Cell-based quadrivalent influenza vaccine – a new method of influenza vaccine production
A cell-based quadrivalent influenza vaccine (Flucelvax Quad) is available on the private market in Australia in 2021. This vaccine is propagated in cell culture rather than in the conventional hens’ eggs. The cell-based vaccine has similar safety and efficacy to existing influenza vaccines and offers a useful alternative.
Influenza is a seasonal infectious disease that circulates most widely in the colder months (in Australia, April to October). Most people with influenza recover without serious complications. However, serious illness, hospitalisation and death can occur.1,2 The populations most vulnerable to severe disease include older adults, young children, pregnant women and people with certain chronic medical conditions.3
The production of influenza vaccines used in Australia has traditionally involved the inoculation of fertilised hens’ eggs with influenza strains selected for that season. This is followed by replication of the virus within the eggs, harvesting of the virus, inactivation and purification. This process requires long and careful planning to ensure that millions of fertilised hens’ eggs are available for the vaccine manufacturing each year.
The effectiveness of influenza vaccination is affected by the age and immunocompetence of vaccine recipients. It also varies between seasons because of factors such as the degree of similarity between the virus strains in the vaccine and those circulating in the community.4 Influenza vaccine effectiveness generally ranges from 45 to 64%.5,6
Concerns have been raised about egg-based influenza vaccine production methods. These include the potential for the influenza vaccine supply to be compromised if there is a worldwide shortage of eggs or if a rapid increase in supply is needed (e.g. in an influenza pandemic). Also, the replication of influenza viruses in eggs results in antigenic changes that reduce the match with the strains selected for that season.
This so-called ‘egg adaptation’ has been a particular problem for the haemagglutinin antigen of influenza A virus subtype H3N2. It is thought to have contributed to lower influenza vaccine effectiveness in some years, particularly when this subtype has dominated. As A(H3N2) strains are seen more commonly in older people, who have the highest rates of death from influenza, this is a ‘double whammy’ effect.7,8
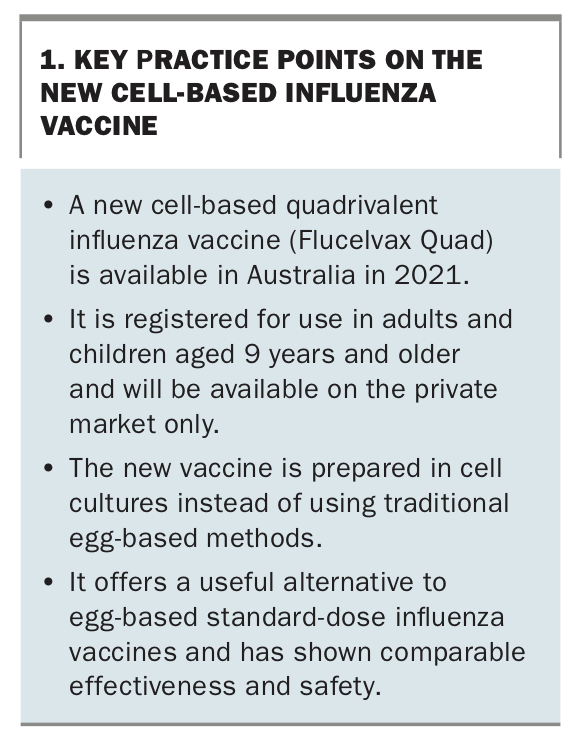
Cell-based influenza vaccine production is one of the methods being developed to improve the durability and magnitude of protection from influenza vaccines, as well as to ensure supply. A cell-based influenza vaccine has been approved by the TGA and is available in Australia for the 2021 influenza season. This article discusses the new vaccine. Key practice points are summarised in Box 1.
{kind=link}
What is the cell-based influenza vaccine?
The newly registered influenza vaccine (Flucelvax Quad) is a quadrivalent inactivated influenza vaccine. It is prepared in Madin-Darby canine kidney (MDCK) cell cultures instead of the traditional egg-based methods. The active ingredient of the vaccine includes the haemagglutinin surface antigens of four strains of influenza virus, belonging to the A(H1N1) subtype, A(H3N2) subtype, B/Yamagata lineage and B/Victoria lineage, respectively (15 mcg of each in 0.5 mL of vaccine). The specific strains and amount of viral antigens contained in the vaccine comply with the seasonal recommendations of the Australian Influenza Vaccine Committee (AIVC), which are based on the WHO recommendations for each annual influenza season.
The virus surface haemagglutinin in the cell-based vaccine acts in a similar way to the inactivated surface antigen in the traditional egg-based vaccines. It stimulates the immune system to produce a protective antibody response within about two weeks of vaccination.
When and how is the vaccine used?
The cell-based vaccine was registered in Australia in 2020 for use in adults and children aged 9 years and older to prevent influenza disease. It has also been approved for use in the US, Canada and Europe.
The vaccine is not yet recommended or registered for children aged 6 months to under 9 years.9 It is available on the private market in Australia in the 2021 influenza season but is not funded under the National Immunisation Program (NIP). The vaccine is administered by intramuscular injection in a single 0.5 mL dose.9
Common side effects
As with any influenza vaccine, postvaccination symptoms may occur. Some of these expected adverse effects mimic the symptoms of influenza (e.g. low grade fever and myalgia). However, the cell-based influenza vaccine, like all other influenza vaccines available in Australia, does not contain live influenza virus and thus cannot cause influenza. Common, usually mild and temporary, adverse effects following vaccination with the cell-based vaccine include:
- injection site pain
- injection site erythema
- headache
- fatigue
- myalgia.10-12
Studies on cell-based influenza vaccine suggest that local adverse events are slightly more frequent than with standard egg-based influenza vaccine. A randomised trial reported local adverse events in 29% of those given cell-based influenza vaccine compared with 25% of those given egg-based vaccines.10,12,13 However, there was little or no difference in the rates of systemic adverse events between cell- and egg-based influenza vaccines.12,14 No vaccine-related serious local or systemic adverse events were reported in these studies after either the cell- or egg-based vaccines.
Use in pregnancy and breastfeeding
Pregnant women are strongly recommended to receive influenza vaccine during each pregnancy, because of their higher risk of morbidity, mortality and adverse birth outcomes if infected.
The cell-based influenza vaccine is currently classified as pregnancy category B1 because of lack of data on its use in pregnant women. However, reproductive and developmental toxicity data for the trivalent formulation of the cell-based vaccine do not show an increased risk of developmental abnormalities. Theoretically, there is no reason to expect any difference in the safety profile of cell-based compared with egg-based influenza vaccines. Similarly, although cell-based influenza vaccine has not yet been evaluated in nursing mothers, there is no reason to expect its safety should differ from that of egg-based vaccines.
Egg-based influenza vaccines, which have been available for much longer, have more evidence on use in pregnancy. Most are currently classified as pregnancy category A in Australia. As only egg-based influenza vaccines are currently available free to pregnant women under the NIP, it is likely most pregnant women in Australia will continue to receive these vaccines in 2021.
Important precautions and interactions
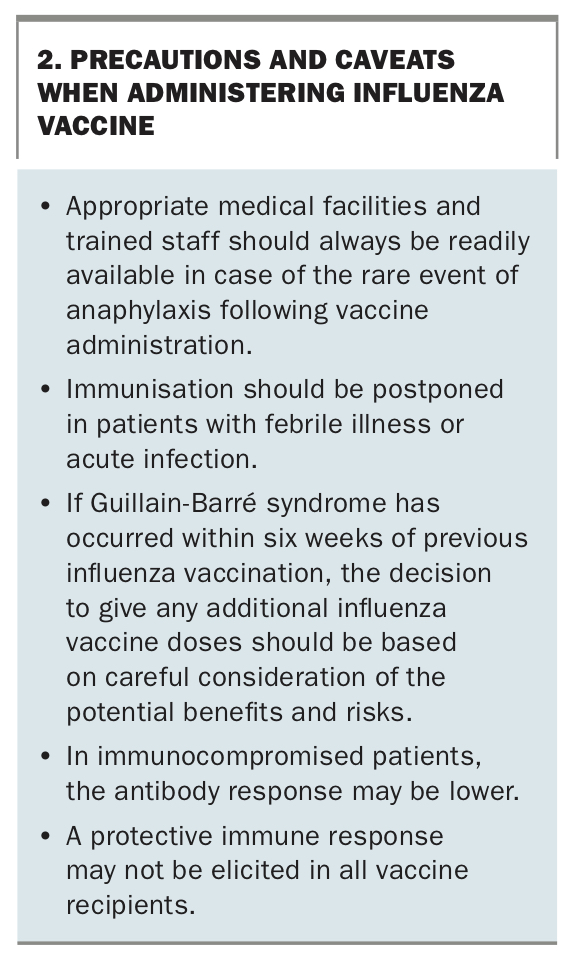
Precautions to be taken when administering cell-based influenza vaccines are similar to those for traditional egg-based influenza vaccines (Box 2). Both vaccines are contraindicated in individuals with known severe allergic reactions (e.g. anaphylaxis) to any component of the vaccine or a previous dose of any influenza vaccine.
{kind=link}
Although no data are available on coadministration of the cell-based quadrivalent influenza vaccine with other vaccines, experience with the trivalent formulation suggests that it can be given at the same time as most other vaccines. However, in 2021 the influenza vaccine program will be rolling out simultaneously with the COVID-19 vaccination program, and it is recommended that COVID-19 vaccines are not given on the same day as any other vaccines nor within 14 days before or after other vaccines.15 Immunisation providers should continue to monitor all recommendations on COVID-19 and influenza vaccination throughout 2021 to ensure they follow the latest advice.
Effectiveness of cell-based vs egg-based influenza vaccine
As described above, in recent years antigenic changes have been observed in the vaccine strains produced from eggs, especially for the A(H3N2) viruses.8 This occurs if the seed strain does not replicate well in eggs, and many cycles of growth (‘passages’) are required to achieve high viral titres. During these numerous passages, the antigenic components of the haemagglutinin surface antigen can change as the virus adapts to avian receptors. This potentially leads to a mismatch between the vaccine strain produced and the epidemic strain of A(H3N2), reducing the effectiveness of the vaccine.7,8 Cell-based production methods can avoid this problem and may result in a closer match of vaccine strains with epidemic isolates of influenza.
However, whether this theoretical advantage significantly alters the ‘real world’ effectiveness of cell-based compared with egg-based influenza vaccines is less clear. All evidence on relative effectiveness of these two vaccine types currently comes from observational studies conducted across two influenza seasons.16-19 These studies indicate that, compared with egg-based vaccines, MDCK cell-based influenza vaccine may slightly reduce non-laboratory-confirmed influenza-related hospitalisations or emergency department (ED) visits in some influenza seasons.16-19 However, there was no evidence of significant differences in effectiveness against laboratory-confirmed influenza or pneumonia-related hospitalisations or ED visits.16,19,20
Given the variability of the effects of cell-based (and egg-based) influenza vaccine on different clinical outcomes, there is currently insufficient evidence to conclude that this cell-based influenza vaccine is more protective against influenza-related outcomes than egg-based standard-dose influenza vaccines. Therefore, based on the evidence currently available for adults and children aged 9 years and over, MDCK cell-based influenza vaccine can be considered as an equivalent alternative to standard-dose egg-based influenza vaccines.9
At present, the only preferential recommendation for influenza vaccines by the Australian Technical Advisory Group on Immunisation (ATAGI) is the use of adjuvanted influenza vaccine (Fluad Quad) in adults aged 65 years and over in preference to standard dose egg-based vaccines.9
Conclusion
The newly registered MDCK cell-based influenza vaccine (Flucelvax Quad) offers a useful alternative to egg-based standard dose influenza vaccines in regard to diversifying production lines and influenza vaccine supply. The vaccine has comparable efficacy to egg-based standard dose influenza vaccines. It is currently available only on the private market. Although local adverse events may be slightly more common after vaccination with the cell-based vaccine, overall it also has a comparable safety profile to standard egg-based influenza vaccines.
We will continue to see more and varied types of influenza vaccine produced globally in an effort to increase availability and hopefully leading to a greater array of safe, more effective vaccines. Exciting new advances in vaccine development, particularly related to the science of the COVID-19 pandemic vaccines, should also inform further innovation in design of influenza and other vaccines for years to come. MT