
High resolution oesophageal manometry
High-resolution oesophageal manometry is the gold standard investigation for the diagnosis of oesophageal motility disorders.18,19 This test uses liquid-perfused or solid-state transducers to detect pressure readings at differing levels of the oesophageal musculature, sphincters and at the gastro-oesophageal junction to assess whether the muscles around the oesophagus are functioning properly (Figure 2).12,18,19 It is often used in conjunction with both gastroscopy and barium swallow to make a diagnosis of a motility disorder, most notably achalasia.
{kind=link}
Treatment
Treatment for dysphagia is based on the results of investigations and subsequent diagnosis. Patients with complex causes of dysphagia are treated by a multidisciplinary team that includes gastroenterologists, dietitians, speech pathologists, ENT surgeons and upper gastrointestinal surgeons. Treatment is often multifaceted and involves diet manipulation or modification, ensuring maintenance of caloric intake and reducing the risk of pulmonary aspiration.
Medications include PPIs for gastro-oesophageal reflux disease and eosinophilic oesophagitis, for which topical corticosteroids may also be considered. Recently, the orally disintegrating tablet formulation of budesonide has been made available on the PBS for patients with diagnosed eosinophilic oesophagitis successfully treated with budesonide. Treatment must be by or in consultation with a gastroenterologist.4,13
More specialised management for strictures, obstructive lesions and achalasia includes new endoscopic and surgical procedures. Peroral endoscopic myotomy (POEM) is now a widely used endoscopic treatment for achalasia. It has similar clinical outcomes to the traditional treatment of laparoscopic Heller myotomy of the lower oesophageal sphincter but with lower rate of serious adverse events; however, it may have a higher rate of reflux-associated oesophagitis.20
Conclusion
For patients presenting with dysphagia, history and examination are the mainstay of assessment and vital in guiding the investigation of dysphagia in primary care. In the older patient, be vigilant for causes of dysphagia secondary to extrinsic compression of the oesophagus. Gastroscopy is the first-line investigation for most patients; however, in the context of oropharyngeal dysphagia, requesting a barium swallow and considering early input from neurologists, speech pathologists and ENT specialists can assist with diagnosis and management. High-resolution oesophageal manometry is the gold standard for the diagnosis of several motility disorders, which require specific and specialised therapies. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.