Coeliac disease – optimising long-term management

Coeliac disease is frequently encountered in general practice and yet it often remains undiagnosed. Patients typically present with common, nonspecific issues such as gastrointestinal upset, iron deficiency and lethargy. A systematic approach to diagnosis and follow up will support patient outcomes.
- Coeliac disease is common presentation in general practice but is often overlooked.
- Expeditious diagnosis and treatment can reduce morbidity and improve quality of life.
- Screening for coeliac disease should be considered in patients with risk factors.
- Accurate serology and histology testing requires active gluten consumption.
- Small intestinal histology is the gold standard for diagnosis; however, in very select circumstances, a paediatric gastroenterologist can diagnose coeliac disease based on serology alone.
- A multidisciplinary management approach and systematic follow up of patients with coeliac disease is important.
Coeliac disease is a chronic illness with autoimmune-like features, characterised by gluten-dependent symptoms, systemic effects, coeliac disease-specific antibodies and enteropathy.1,2 Coeliac disease affects both sexes, with a modest female predominance, and can develop at any age. Although its global seroprevalence is 1.4%, there is substantial variability based on geography.3 Prevalence in some areas, such as South-East Asia, remains poorly studied. Untreated coeliac disease is associated with increased morbidity, including higher rates of autoimmune disease, osteoporosis and lymphoproliferative disease, as well as decreased quality of life and increased health care use. Fortunately, expeditious diagnosis and treatment with a strict gluten-free diet can minimise these risks.
Coeliac disease affects more than 350,000 people in Australia. However, given its broad and often nonspecific presentation, the condition is frequently overlooked, with up to 80% of patients remaining undiagnosed.4 Case finding of at-risk individuals is recommended to detect cases before substantial morbidity has developed. Sensitivity screening antibody tests exist; however, a definitive diagnosis relies on the demonstration of characteristic small intestinal damage. The accuracy of these investigations is compromised when patients remove gluten from their diet prior to investigation.
GPs play a central role in the long-term management of patients with coeliac disease, including confirmation of treatment efficacy and monitoring for complications, which support optimal long-term outcomes.5
Pathogenesis
Gluten is a complex storage protein derived from wheat, barley and rye that contains peptides resistant to gastrointestinal degradation. Oat contains similar gluten-like peptides and, although it appears substantially less toxic than wheat, barley and rye, it currently remains excluded from the gluten-free diet in Australasia. Gluten peptides are modified (deamidated) by an enzyme called tissue transglutaminase (tTG), which ‘supercharges’ the antigen to enable effective activation of gluten-specific T cells in patients with coeliac disease. Activated T cells orchestrate a proinflammatory reaction that ultimately results in damage to and inflammation of the small intestine. Testing for the antibodies that form against tTG and deamidated gliadin peptides (DGP) is a useful screening tool for coeliac disease.
Similar to classic autoimmune diseases (e.g. type 1 diabetes), genetic and environmental factors are important in coeliac disease development.6 Key human leukocyte antigens (HLA) genes are essential for the gluten-specific T-cell response and for coeliac disease to develop.7 The HLA genes imparting the greatest risk – the HLA-DQ2 and DQ8 genes – are seen in over 99% of all patients with coeliac disease (HLA-DQ2.5 in 88%, HLA-DQ8 in 6% and HLA-DQ2.2 in 4%).8 Notably, these HLA genes are present in about 40 to 50% of the general population in Australia.4 This means that HLA testing has a poor positive predictive value and an exceptional negative predictive value for coeliac disease.
Environmental factors contribute to the development of coeliac disease; however, their identity and role remain poorly defined. Gastrointestinal infections, exposure to large amounts of gluten under the age of five years and seasonality and geographic location of birth have been implicated in the development of coeliac disease in children aged 2 to 18 years.6 These environmental factors are thought to alter the gut microbiome, which in turn influences immune responses to gluten. Results from prospective cohort studies examining environmental and genetic factors in the development of coeliac disease and type 1 diabetes, such as the Australian Environmental Determinants of Islet Autoimmunity (ENDIA) study, are eagerly awaited.
When to consider coeliac disease
Despite the high prevalence of coeliac disease, a case finding strategy is considered the best approach to identifying patients. Population screening is not currently recommended because coeliac disease can occur at any age (including later in life) and there is currently insufficient data to confirm improved outcomes with screen-detected disease.
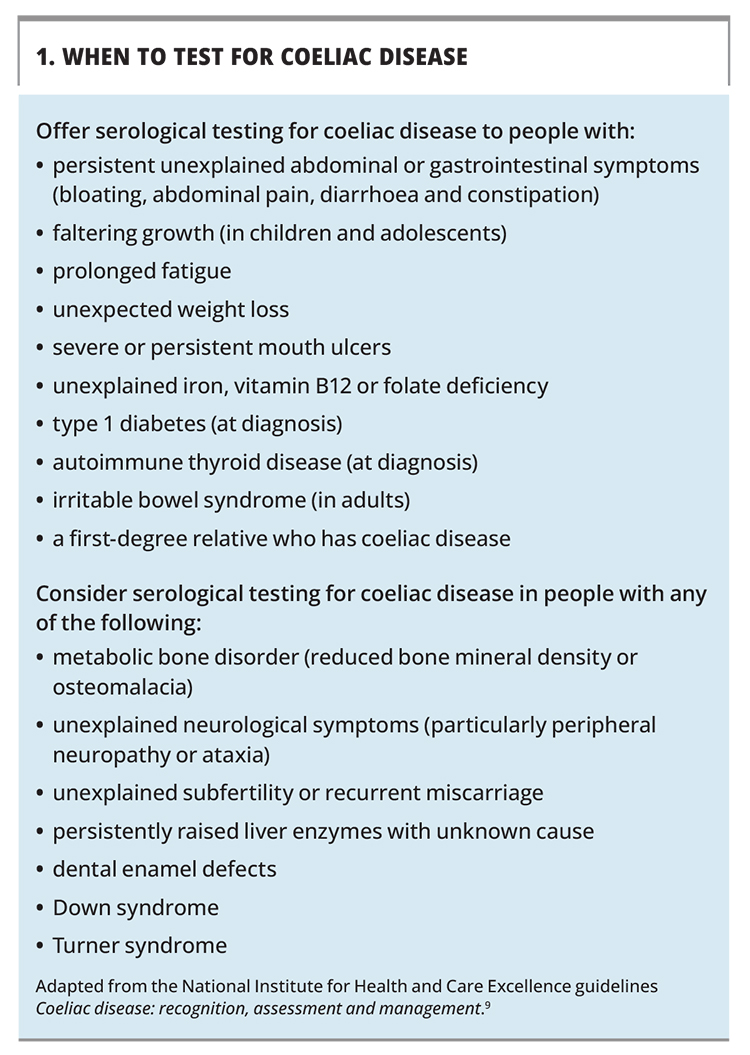
The symptoms and risk factors that should prompt consideration for coeliac disease screening are summarised in Box 1.9 Typical symptoms include gastrointestinal upset, such as bloating or abdominal pain, nausea, weight loss and diarrhoea or constipation (indistinguishable from irritable bowel syndrome). Extraintestinal issues are also common and include chronic lethargy, headaches, poor concentration, iron deficiency and anaemia. An itchy, blistering rash, called dermatitis herpetiformis, is also related to coeliac disease. Malabsorption is a feature in only a subset of patients. A third of patients with coeliac disease are overweight or obese at diagnosis.10 Acute reactions to gluten ingestion are often reported; however, given the ubiquity of gluten in Western diets, these often go unnoticed by patients until they are adherent to a strict gluten-free diet. Notably, 20% of patients are regarded as ‘asymptomatic’ at diagnosis; however, many patients will have subclinical nutrient deficiencies or reduced bone density.
{kind=link}
Diagnosis and investigations
Once coeliac disease is suspected, patients should undergo serological screening and, if serological screening is positive, a gastroscopy should be performed to obtain a tissue sample for diagnosis (Flowchart).
Coeliac serology
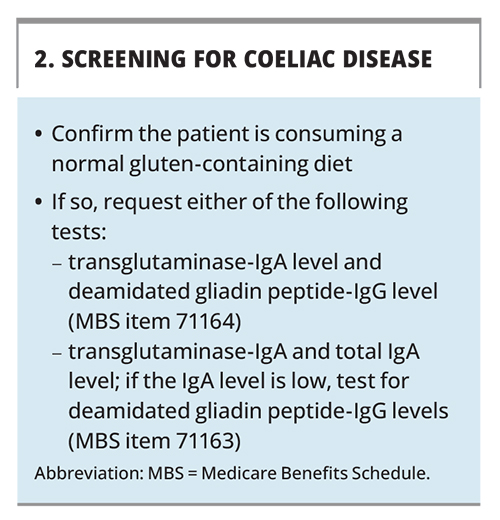
Serologic testing for coeliac disease assesses for tTG and DGP antibodies. Testing for endomysial antibodies is another approach, although this is less commonly performed in Australia. These assays are highly sensitive and specific. They can be employed in two ways (Box 2).11 A common approach is to measure tTG-IgA and DGP-IgG levels together, which may improve detection of coeliac disease compared with a single antibody measurement.12 Assessing an IgG-based antibody also mitigates potential false-negative results that occur in the 3% of people with coeliac disease who have selective IgA deficiency. The other approach is to measure tTG-IgA and total IgA levels. If IgA deficiency is present, repeat serology testing using the DGP-IgG antibody test is recommended and is preferred over the tTG-IgG test, which lacks sensitivity.
{kind=link}
Serological tests have a false-negative rate of about 10%. A negative coeliac disease serology result in patients at higher risk for coeliac disease has a reduced negative predictive value and additional work-up should be considered for these patients.13 Occasionally, patients have persistently positive coeliac disease serology results but normal small intestinal histology, a condition called ‘latent’ or ‘potential’ coeliac disease.1 In these patients, treatment and follow up should be individualised in discussion with a specialist. Long-term follow up is recommended, as one-third of these patients will develop full-blown disease with villous atrophy.14
Gastroscopy and small intestinal biopsies
The diagnostic gold standard for coeliac disease is the demonstration of the characteristic enteropathy of coeliac disease: raised intraepithelial lymphocytes, crypt hyperplasia and villous atrophy in the proximal duodenum.11 The accuracy of this approach is dependent on patients actively consuming gluten and not using immunosuppressant medication. Multiple biopsies from the first and second parts of the duodenum are needed as coeliac disease can have a patchy distribution. Importantly, villous atrophy is not pathognomonic for coeliac disease and can be caused by other factors, such as medication use (e.g. olmesartan, NSAIDs), infections (e.g. Giardia, tropical sprue) or illnesses (e.g. Crohn’s disease, common variable immunodeficiency). The combination of villous atrophy with positive coeliac serology is therefore much more predictive of coeliac disease than either alone.
HLA DQ2/8 genotyping
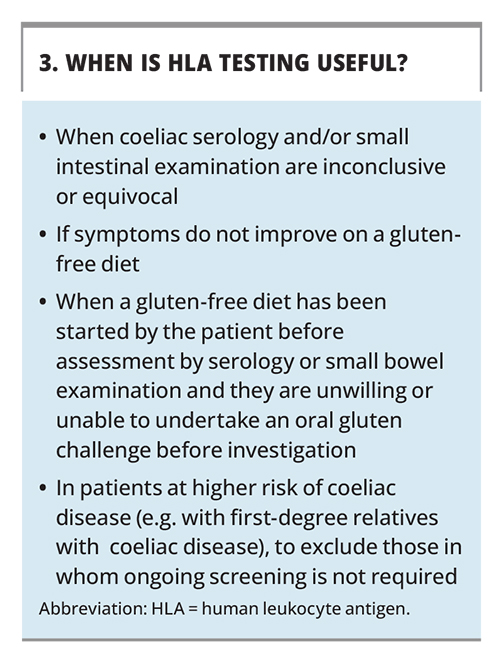
HLA DQ2/DQ8 genotype testing is not a routine investigation, although it can be useful in specific situations (Box 3).7 Its main benefit is derived from its ability to exclude a coeliac disease diagnosis when the HLA susceptibility genes for coeliac disease are not present. The absence of HLA-DQ2.5, HLA-DQ8, and HLA-DQ2.2 allows coeliac disease to be confidently excluded in 99% of patients. Unlike serology and intestinal histology, genotyping is a ‘once only’ test and the results are not adversely affected by a gluten-free diet. It has an exceptionally strong negative predictive value: a negative HLA result excludes coeliac disease. A positive result does not diagnose coeliac disease and further investigation may be needed. Importantly, a positive HLA genotyping result in isolation has a poor predictive value for coeliac disease and does not mean an individual should commence a gluten-free diet.
{kind=link}
Non-biopsy guidelines in children
In paediatric studies, levels of tTG-IgA greater than 10 times the upper limit of normal have a very strong predictive value (more than 99%) for coeliac disease.15 This data has shaped the recent European Society for Paediatric Gastroenterology Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease, where the recommended process is as summarised below.
- Patients with a positive tTG-IgA result should be referred to a paediatric gastroenterologist.
- In patients with a tTG-IgA level greater than 10 times the upper limit of normal and who have a positive endomysial antibody result on a separate blood sample, coeliac disease can be diagnosed by the paediatric gastroenterologist without a gastroscopy.
- Patients with a tTG-IgA level of less than 10 times the upper limit of normal are recommended to undergo gastroscopy to confirm the diagnosis.15
The authors indicate implementation of these guidelines should be by a paediatric gastroenterologist. An Australian study has supported the use of this serodiagnostic approach and found that the ‘more than 10 times the upper limit of normal’ rule applied to one-third of children with coeliac disease.16 Currently, these guidelines are employed variably in children with positive coeliac disease serology in Australia and have not been applied to adults with positive coeliac disease serology.
Gluten challenge
A gluten-free diet for more than a few months may cause false-negative coeliac disease serology and intestinal histology. The only definitive way to secure a diagnosis is to reintroduce gluten before assessment.11 The optimal dose and timing of a gluten challenge required for definitive diagnosis is unclear; however, as the gluten challenge is being done to determine with as much confidence as possible whether coeliac disease is present, returning to a normal gluten-containing diet (about 15 g per day) for at least six weeks is ideal. In practice, it is reasonable to recommend 4 to 8 g per day (e.g. two to four slices of bread daily), for at least six weeks before investigation with coeliac serology. A gastroscopy should also be considered in cases where suspicion for coeliac disease is high or when there are other reasons to perform a gastroscopy (e.g. the presence of gastrointestinal symptoms). In children, this dose can be reduced by half for the same duration. Starting the challenge slowly and increasing the dose over three to four days is often better tolerated. Patients should be encouraged to persist for as long as they can for the most reliable results. Symptomatic relapse on a gluten challenge is common, although it has poor predictive value for the presence of coeliac disease. This highlights the important point that a ‘trial’ of a gluten-free diet is not helpful for diagnosis, as many people may feel better without necessarily having coeliac disease.
Management
GPs play a crucial and central role in the care of patients with coeliac disease, from diagnosis through to long-term annual follow up.5 A lifelong and strict gluten-free diet is the mainstay of treatment for coeliac disease; however, it should not be commenced until coeliac disease is confirmed by a specialist. Both symptomatic and asymptomatic patients should be treated, as the risk of complications correlates with the presence of intestinal inflammation and not the presence of symptoms. Effective treatment reverses villous atrophy and symptoms, as well as improving patients’ nutrition, bone density and quality of life. Most symptomatic patients experience an improvement within weeks to months on a gluten-free diet, with gastrointestinal symptoms typically resolving faster than extraintestinal manifestations. Symptoms can take longer to resolve in older patients (aged over 50 years) and in patients with a more severe presentation (e.g. with higher antibody levels, more significant enteropathy or signs of malabsorption).
Gluten-free diet
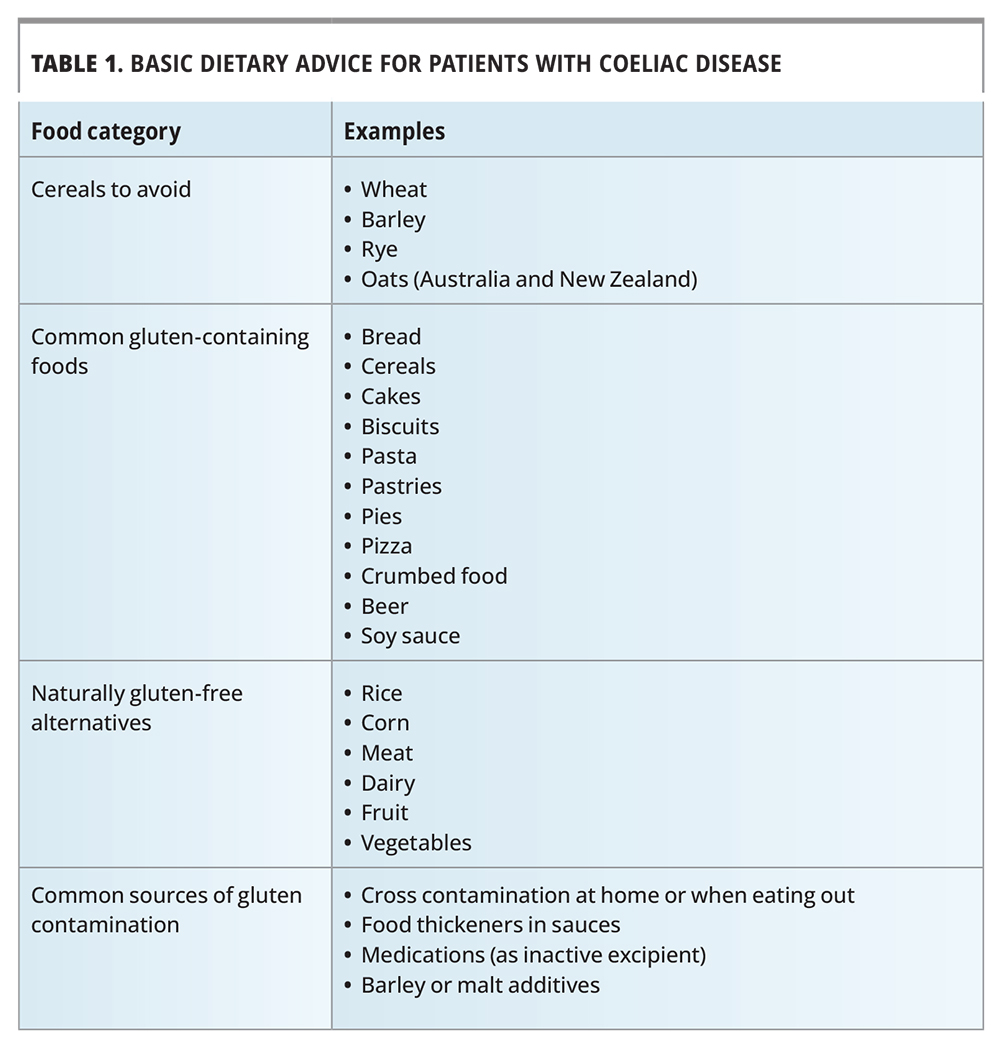
The gluten-free diet involves removing all sources of gluten derived from wheat, rye, barley and oats (Table 1). Small amounts of gluten (e.g. 10 to 50 mg daily over three months) can be potentially harmful; a safe threshold of gluten intake has not been defined and is likely to vary between patients.17,18 Input from a skilled dietitian is important to ensure patients learn the correct skills to facilitate a gluten-free diet and ensure balanced nutrient intake.19 Key skills for patients to learn include knowing which foods contain gluten, how to avoid cross-contamination, how to read labels, how to safely prepare meals and dine out, and how to ensure a healthy and nutrient replete diet. Ongoing encouragement is important to promote strict adherence to the gluten-free diet, as it can be challenging. This is particularly the case for patients who are asymptomatic with gluten exposure. It is important to remind patients that intestinal damage still occurs with gluten exposure even if they are asymptomatic and that the resultant enteropathy predisposes them to nutritional deficiencies and other complications, such as osteoporosis.
{kind=link}
Membership of Coeliac Australia (the national coeliac disease patient advocacy and support body) is recommended and is associated with improved dietary adherence. Gluten-free alternatives are expensive and can be higher in carbohydrates and/or fat and lower in nutrients (e.g. folate and thiamine). The gluten-free diet is low in fibre, so a fibre supplement can be useful, especially for patients with constipation. A higher rate of metabolic-associated fatty liver disease has been reported after coeliac disease diagnosis.20 In Australasia, oats are currently excluded from a glutenfree diet, as a small proportion of patients may develop adverse responses to oats and most commercial brands of oats are contaminated with wheat; however, this legislation is under review.
Complication screening and management
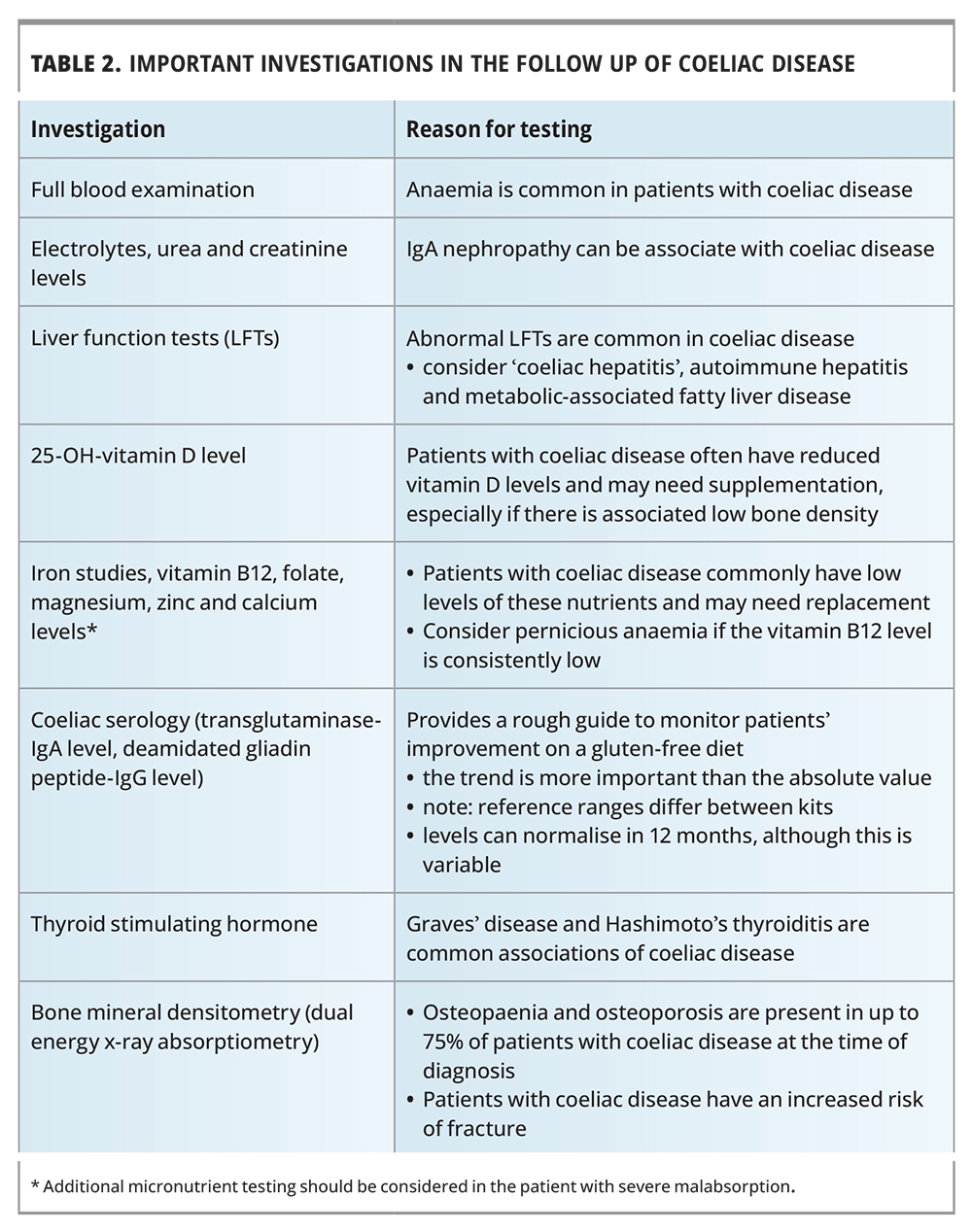
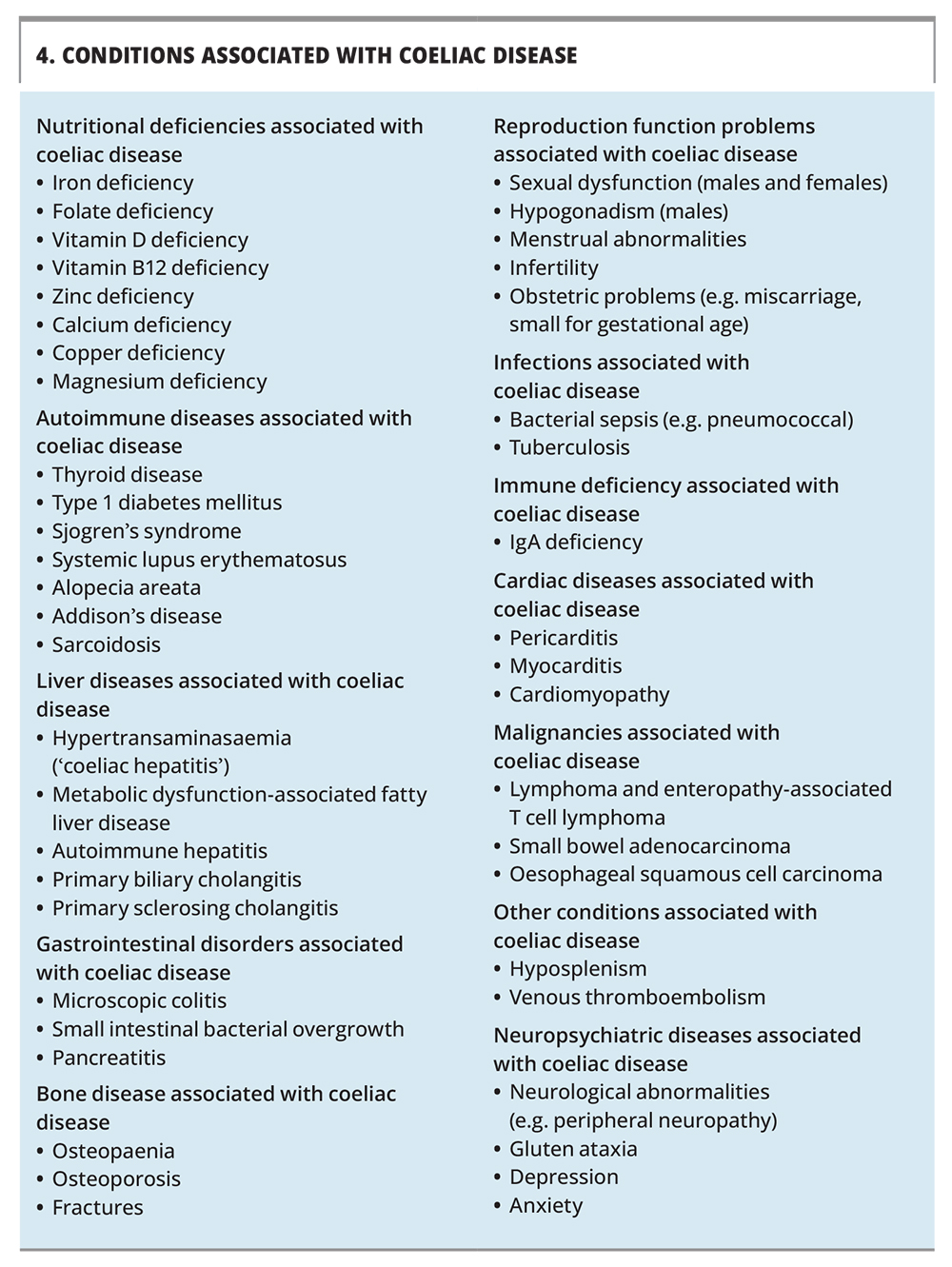
Follow up of patients with coeliac disease should include assessment of disease activity, nutritional status and the presence of complications, based on history and specific testing (Table 2). Monitoring should be undertaken every three to six months in the first year after diagnosis and until patients are stable and symptom free, and yearly thereafter. The broad range of disease associations with coeliac disease are summarised in Box 4.
{kind=link}
{kind=link}
Coeliac disease serology is a marker of disease activity; however, titres correspond poorly to the state of the intestinal lesion, especially in adults. Normalisation of tTG-IgA and DGP-IgG levels is often seen in patients within the first year on a strict gluten-free diet, although it can take longer.10 Coeliac disease serology is not sensitive enough to detect small or infrequent gluten ingestion and is more reflective of exposure over time. When disease activity needs to be accurately assessed, a gastroscopy with small intestinal biopsies is recommended.
Nutrient levels should be measured and any deficiencies corrected (Table 2). Supplementation can often be stopped for many nutrients after six to 12 months as normal absorption resumes.
Performing bone mineral densitometry is recommended because of the high prevalence of osteopaenia, osteoporosis and increased bone fracture risk in patients with coeliac disease.21 Treatment with a gluten-free diet will improve bone density, although it may not normalise it in all cases.
Functional hyposplenism in coeliac disease predisposes to a higher rate of sepsis, especially from encapsulated organisms like pneumococcus.22 It is important to ensure patients are fully vaccinated in general and up to date with the influenza vaccination. Pneumococcal vaccination is recommended, especially in elderly patients. Patients with coeliac disease tend to have a lower response to hepatitis B vaccination, and chronically low responses should prompt clinicians to screen for coeliac disease. The risk of coeliac disease in first-degree relatives is about 10%; screening for coeliac disease is strongly supported in symptomatic relatives and should be considered in asymptomatic relatives.23
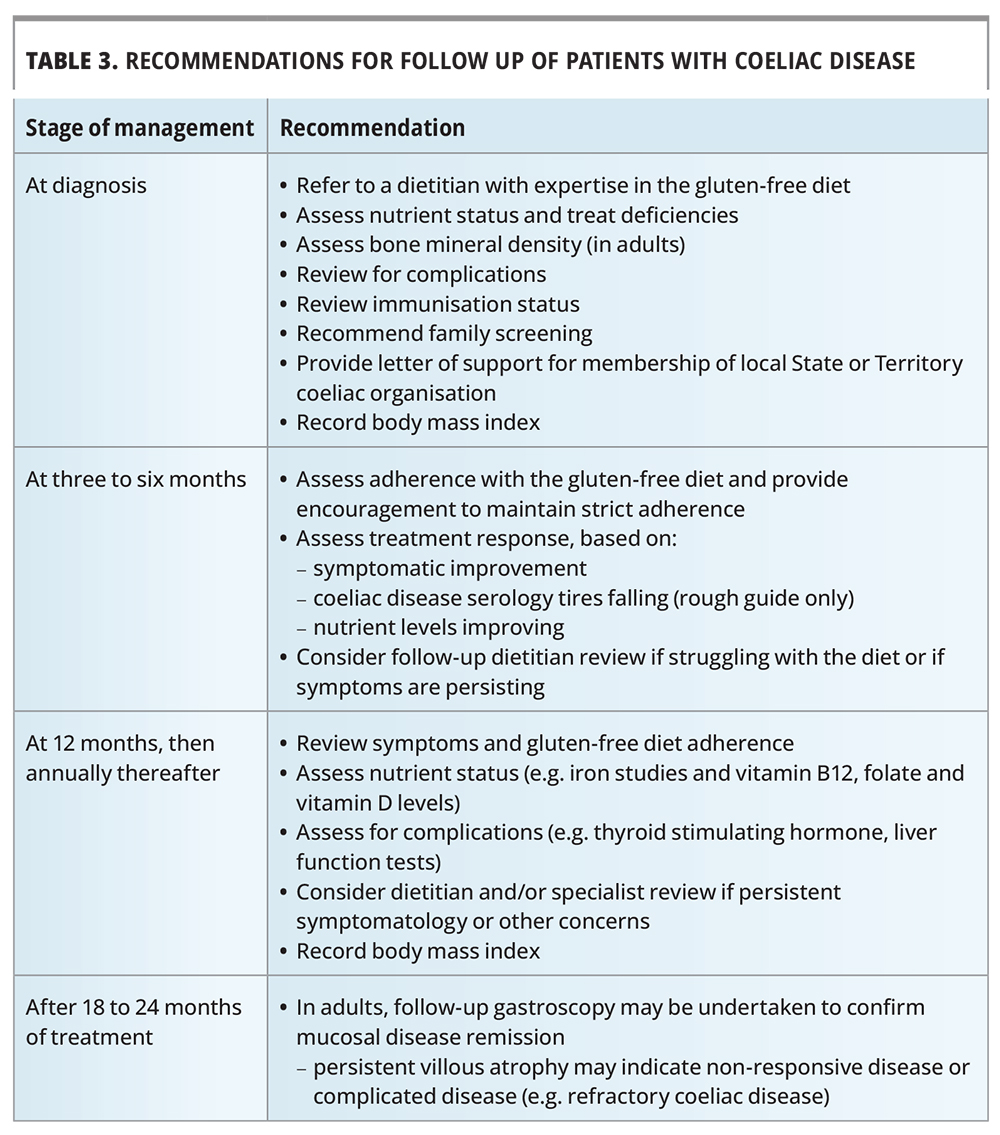
Long-term follow up
Long-term care of patients with coeliac disease involves confirming gluten-free diet adherence, assessing disease activity, evaluating clinical and nutritional status and monitoring for complications (Table 3). Mucosal disease remission is a key goal of treatment to reduce long-term morbidity. Pregnancy is an important time to monitor disease activity, as poor outcomes such as intrauterine growth restriction, miscarriage, low birth weight and premature delivery are more common in the setting of active coeliac disease.24-26
{kind=link}
Managing nonresponsive coeliac disease
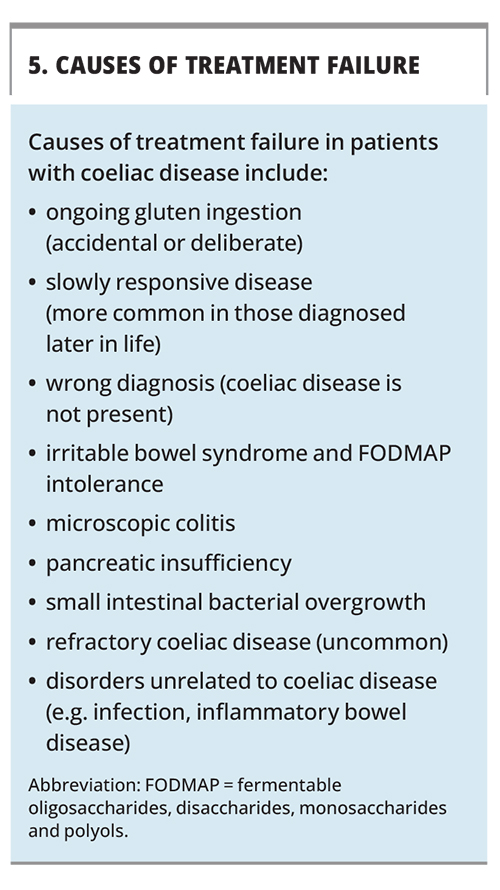
Persistent symptoms and villous atrophy despite a strict gluten-free diet are common, and can be seen in 30% and 60% of patients, respectively.5 A systematic approach to evaluation can usually establish a cause (Box 5). Adherence to the gluten-free diet should be assessed by an expert dietitian, as ongoing gluten exposure, whether deliberate or accidental, is the most common cause for treatment failure. Irritable bowel syndrome with intolerance to fermentable carbohydrates, including oligosaccharides, disaccharides, monosaccharides and polyols (collectively termed ‘FODMAPs’), is a common cause of persistent intermittent symptoms. Common sources of dietary FODMAPs include lactose from dairy or fructans from onion, garlic and wheat. Referral to a specialist is warranted if there are substantial malabsorptive symptoms, such as diarrhoea and weight loss, as this could suggest refractory coeliac disease. Refractory coeliac disease is a rare complication of coeliac disease when a strict gluten-free diet fails to resolve symptoms or the small intestinal damage. A major concern with refractory coeliac disease is the development of lymphoproliferative malignancies, particularly a variant called an enteropathy-associated T-cell lymphoma that carries a very poor prognosis.
{kind=link}
Non-coeliac gluten (or cereal) sensitivity
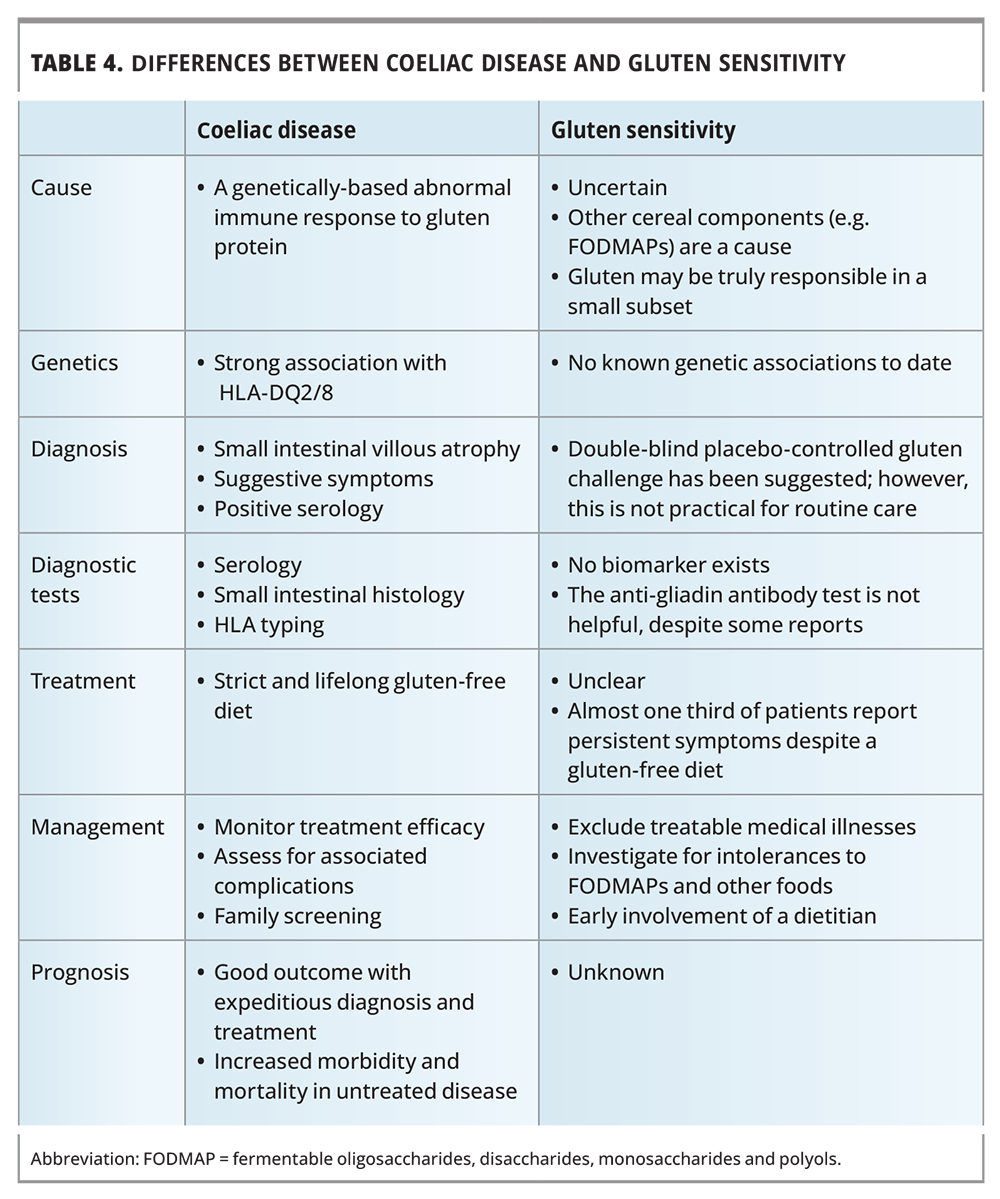
The term ‘gluten sensitivity’ describes patients without coeliac disease who report symptoms that they attribute to gluten, with apparent improvement on a gluten-free diet.1 However, this term is being phased out, as recent data on patients reporting ‘gluten sensitivity’ has shown that the cause of symptoms is not gluten but other cereal components, such as wheat fructans.27,28 Many clinicians now use the term ‘non-coeliac cereal sensitivity’ to describe patients with this clinical entity. Symptoms can be the same as coeliac disease; however, a higher proportion tend to complain of lethargy, headaches, ‘brain fog’ and fibromyalgia-like symptoms (Table 4). Disease pathogenesis is unknown and no biomarker exists. It is important that coeliac disease is assessed for in patients who report gluten or cereal sensitivity as this diagnosis has longer-term health implications for patients and their families. Often a gluten challenge is required as a gluten- free diet has usually already been commenced by the patient.
{kind=link}
The future
Understanding the genetic and immunological basis for coeliac disease has afforded the opportunity to develop new diagnostic approaches and treatments. These treatments include targeted enzymes that degrade gluten peptides, a transglutaminase inhibitor, a drug that reduces intestinal permeability, and approaches that aim to induce gluten tolerance, several of which are in human Phase 1 or 2 clinical trials.29 No drug has yet successfully progressed beyond Phase 2 trials, with a tolerogenic gluten peptide ‘vaccine’ and a drug modulating tight junctions recently failing to demonstrate efficacy.29 Many of these treatments aim to reduce the gluten load in the gut to assist the gluten-free diet, whereas others aim to restore immune tolerance to gluten to ultimately allow an unrestricted diet. Highly sensitive and specific diagnostics that assess the causative gluten-specific T cell are also under development and may one day enable coeliac disease to be diagnosed on a blood sample even when the patient is strictly gluten free.30,31 Greater understanding of environmental factors and the role of the microbiome may eventually inform new approaches for coeliac disease treatment and even prevention.6
Conclusion
Coeliac disease is a highly prevalent autoimmune-like illness, which, if untreated, can lead to substantial morbidity, impaired quality of life and increased mortality. Prompt recognition and testing of at-risk patients by the GP is the key to expediting diagnosis and treatment. A strict gluten-free diet will resolve symptoms and reduce morbidity, especially if undertaken before substantial complications have developed. Specialist dietitian input is essential to ensure the gluten-free diet is followed correctly and nutrient intake is adequate. Long-term medical follow up is best managed by the GP; a systematic approach will ensure optimal patient outcomes. MT
COMPETING INTERESTS: Dr Saitta: None. Associate Professor Tye-Din reports consulting fees from Anatara Lifesciences, Anokion, Chugai Pharmaceuticals, Janssen, Novoviah, Vaccitech and Equillium; Honoraria from Inside Practice and Takeda; research funding from Chugai Pharmaceuticals, Codexis, Immunic, Novoviah and Tillots; is Chair of the Data Safety Monitoring Board for Topas Therapeutics; Chair of the Medical Advisory Committee, Coeliac Australia; and Secretary of the International Society for the Study of Celiac Disease.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.