Obesity and weight management in women at midlife

Women in midlife have menopausal weight gain in addition to the usual causes of excess weight. The best way to achieve rapid weight loss is to use a very low energy ketogenic diet. Appetite suppression after weight loss is necessary for weight maintenance and has to be lifelong as the physiological changes leading to weight regain are long lasting.
Around 30% of adults in Australia have obesity. As well as the common causes of excess weight gain occurring in the general population, women at midlife have to cope with a further increase in weight gain caused by menopause. Because obesity is so prevalent and causes so much pathology, all general practitioners should know how to help their patients lose weight.
The average weight gain at the menopause is a modest two to three kilograms but this average hides the range of weight gain caused by menopause. Menopausal weight gain results from a transient increase in hunger and a profound reduction in spontaneous activity, which does not recover and can only be reversed by replacing oestrogen.1,2 Over time, this weight gain can lead to obesity in some women.’ Obesity in women in midlife should be treated, as it has significant health consequences including an increase in cardiovascular disease and stroke and a reduction in wellbeing.3-5
How to lose a lot of weight
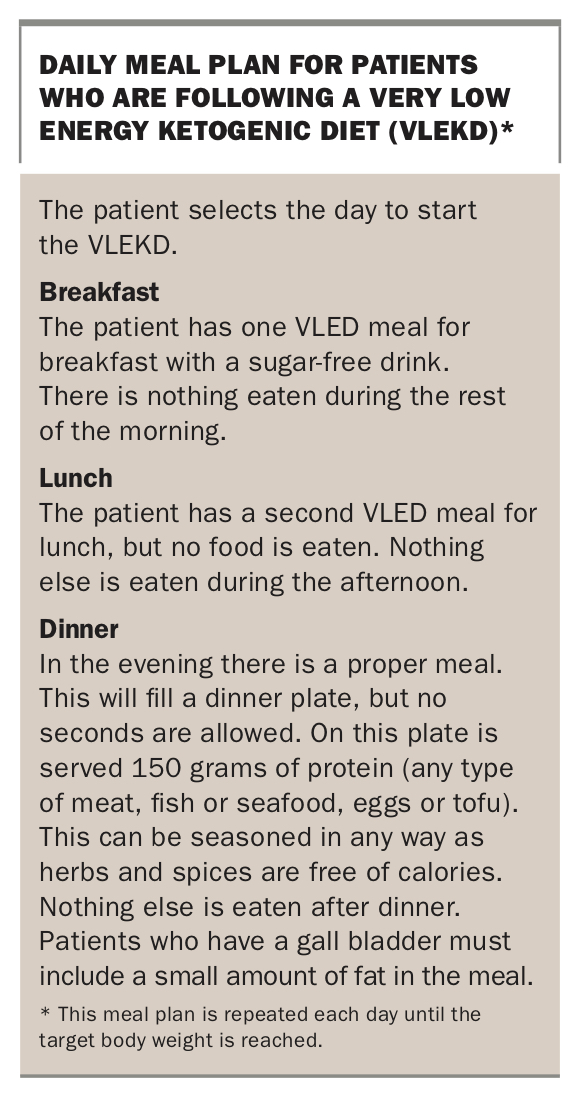
Evidence suggests that a very low energy ketogenic diet (VLEKD) is the best method to achieve rapid weight loss.6 To lose weight rapidly, it is necessary to have a large gap between energy expenditure and energy intake. This can be achieved by reducing daily energy intake to 3280 kilojoules (800 calories). The problem is that 3200 kilojoules of food does not provide all of the micronutrients we need. Therefore, this diet needs to be undertaken using a scientifically formulated VLED product, which provides daily nutritional needs with restricted calories. These products are marketed as a powder that is added to cold water and shaken, or as bars or soups.
Two VLED meals and one ‘proper’ meal should be eaten daily, with no snacking in between. A small amount of fat must be included in the meal each day if the patient still has a gall bladder. This can be a quarter of an avocado, a tablespoon of oil in a salad dressing, a few olives or a small amount of cheese. A small amount of fat is essential because the gall bladder must be emptied daily to reduce the risk of gallstone formation. An example of a VLEKD meal plan is outlined in the Box. This way of eating should be continued until the target weight is reached, after which the VLED products are slowly withdrawn and carbohydrates reintroduced to transition to a balanced diet. The patient should be advised that in the lifelong maintenance phase, all foods are allowed but portions have to be smaller than they were before starting the diet.
{kind=link}
Some patients do not tolerate VLEDs. For these individuals, VLED products can be replaced with capsules that contain all of the vitamins, metals and minerals. If using this approach, a small amount of carbohydrate-free food is needed for breakfast (an egg) and lunch (a small salad and 50 g protein). Dinner is the same as when using a VLED to obtain the nutrients.
Patients should be informed on how this diet works and what to expect when on the diet. Rapid weight loss occurs predominantly through caloric restriction, but ketosis helps. Ketosis occurs when the liver burns fat for energy. Since the liver prefers to burn glucose it is necessary to severely reduce carbohydrate intake. Increasing ingested fat is not necessary or advisable to achieve ketosis.
On the first and second day of the diet, the body makes up the missing energy intake by burning glycogen. During these two days patients may experience severe hunger. However, when the glycogen stores have been used (the morning of day 3), the body must then burn fat. When the liver is burning a lot of fat, it produces ketones, which suppress hunger by acting on the brain and controlling hunger regulating hormones and nutrients.7,8 Patients may wish to keep some protein on hand (such as a roast chicken) to nibble on in the first two days to avoid hunger. This extra protein will not delay ketosis, but after day 3 there should be no additional caloric intake.
Exercise is advisable as it helps avoid muscle loss and very slightly increases energy expenditure. Three hours per week of light exercise can prevent muscle loss when using a VLEKD.9 For those patients unable or unwilling to avoid all carbohydrates during rapid weight loss, hunger suppressing medication should take the place of ketones.
How to maintain weight loss
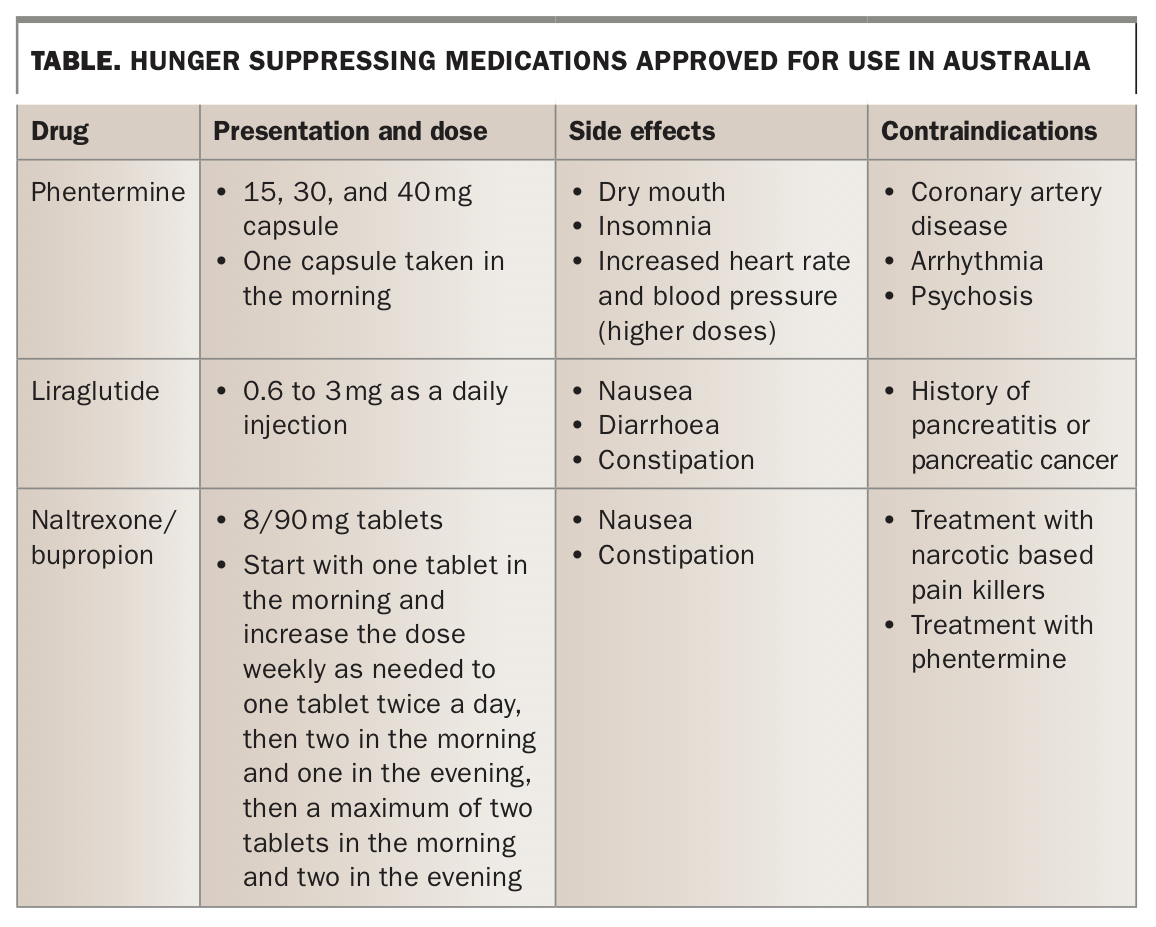
Losing weight is only the first step in this journey. There is very good evidence that most people regain weight eventually. The reason for this is that weight is predominantly genetically determined, either due to changes in gene sequence or, probably more commonly, by epigenetic mechanisms, and the body attempts to defend the weight to the genetic level.10-16 It does that by reducing energy expenditure and increasing hunger after weight loss.17,18 These changes are long-lasting with evidence showing that energy expenditure and leptin levels are still lower than baseline six years after weight loss.19-21 For this reason medication is required after rapid weight loss to suppress hunger. Medications that have been approved in Australia to suppress hunger are summarised in the Table.
{kind=link}
It is the author’s experience that there is a wide range of reactions to any medication, so a drug that works in one individual with good efficacy and no side effects may cause unbearable side effects and have little efficacy in another. Therefore, an individualised approach to drug selection is needed, which takes into account the contraindications of available pharmacotherapies and the patient’s preference. If the initially chosen medication is not effective or causes intolerable side effects, another agent can be selected. Overall, it is best to use multiple agents, each at low dose, to mimic the action of the body to reduce hunger after a meal when hormones are released transiently to suppress the drive to eat.
There are three other medications available in Australia, which are not yet approved by the TGA for weight loss: topiramate, topiramate/phentermine combination and semaglutide.22,23 The side effects of topiramate include paraesthesia, confusion, increased risk of kidney stones, glaucoma and fetal abnormalities (cleft lip). Semaglutide has the same side effects as liraglutide (Table). These may be considered for off-label use if the above therapies are unsuccessful.
Conclusion
Obesity is prevalent and causes much pathology. Women in midlife are particularly at risk of obesity due to menopausal weight gain. Weight loss is best achieved with a VLEKD and maintained with lifestyle strategies and hunger suppressing medications. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.