Everything old is new again: don’t forget about syphilis

Sexually transmitted infections
Notifications of infectious syphilis are continuing to rise. This article summarises key information on testing, treatment and follow up that is essential to primary care.
After a historical low in the 1990s, syphilis notifications have increased in Australia every year for the past 15 years. Despite a range of prevention methods and the availability of a cheap single-dose cure to which no antimicrobial resistance has developed, this infection shows no signs of slowing. Syphilis is an important disease in its own right with serious sequelae if untreated. Crucially, it is also a risk factor for HIV transmission and acquisition.
Treponema pallidum subsp. pallidum, the causative organism, is a member of the Spirochaetaceae family of bacteria. Humans are the only host, and transmission is almost entirely attributable to sexual contact and, outside of Australia, vertical transmission. Structurally, T. pallidum is spiral shaped, 0.2 µm in diameter and varies from 6 to 15 µm in length. Endoflagellae facilitate the characteristic corkscrewing movement seen under the microscope.
The evolving epidemiology of syphilis in Australia
Before the Second World War, syphilis was endemic in Australia, with notification rates of 200 per 100,000 reported in the general population. The discovery in the 1940s that penicillin was effective against T. pallidum heralded a precipitous reduction in the incidence of infection, which further decreased as safe sex became more common in the wake of the HIV/AIDS epidemic. By 2003–04 notifications of infectious syphilis had dropped to 4.2 cases per 100,000 population.
However, numbers of infectious syphilis cases in Australian cities have subsequently increased. In Sydney, for example, 16 cases of infectious syphilis were reported in 1999, with a rapid increase to 162 in 2003 and 745 in 2014. A total of 2736 cases of infectious syphilis were notified nationally during 2015, a notification rate of 11.8 per 100,000 per year.1
Syphilis infection in Australia appears to be concentrated among men who have sex with men (MSM) and Aboriginal people residing in remote communities in Northern Australia. People in these two populations constitute 16% of syphilis diagnoses.
Most MSM diagnosed with infectious syphilis live in major cities. HIV-positive MSM are disproportionately impacted; despite only 10% of MSM in urban Sydney being HIV positive, they constitute almost 50% of new syphilis notifications and 87% of reinfections.2
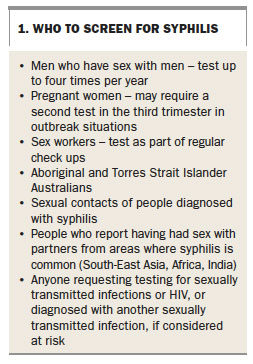
Historically, Indigenous Australians, particularly those living in remote settings, have had much higher (up to 100-fold) rates of infectious syphilis notification than the general population. After notification rates declined in 2006 there was hope that syphilis could be eliminated from remote Aboriginal communities. Unfortunately, meeting this important health equity goal was rapidly derailed by an outbreak of heterosexually acquired syphilis in the remote gulf country of Queensland. Beginning in 2011, the outbreak has now spread across Northern Australia, and syphilis diagnoses among Aboriginal Australians increased 280% between 2013 (154 cases) and 2015 (433 cases).1 In contrast to the predominance of cases being among MSM in the general population, the highest rate of notification among Aboriginal people (120/100,000/year) has occurred among women 15 to 19 years of age; and more than 10 cases of congenital syphilis have been reported in children born to these women. Recommendations for who to screen for syphilis are given in Box 1.
{kind=link}
Tests for syphilis
Serological testing for syphilis relies on well-validated, sensitive and specific treponemal tests such as enzyme immunoassay (EIA). Confirmation is provided by additional tests such as the T. pallidum particle agglutination assay (TPPA) or the fluorescent treponemal antibody absorption test (FTA-abs). These specific tests do not provide information of disease activity, and even if the patient is treated the results will normally remain positive for life. Therefore, a nonspecific test (sometimes called a nontreponemal test) such as the Venereal Disease Research Laboratory (VDRL) test or rapid plasma reagin (RPR) assay is used to provide a titre (e.g. 1:8, 1:16, 1:32 etc.). These tests detect antibodies that are formed indirectly during an infection with T. pallidum. Serial titres can assess both treatment response and reinfection. Fortunately, most laboratories will perform appropriate testing algorithms if ‘syphilis serology’ is requested on the pathology form.
In patients with genital lesions of primary syphilis, dark-field microscopy may also aid diagnosis. This requires a skilled microscopist but can achieve a sensitivity of up to 75%.3
The development of the T. pallidum polymerase chain reaction (Tp-PCR) test for early diagnosis of syphilis has opened up a new field of molecular investigations for syphilis. Tp-PCR is sensitive and specific, and has been reported to become positive before a serological response, potentially allowing more rapid treatment. The specimen is taken by rubbing a viral transport swab over a moist syphilis lesion, and is most useful in diagnosing primary disease. All states and territories have access to this test through public or private pathology services.
Clinical manifestations
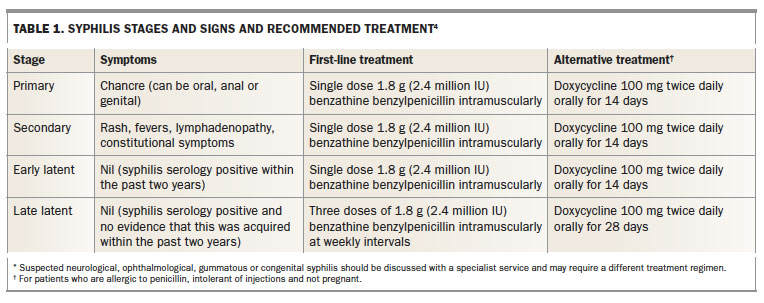
Syphilis is notorious for producing a myriad of clinical signs and symptoms and for being part of the differential diagnosis of many other diseases. However, it tends to follow a series of clinical stages, which are summarised along with treatment recommendations in Table 1.4
{kind=link}
Primary syphilis
Primary syphilis occurs between nine and 90 days after exposure with the development of the classic chancre (ulcer) at the point of inoculation, often followed by painless local lymphadenopathy. A chancre can therefore present on the vulva, cervix, penis, anus or oral cavity, depending on the type of sexual exposure; however, because three-quarters of chancres are painless they may be overlooked. Nongenital primary lesions may be mistaken for noninfectious conditions such as aphthous ulcers or anal fissures. A thorough sexual history and a high index of suspicion are therefore essential.
If available, dark-ground microscopy can afford immediate diagnosis, and a swab should be collected for Tp-PCR testing. Serological testing for syphilis is usually positive, but can be falsely negative in up to 10% of cases of primary syphilis, thus repeat serology should be performed if suspicion remains high.
The differential diagnosis of a genital ulcer includes other sexually transmissible infections such as herpes simplex virus, lymphogranuloma venereum chancroid (Haemophlius ducreyi) and donovanosis, the latter two being very rare in Australia.
Secondary syphilis
Secondary syphilis begins three to five months after infection, and a third of patients still have a residual chancre. Without treatment, symptoms of secondary syphilis may recur up to one to two years after infection. The characteristic maculopapular erythematous rash affecting the palms and soles occurs in more than 75% of patients. There may also be systemic involvement such as headache, malaise, mild fever, lymphadenopathy or sore throat.
Other common signs of secondary disease include condylomata lata (pale highly infectious elevated papules at moist body orifices), oral mucosal erosions, patchy alopecia and raised liver enzyme levels. Ophthalmological (e.g. uveitis or retinitis) and neurological complications can also occur.
Results of both specific treponemal serology and nonspecific VDRL and RPR tests are always positive in secondary syphilis. If results are negative, the diagnosis is effectively excluded.
Latent syphilis
Latent syphilis is divided into early and late latent infection. Early latent syphilis is considered infectious to sexual partners, whereas late latent syphilis is probably not infectious. A diagnosis of early latent syphilis means the patient has no signs of primary or secondary disease and has positive syphilis serology, preceded by negative serology within the past two years, a recent clinical syndrome consistent with primary or secondary syphilis, or recent sexual contact with an infectious person.
Asymptomatic seropositive patients with no evidence of acquisition within the previous two years, acquired syphilis or previous treatment are classified as having late latent infection.
Before effective antibiotic treatment was available, one in three patients with syphilis developed a manifestation of symptomatic late disease (tertiary syphilis). Manifestations were neurosyphilis, cardiovascular syphilis and late benign syphilis (gummatous disease). Patients with neurological, ophthalmological or cardiovascular signs and positive syphilis serology should be referred for specialist review.
Treatment of syphilis
A single intramuscular dose of benzathine benzylpenicillin (benzathine penicillin G) 1.8 g (2.4 million IU) has remained the first-line treatment for all stages of infectious syphilis for 70 years, without evidence of drug resistance developing. Oral doxycycline is an alternative treatment for patients who are allergic to penicillin, intolerant of injections and not pregnant. Pregnant women should be treated with a penicillin-based regimen, or desensitised if they are allergic to penicillin. Consultation with the midwifery or obstetric team is essential to ensure the baby is screened and treated if required.
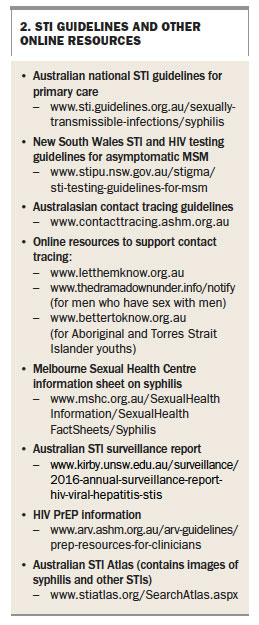
The Australian STI Management Guidelines focus on the management of syphilis in primary care (Box 2).4,5 They recommend a single 1.8 g dose of benzathine benzylpenicillin for primary, secondary and early latent syphilis, and three 1.8 g doses at weekly intervals for late latent infection. Treatment should be the same regardless of HIV status. Patients with more complicated disease (e.g. neurological or ophthalmological signs) should be referred to specialist services for management.
{kind=link}
Treatment response
Response to treatment should be monitored using the RPR or VDRL titre. A patient with a fourfold (two titre) reduction within six to twelve months is considered cured. Testing should occur at three months after treatment and be repeated three monthly. A titre that rises after treatment is most commonly due to reinfection. In case of doubt, specialist referral is recommended.
A Jarisch-Herxheimer reaction can occur three to 12 hours after treatment in response to the release of cytokines when the spirochaete is killed. It is characterised by rigors and headache, and the transient worsening of secondary lesions. Patients should be advised of this possible reaction in advance and advised to take NSAIDs as needed. The reaction usually passes within 24 hours.
Contact tracing and prevention
Contact tracing is an important component of managing sexually transmissible infections. It aims to identify and treat exposed or infected sexual partners. This has a public health benefit, but also reduces the likelihood of reinfection of the index case. The diagnosing clinician is responsible for initiating a discussion about contact tracing, which can be performed by the patient, the clinician, or using online notification services that can provide anonymity for those unwilling or unable to make personal contact (Box 2).
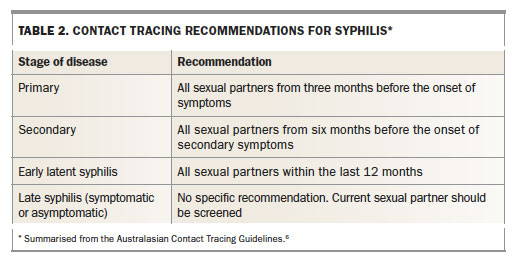
Contacts presenting within three months of exposure to infectious syphilis should be empirically treated as a case of incubating syphilis, using the same regimen as for primary syphilis because serology may be falsely negative during this period. Contacts from greater than three months previously can defer treatment until serology results are known. How far back to trace contacts depends on the disease stage and is outlined in the Australasian Contact Tracing Guidelines website (www.contacttracing.ashm.org.au) and summarised in Table 2.6
{kind=link}
All patients with syphilis should undergo a full sexual health screen, including an HIV test. Evidence-based guidelines for which tests to offer to MSM are available, and include testing high-risk men up to four times per year (see Box 2). Although condoms are not always protective against syphilis acquisition, consistent condom use is associated with a reduced incidence of infection and should be recommended. For MSM not reporting consistent condom use, a history of unprotected anal sex with a diagnosis of syphilis should prompt referral to a service able to prescribe HIV pre-exposure prophylaxis, as these men are at high risk of subsequent HIV seroconversion.
Trials of antibiotic pre-exposure prophylaxis for syphilis in people at high risk are under way, but this treatment cannot be recommended for routine care, as the efficacy of this approach lacks evidence.
Conclusion
General practitioners and nonsexual health specialists are crucial components of syphilis treatment and control. Many diagnoses of syphilis are made by primary care clinicians across Australia, including in the settings of the epidemics among urban MSM and among Aboriginal communities in Northern Australia. National guidelines for testing, treatment and contact tracing of syphilis are available and if followed make infectious syphilis very manageable in primary care. Clinicians should also make use of local sexual health services that can provide advice and support regarding management. MT
COMPETING INTERESTS: None.
References
- The Kirby Institute. HIV, viral hepatitis and sexually transmissible infections in Australia annual surveillance report 2016. Sydney: The Kirby Institute, UNSW Australia, 2016. Available online at: https://www.kirby.unsw.edu.au/surveillance/2016-annual-surveillance-report-hiv-viral-hepatitis-stis (accessed May 2016).
- Botham SJ, Ressler K, Maywood P, et al. Men who have sex with men, infectious syphilis and HIV coinfection in inner Sydney: results of enhanced surveillance. Sexual Health 2013; 10: 291-298.
- Romanowski B, Forsey E, Prasad E, Lukehart S, Tam M, Hook EW 3rd. Detection of Treponema pallidum by a fluorescent monoclonal antibody test. Sex Transm Dis 1987; 14: 156-159.
- Australasian Sexual Health Alliance. Australian STI management guidelines for use in primary care. Sydney: Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine; 2016. Available online at: http://www.sti.guidelines.org.au/sexually-transmissible-infections/syphilis (accessed May 2016).
- Templeton DJ, Read P, Varma R, Bourne C. Australian sexually transmissible infection and HIV testing guidelines for asymptomatic men who have sex with men 2014: a review of the evidence. Sex Health 2014; 11: 217-229.
- Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine (ASHM). Australasian contact tracing guidelines. Sydney: ASHM; 2016. Available online at: http://www.contacttracing.ashm.org.au (accessed May 2016).
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.