Management of adolescent obesity – what works and how we define success

Adolescence is a time of dramatic physical, neurocognitive and psychosocial change. These changes demand developmentally appropriate approaches, priorities and definitions of success when managing adolescent patients with overweight and obesity. Engagement, patience and flexibility are key.
- Adolescent obesity is unlikely to spontaneously remit and intervention should not be delayed until adulthood as health trajectories are established in adolescence.
- Adolescent obesity is associated with psychosocial and medical comorbidities, and these should be considered when discussing weight management goals with the patient.
- The principles of weight management for adolescents are often the same as for adults but have a much smaller evidence base.
- Lifestyle management is key to long-term weight loss and remains essential even if additional therapies are added.
- Time and patience are needed to engage the young person and understand their goals.
The principles of obesity management for adolescents are the same as for adults but the approaches required are different. This is because adolescence – defined by the World Health Organization as the second decade of life – is an intense stage of development. In Australia, one in four adolescents is overweight and one in eight has obesity.1 As in adults, obesity in adolescents is the result of:
- a polygenic genetic predisposition
- intrinsic factors such as poor sleep, depression or physical disability
- environmental factors, including those leading to sedentary lifestyles and reduced physical activity, and readily available high-density food and drink.
Obesity in an adolescent is unlikely to resolve spontaneously.2 Both sexes can use the pubertal growth spurt to reduce absolute weight via weight maintenance. Adolescent boys have a distinct advantage compared with adolescent girls because of body composition changes that increase lean mass, which is metabolically more active than fat mass. Emerging autonomy and increasing peer influences in adolescence make lifestyle interventions more difficult to follow. Social anxiety and depression, weight stigma, cyber and other bullying and social exclusion may all come together to drain the capacity of adolescents to address their health.
The ability to plan and develop medium-to-long term goals, and to appreciate and continue the permanent behavioural changes needed to reduce obesity and maintain weight are regulated by the prefrontal cortex.4 This part of the brain is not fully mature until the mid twenties.4 The impulsive and hyperemotional brain of mid adolescence is often counterproductive for weight management.
The threat of obesity-related morbidity has a limited impact on motivating adolescents to lose weight. This is partly because of their cognitive inability to envisage so far into the future and partly because the immediate impact of their weight is primarily psychosocial. Future morbidity is almost always a significant concern for parents, many of whom have obesity and/or a history of failed weight loss attempts themselves. The GP is an advocate for young people and their immediate struggles, and this may involve counselling parents to avoid nagging or negative comments. Their role is to provide a supportive environment for healthy eating and exercise and to model the behaviour they are requesting of the young person.
Defining obesity
A healthy body mass index (BMI) range is lower for adolescents than for adults and is adjusted for age and sex. ‘At risk for obesity’ (overweight) is defined as a BMI in the 85th to 95th percentile for age and sex, and obesity as above the 95th percentile.5 A waist-to-height ratio of above 0.5 also signals excess weight. The Edmonton Obesity Staging System for Pediatrics (EOSS-P) has been suggested for adolescents and, importantly, shifts the focus away from weight alone to include the impacts on physical and psychological health and functional limitations.6
Starting the discussion
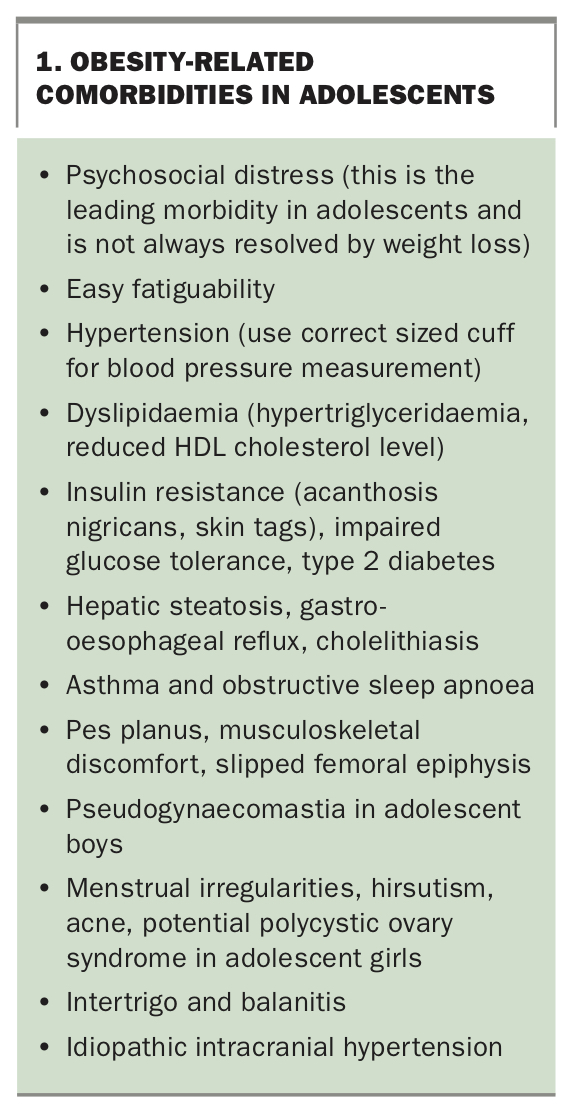
Few adolescents will present to their GP requesting advice on weight management, even though this may be a high priority for them. A patient presenting with obesity-related comorbidities (Box 1) provides an opportunity to discuss body weight and the benefits of modest weight loss (5 to 7 kg). For a young person, these benefits are more likely to relate to increased self-efficacy, easier movement and a greater sense of wellbeing, as these improvements are more personally relevant than any comorbidities. Adolescents understand goal setting and, with support, will work with health professionals to set realistic and achievable goals.
{kind=link}
GPs are understandably concerned about raising weight issues with young people for fear of causing them distress or causing their parents to be angry or upset. Developing trust and a relationship with the young person as an individual, as well as reassurance of confidentiality are important. The confidentiality discussion should include when confidentiality may need to be broken – when there is risk or concern of harm to themselves or others and harm by others.
There are often concerns that weight management may induce an eating disorder. Many adolescents with obesity have disordered eating that may need to be addressed; however, the concern that a sensible weight loss plan induces an eating disorder is not supported by evidence.7
Assessment
History
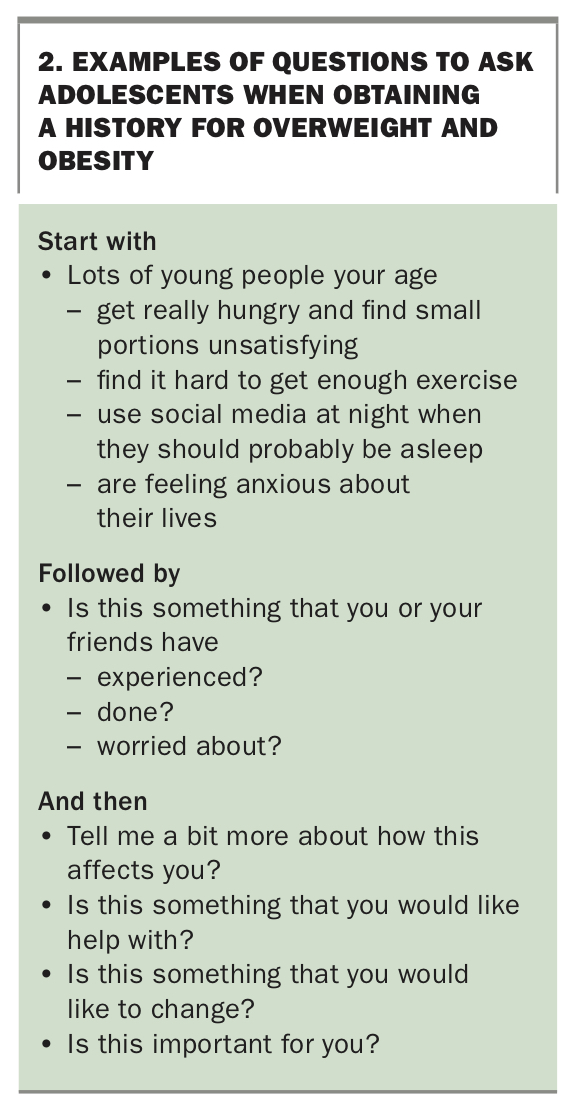
Always try to spend some time talking with the adolescent by themself. Insightful details are likely to be revealed with time and over several visits as trust is established. Start with less personal questions and avoid asking questions with a ‘yes’ or ‘no’ answer. Consider starting with a question such as ‘Lots of young people your age are/have {insert statement}. Is this something you have {thought, done, worried about}?’. Example questions and follow up questions are provided in Box 2.
{kind=link}
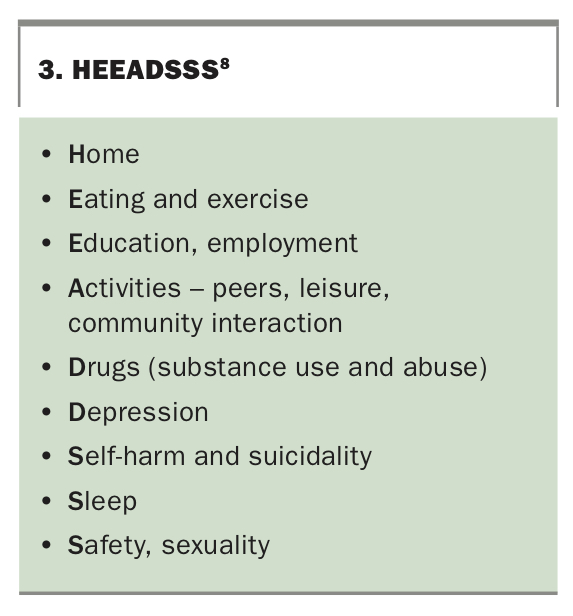
The HEEADSSS semi-structured psychosocial assessment is a useful framework to understand the young person’s life (Box 3).8 Although GPs may understandably feel more confident taking a medical history, using the HEEADSSS framework is an excellent way to build a relationship with the young person and it does not have to be worked through in one visit. Another advantage of focusing on the HEEADSSS framework is that many relevant medical questions can be easily explored. It is highly likely that depression and/or anxiety will need to be addressed before weight management, which itself demands psychological energy. Ignoring mental health issues may set the young person up to fail at weight management, a situation to be avoided at all costs.
{kind=link}
Obtaining a medical and lifestyle history is also important and includes:
- family history of obesity and related disorders
- weight gain history
- hunger and meal patterns, including meal skipping
- food purchased away from home
- small screen use
- regular sport and incidental activity and barriers to these
- snoring and apnoeas, fatigue
- headaches (idiopathic intracranial hypertension, IIH)
- concerns about gynaecomastia in adolescent boys
- menstrual pattern in adolescent girls.
Examination
When examining an adolescent patient, ensure privacy and minimal disturbance of clothing. Parameters of interest include:
- height
- weight
- waist circumference
- puberty stage for assessment of height growth potential (use self-report with Tanner line drawings for comparison)
- blood pressure (use appropriate size cuff)
- acanthosis nigricans – neck and axillae
- tonsillar enlargement
- abdomen – hepatic enlargement (steatosis), striae
- hirsutism and acne in adolescent girls
- pseudogynaecomastia in adolescent boys
- papilloedema ([IIH] mostly in adolescent girls).
Investigations
It is easy to be pressured into over-investigation. Any testing should be paired with obesity-related morbidity (Box 1) and may include the following.
- Thyroid stimulating hormone (TSH) level, although hypothyroidism is rarely associated with severe obesity.
- Fasting lipid profile and glucose and liver transaminase levels to define metabolic risk.
- An oral glucose tolerance test to exclude prediabetes if acanthosis nigricans is present or if there is a family history of type 2 diabetes.
- In adolescent girls with clinical hyperandrogenism, elevated testosterone and low sex hormone-binding globulin levels may suggest polycystic ovary syndrome (PCOS). A pelvic ultrasound will not distinguish between the multicystic ovaries of normal puberty and PCOS. Current guidelines suggest that the diagnosis is not made until eight years after menarche.9
Am I missing a secondary cause of obesity?
A young person with so called ‘simple’ obesity may have increased height growth as the body responds to overnutrition. Girls may have advanced puberty. For boys, the evidence is less clear and suggests that later puberty may be more likely with obesity. A reduction in height velocity, skin fragility and the presence of striae in nonweight-gain areas are common in Cushing’s syndrome. Stretch marks are common on the breasts and hips during puberty in girls, including those in the healthy weight range. Single gene abnormalities may be associated with intellectual disability, dysmorphic features and short stature. Brain tumours causing appetite disturbance are rare and are associated with other symptoms and signs of hypothalamic/pituitary damage.
Management
To establish a lifelong habit, change takes time and requires complex decision- making that can never be achieved by education alone. A focus on lifestyle factors is key to long-term weight management, and issues related specifically to adolescent weight management are discussed below.10
It is important to note that management will occur over time and that followup appointments are essential. GPs can assist the adolescent to choose SMART (specific, measurable, achievable, relevant, time-bound) goals such as:
- weight maintenance initially (stopping further weight gain)
- cutting out soft drinks and other sugar-sweetened beverages
- walking to school most days
- aiming for an earlier bedtime so as to have energy to be active
- aiming to increase daily steps as measured by a smartphone or activity tracker
- avoiding second helpings
- eating fruit instead of chips at school.
Dietary change
There is no single effective ‘diet’ to help with weight loss and the word diet itself is not useful. The goal of weight loss is a reduction in overall energy intake while maintaining a nutritionally sound eating plan and avoiding hunger. Strategies are to ensure adequate protein intake, reduce fats and avoid saturated fats, reduce simple sugars and choose lower glycaemic index options (without higher fat), increase fresh vegetable and fruit intake and drink water and unflavoured milk only. Some adolescents prefer prescription, others general guidelines, and a dietitian is helpful here.
High protein, low carbohydrate and intermittent fasting regimens with three days of 600 to 700 calories can provide a nutritionally sound diet in adolescents.11 There are no trials on chrono-nutrition, i.e. whether eating most calories earlier in the day improves weight loss, and a limited window for eating may be difficult to achieve for adolescents. Apps are available to assist in understanding food composition and energy content. A smaller plate size and large serves of predominantly leafy green vegetables help with portion control and satiety.
Very low energy diets generally use meal replacements for three meals, with the goal of consuming less than 800 calories per day. A quality meal replacement with all essential minerals and vitamins and high-quality protein can be used with medical supervision for short periods of time (four to eight weeks) in the consenting older adolescent with a clear treatment goal of rapid weight loss.11 In adolescents with type 2 diabetes, orthopaedic complications or severe sleep apnoea, a 5 to 10 kg loss will have significant health benefits.12
Decrease sedentary behaviours
Reducing sedentary behaviours is important but can be challenging for adolescents as they have limited discretionary time and school requires prolonged sitting. Although not evidence-based, the Australian guidelines for physical activity and sedentary behaviour are a useful guide (https://www.health. gov.au/health-topics/physical-activity-and-exercise/physical-activity-and-exercise-guidelines-for-all-australians/for-children-and-young-people-5-to-17-years). Reducing leisure screen time (except for online exercise programs) is a starting point, but this time needs to be filled with another activity. GPs can assist by exploring possible alternatives to screen use with the adolescent. Adolescents with obesity are often socially marginalised and social media may be their main social interaction. Heavy screen use is associated with depression and social anxiety.
Increase physical activity
A physical activity habit and continued monitoring of food intake are predictors of long-term body weight loss maintenance. Most adolescents fail to meet national guidelines of 60 minutes of moderate to vigorous activity most days of the week. Many need reassurance that the feelings of breathlessness, sweating and chest discomfort they experience when they first exert themselves are not dangerous and that they should persevere in building up fitness. The goal is to build up activity in ways that are sustainable over time. Incidental walking (to and/or from school or a bus stop) and using a smart phone to monitor daily steps are some simple changes.
Sleep hygiene
Normal adolescent sleep architecture has a tendency towards delayed sleep onset and resistance to early waking.13 Most adolescents do not get enough sleep during the week and may sleep excessively during the weekend, with significant impact on eating and activity patterns. Although cross-sectional studies show shorter duration of sleep is associated with overweight and obesity in adolescents, there is no empirical evidence to support targeting sleep as a means of obesity management. However, improving sleep habits improves mood, school performance and general wellbeing, and increases energy levels to support increased daytime physical activity. Smartphone social networking use can interfere with sleep and whole-of-family strategies may be required to reduce use.
Online resources for managing adolescent obesity
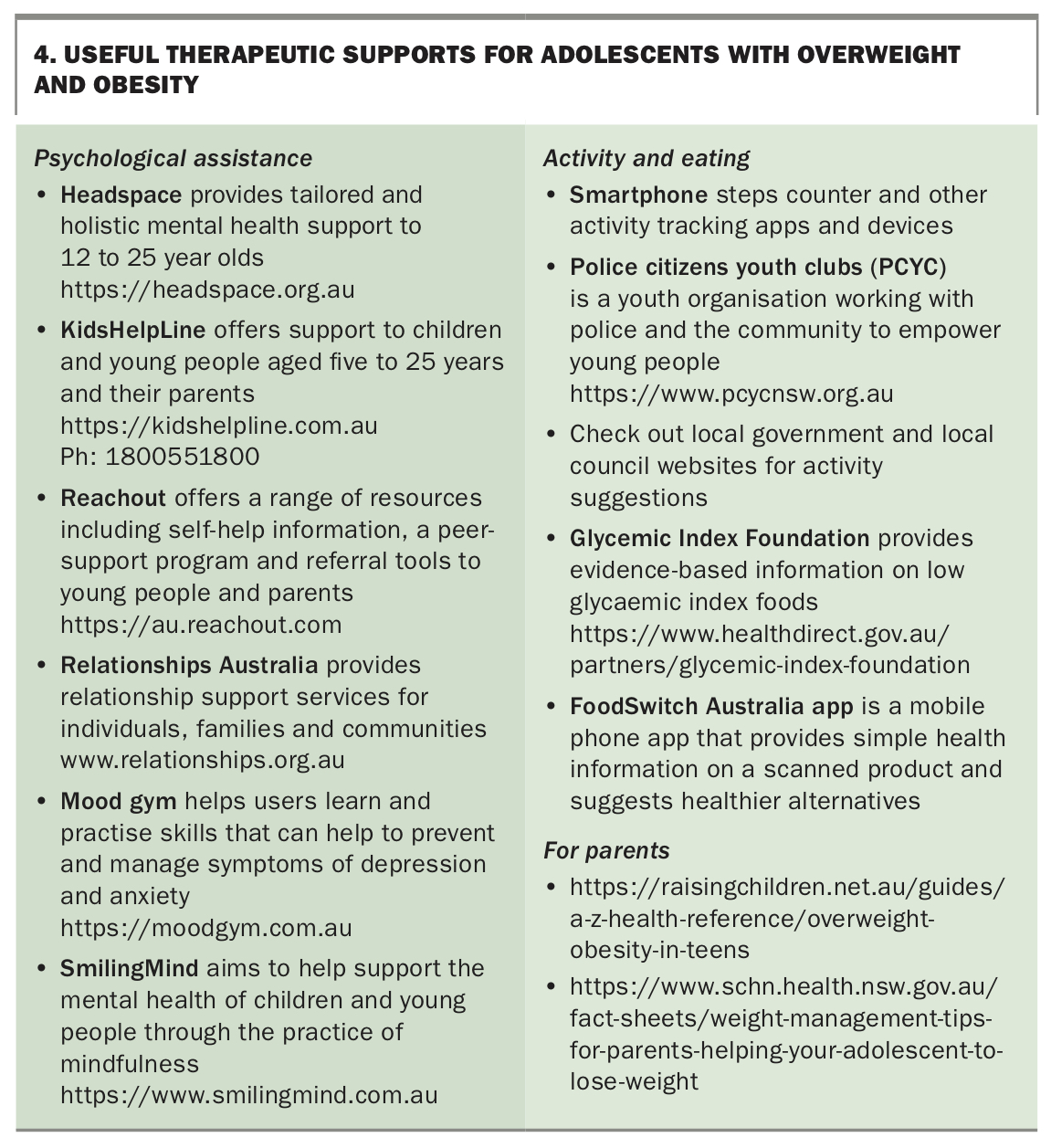
Adolescents routinely seek advice for many aspects of their life via the internet. Ask about what information they have discovered on weight management on the internet and if they think it is credible. Useful online therapeutic supports for adolescents are listed in Box 4.
{kind=link}
What helps, what hinders
In a recent qualitative study of adolescents with overweight and obesity, participants reported several perceived barriers and enablers to weight loss and healthy lifestyle.14 The most significant barriers reported were food and eating behaviours, including ease of access, hunger, stress eating and pressure from others.14 Another barrier to weight management is the struggle to increase physical activity. Many adolescents with overweight and obesity seek activity that is safe, inexpensive and fun – usually with peers. Such activities are generally not found in local playgrounds or gyms. Discussion with parents may be necessary to find solutions that work for the adolescent and their family. Internalisation of weight bias, lower self-esteem and self-worth as a result of external weight bias (which for young people includes bullying) and discrimination because of weight are more common in adolescent girls and may reduce self-efficacy.15 This may in turn hinder efforts at lifestyle modification such as increasing physical activity and dietary change.
The natural emerging autonomy in adolescents requires consideration; providing some choice around food items, refraining from nagging and negative comments, and encouraging and supporting the desired lifestyle changes. In situations where parents are separated with differing lifestyles, or not presenting a united front on weight management, adolescents are disadvantaged. The young person may also struggle if they are made to feel that they are the only member of the family that needs to address their weight and/or health.
Creating a management team and when to refer to specialist care
There are limited weight management services for adolescents associated with public or community health services. State Departments of Health, local health districts or local councils may offer group or individual programs and/or maintain a list of potential local supports (Box 4).
Adolescents with obesity are generally eligible for visits to allied health professionals including dietitians, exercise physiologists and psychologists. Approach these in the order that you and the young person agree is likely to meet their immediate needs most effectively.
As the prevalence of physical morbidity increases, so will the frequency of specialist referral, including respiratory and sleep medicine, orthopaedics and endocrinology. Androgen excess in adolescent girls may be due to possible evolving comorbid PCOS, and these young women may also have insulin resistance. Both adolescent boys and girls with dominant central adiposity are more likely to have features of the metabolic syndrome in evolution.
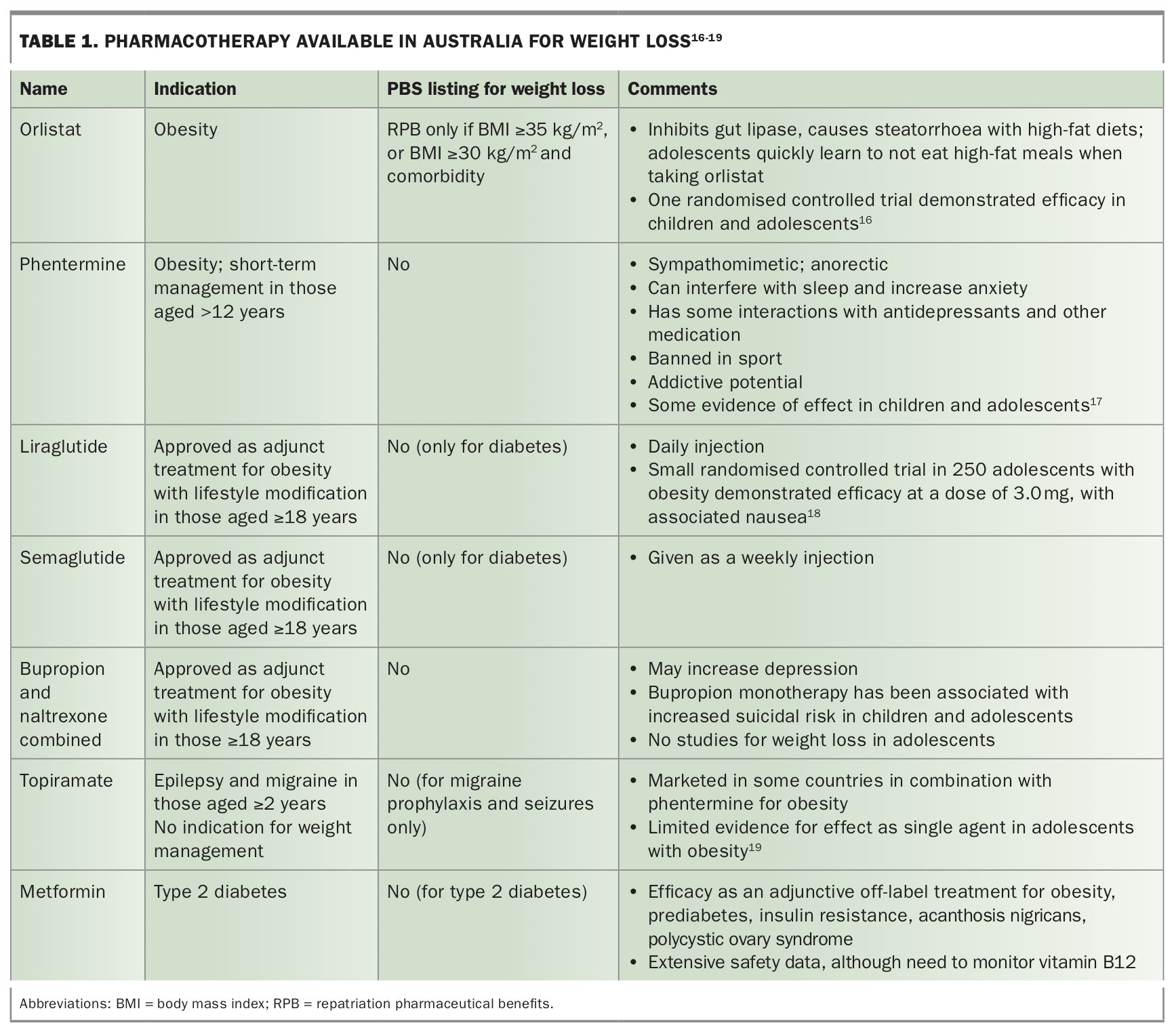
Pharmacotherapy
Table 1 summarises the therapeutic options available in Australia in 2021 for weight management.16-19 In practice, metformin is a useful off-label medication, provided it is introduced slowly to avoid gastrointestinal upset. There is empirical evidence to support a modest increase in weight loss when it is used with lifestyle modification in adolescents. It also has a preventive role in obesity and insulin resistance induced by newer antipsychotic agents such as risperidone and olanzapine.20 Metformin is an effective ovulation induction agent, as is weight loss itself, and adolescent girls should be assessed for contraception needs if this or any other pharmacotherapy is used.
{kind=link}
Bariatric surgery
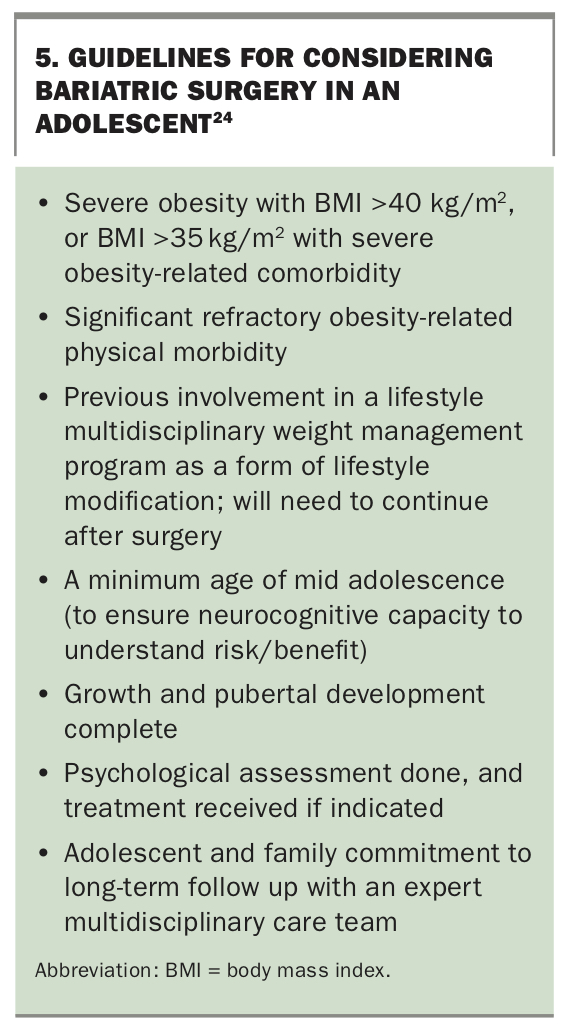
Evidence from an Australian randomised controlled trial for laparoscopic gastric banding, a systematic review and prospective data from the Teen-Longitudinal Assessment of Bariatric Surgery (Teen-LABS) trial suggest that bariatric surgery does have a place in the treatment of severe obesity in adolescents.21-23 The latter two studies also included laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass, where gastrointestinal tract anatomy is permanently altered. These procedures are also associated with a greater degree of weight loss. Around 25% of body weight was lost across the three studies, with major improvement in, or remission of, obesity comorbidities including type 2 diabetes and hypertension. However, a high percentage of adolescents had nutritional deficiencies after surgery. Data on the long-term effects of surgery in this age group are still needed. Clinical consensus guidelines for bariatric surgery in adolescents have been published in Australia and are summarised in Box 5.24
{kind=link}
Defining success and long-term outcomes
Halting weight gain is considered a success for adolescent weight management and, if there is height growth potential, may be all that is required to reduce BMI. Increasing physical fitness, changing body shape, improving metabolic markers and a sense of wellbeing are all positive indicators of changing habits, and therefore success. Weight loss and maintenance may take longer, and there may be relapse and/or regression. While waiting for stronger prefrontal cortex function, revisiting interventions that work, regular monitoring and booster sessions with the adolescent’s management team are all useful strategies to help support their weight management goals.
Conclusion
The principles for managing overweight and obesity in adolescents are similar to those for adults, with a focus on lifestyle factors being key to success in reaching long-term weight management goals. The challenge for GPs is to understand how adolescence, including puberty, lifestyle behaviours, family obesity and psychosocial factors affect weight management. A sensitive and nuanced approach is important and includes setting initial small weight-management goals with a view to transitioning to medium-to-long-term goals, a multidisciplinary approach to management and ongoing monitoring and support. MT