Management of common hepatobiliary disorders in pregnancy

Liver diseases
Health problems in pregnancy
Liver biochemistry results can be abnormal due to changes that occur during pregnancy. Careful history taking and examination are required to establish the cause and, if a hepatobiliary disorder is present, to determine whether it is pre-existing, coincidental or related to the pregnancy.
- Liver disease is not uncommon during pregnancy and it may be pre-existing, coincidental or pregnancy related.
- The patient’s clinical history and stage of pregnancy will help to determine the likely cause of abnormal liver biochemistry.
- Pregnancy-related liver diseases include hyperemesis gravidarum, pre-eclampsia, intrahepatic cholestasis of pregnancy, HELLP syndrome and acute fatty liver of pregnancy; they can be life-threatening and may recur in subsequent pregnancies.
- Severe pre-eclampsia with hepatic involvement, HELLP syndrome and acute fatty liver of pregnancy are indications for delivery.
- Babies born to mothers positive for hepatitis B surface antigen (HBsAg) should be given a dose of monovalent hepatitis B vaccine and hepatitis B immunoglobulin at birth.
- Breastfeeding is generally safe for mothers with hepatitis B or C but should be avoided when the nipples are cracked and bleeding.
Picture credit: © Westend61/Miriam D/Diomedia.com
The diagnosis and management of hepatobiliary disease in pregnant women can be challenging. Laboratory results are altered by normal physiological changes that occur during pregnancy and options for hepatobiliary imaging are limited. The health of both the mother and child must be considered before performing invasive procedures, prescribing new medications or planning early delivery.
In general, hepatobiliary diseases during pregnancy can be divided into three groups:
- underlying chronic liver disease (e.g. chronic viral hepatitis, autoimmune hepatitis [AIH], fatty liver disease, cirrhosis)
- coincidental hepatobiliary disease (e.g. gallstones, acute viral hepatitis, herpes hepatitis, drug-induced liver injury)
- pregnancy-related liver disease (e.g. hyperemesis gravidarum, intrahepatic cholestasis of pregnancy (IHCP), pre-eclampsia with hepatic involvement, HELLP [haemolysis, elevated liver enzymes, low platelets] syndrome, acute fatty liver of pregnancy [AFLP]).
Abnormal liver biochemistry in pregnancy
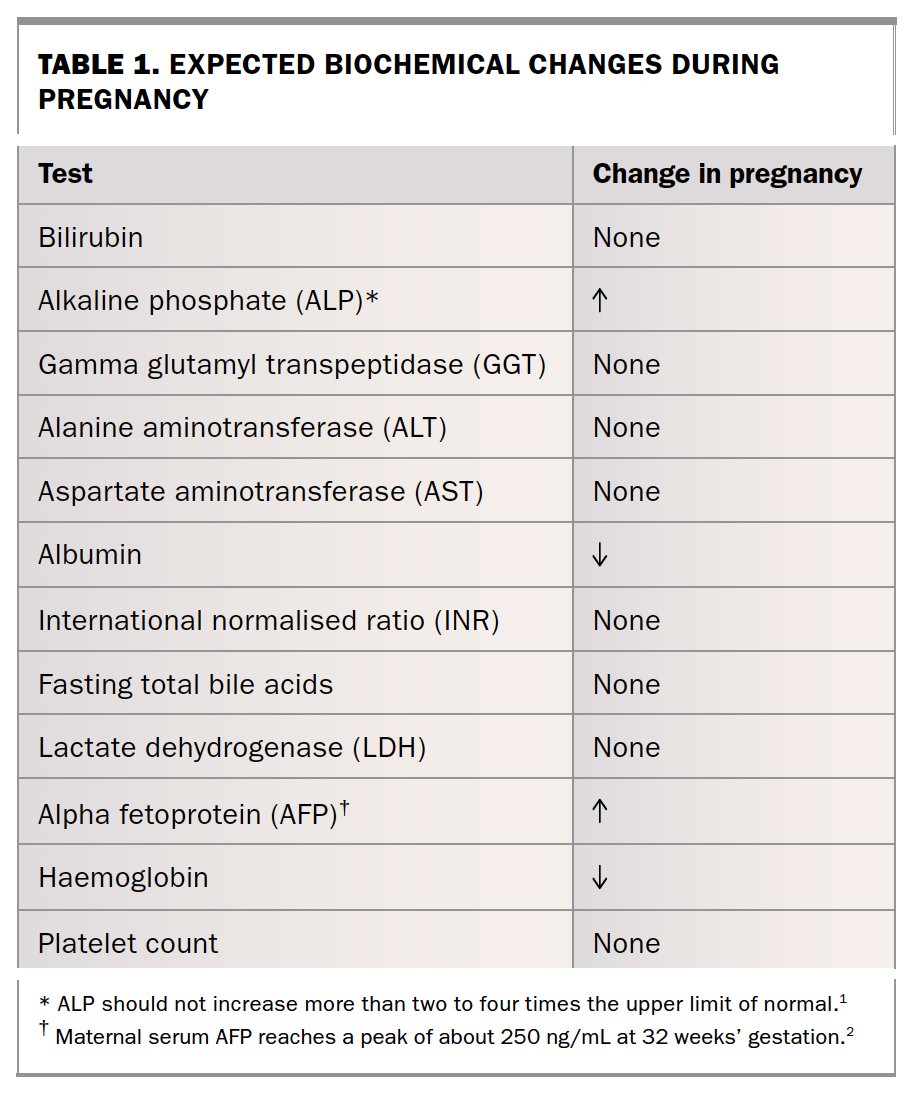
The normal physiological changes that occur during pregnancy affect several laboratory results, including liver biochemistry. An understanding of what is a normal or abnormal result is necessary when assessing pregnant women for liver disease (Table 1).1,2 Levels of alkaline phosphatase (ALP) and alpha-fetoprotein (AFP) are elevated because they are produced by the placenta. Levels of ALP may increase to two to four times the upper limit of normal.3 The maternal serum AFP concentration increases during pregnancy to a peak of about 250 ng/mL at 32 weeks’ gestation. Unexpectedly high maternal serum AFP concentrations may suggest fetal abnormalities such as neural tube defects.4
{kind=link}
Levels of alanine aminotransferase (ALT), aspartate aminotransferase (AST) and bilirubin should not increase above laboratory reference ranges during pregnancy; any elevation should be investigated further. Albumin and haemoglobin levels are lower during pregnancy due to haemodilution. Most other laboratory tests will remain within normal reference ranges even if they are slightly higher or lower than the patient’s baseline levels.5
Abnormal liver biochemistry occurs in 3 to 5% of pregnancies.5 If results are truly abnormal then the work up of the patient should be carried out in a similar fashion to that in nonpregnant women. The gestational age or trimester of pregnancy will help narrow down the differential diagnosis. Other useful information from the patient’s clinical history includes:
- associated symptoms such as nausea, vomiting, abdominal pain or pruritus
- personal history of liver disease or gallstones
- issues during prior pregnancies
- previous serological test results for chronic hepatitis
- recent use of medications or potential toxins (prescription, over the counter, herbal or recreational)
- risk factors for infective hepatitis (injecting drug use, tattoos/piercings, sexual contacts, blood transfusion, travel)
- alcohol consumption
- family history.
On physical examination, spider naevi and palmar erythema can be normal findings during pregnancy but jaundice is not.
If liver enzyme levels are elevated in a hepatocellular profile (i.e. disproportionate elevation in ALT and AST levels) then investigations for coincidental liver disease should be considered in addition to pregnancy-related liver diseases and undiagnosed chronic liver disease. Common causes of elevated liver enzyme levels in nonpregnant women should also be considered, such as nonalcoholic fatty liver disease and alcohol abuse. Women with nonalcoholic fatty liver disease often have mild to moderate elevations in levels of transaminases (usually with an AST to ALT ratio less than one) and may also have mild elevations in gamma glutamyl transpeptidase (GGT) and ALP levels. Evidence of alcohol consumption may be apparent from the clinical history but some women may not disclose this information. Biochemical changes that suggest alcohol consumption include an elevation in GGT level with a disproportionate elevation in AST compared with ALT levels.
If the elevation of liver enzymes is in a cholestatic pattern (i.e. disproportionate elevation in levels of ALP and GGT) then an abdominal ultrasound examination should be performed to identify any biliary obstruction. Other causes of cholestasis to consider include use of medications or toxins, and undiagnosed liver diseases such as primary biliary cholangitis (formerly known as primary biliary cirrhosis) and primary sclerosing cholangitis.
A mixed hepatocellular/cholestatic pattern of liver biochemistry is commonly encountered; all causes of liver disease must be considered.
Coincidental hepatobiliary disease
Acute viral hepatitis
Acute viral infections typically result in elevated levels of transaminases. Investigations to consider in pregnant women with elevated transaminase levels include: hepatitis A virus (HAV) immunoglobulin M (IgM); hepatitis B surface antigen (HBsAg) and hepatitis B core IgM; anti-hepatitis C virus (HCV; if positive then HCV RNA testing); Epstein-Barr virus (EBV) IgM; cytomegalovirus (CMV) IgM; hepatitis E virus (HEV) IgM; and herpes simplex virus (HSV) polymerase chain reaction (PCR) testing.
The management of hepatitis B and C during pregnancy is discussed later in this article. Acute hepatitis A has a similar disease course in both pregnant and nonpregnant women. Maternal and fetal outcomes are excellent, although severe disease late in pregnancy may be associated with an increased rate of premature birth.6,7 The illness is usually self-limiting and the management is supportive. Mother-to-child transmission of HAV infection is extremely rare; however, administration of HAV Ig to the neonate should be considered if maternal infection occurs within two weeks of delivery.5
Although HEV infection is more common in resource-limited countries, it is important to consider during pregnancy because it is associated with high maternal and fetal mortality. Early recognition is essential to providing appropriate supportive care for the mother and child.5
Hepatitis due to HSV infection is rare but carries a high mortality rate during pregnancy. Typical features include a prodrome of fevers, upper respiratory tract symptoms, mucocutaneous lesions (present in more than 50% of cases) and significantly elevated levels of transaminases despite a normal bilirubin level (anicteric hepatitis). If suspected, testing for HSV by PCR is recommended given the limited sensitivity and specificity of HSV IgM. If HSV hepatitis is suspected then empirical therapy with intravenous aciclovir should be commenced.5
Biliary stones and pancreatitis
Mild, transient abdominal pain is common during pregnancy.8 It is usually musculoskeletal pain, triggered by anatomical changes that occur over the course of pregnancy. Severe or constant pain may result from more sinister pathologies, particularly when pain is accompanied by symptoms such as nausea, vomiting, jaundice, fevers or vaginal bleeding. Diseases not unique to pregnancy that present with abdominal pain include gallstones, hepatitis infection, peptic ulcer disease, gastro-oesophageal reflux, appendicitis and severe constipation. Pregnancy-related liver diseases and other pregnancy-related conditions (e.g. miscarriage, ectopic pregnancy, chorioamnionitis, placental abruption, uterine rupture and labour) may also cause abdominal pain and should be considered.
Gallstones may present with biliary colic or complicated gallstone diseases, such as acute cholecystitis, gallstone pancreatitis, symptomatic choledocholithiasis or cholangitis, and can usually be identified on abdominal ultrasound examination. Abdominal ultrasound has a sensitivity of 95% for the detection of gallstones.5 If ultrasound is nondiagnostic then magnetic resonance cholangiopancreatography (MRCP) can be used. MRCP does not require contrast agents such as gadolinium, which crosses the placenta and may harm the fetus.5 Most guidelines recommend only using MRCP during the second and third trimesters because there are limited data on its safety during the first trimester.5
Gallstones are more common during pregnancy because their formation is enhanced by hormonal changes that lead to cholesterol supersaturation of bile and slowed gallbladder emptying. Acute cholecystitis during pregnancy is generally managed surgically with an early laparoscopic cholecystectomy.5 Conservative management of acute cholecystitis is associated with recurrent symptoms, repeat hospitalisations and maternal and fetal complications.5,9,10 Gallstone pancreatitis, symptomatic choledocholithiasis and cholangitis may result in poor fetal outcomes without early intervention.5,9 When early endoscopic retrograde cholangiopancreatography (ERCP) is performed, fetal radiation exposure should be minimised by limiting fluoroscopy time and lead shielding of the fetus.5 Women in the second and third trimesters should be placed in the left pelvic tilt or left lateral position during ERCP to avoid vascular compression.5
Liver diseases related to pregnancy
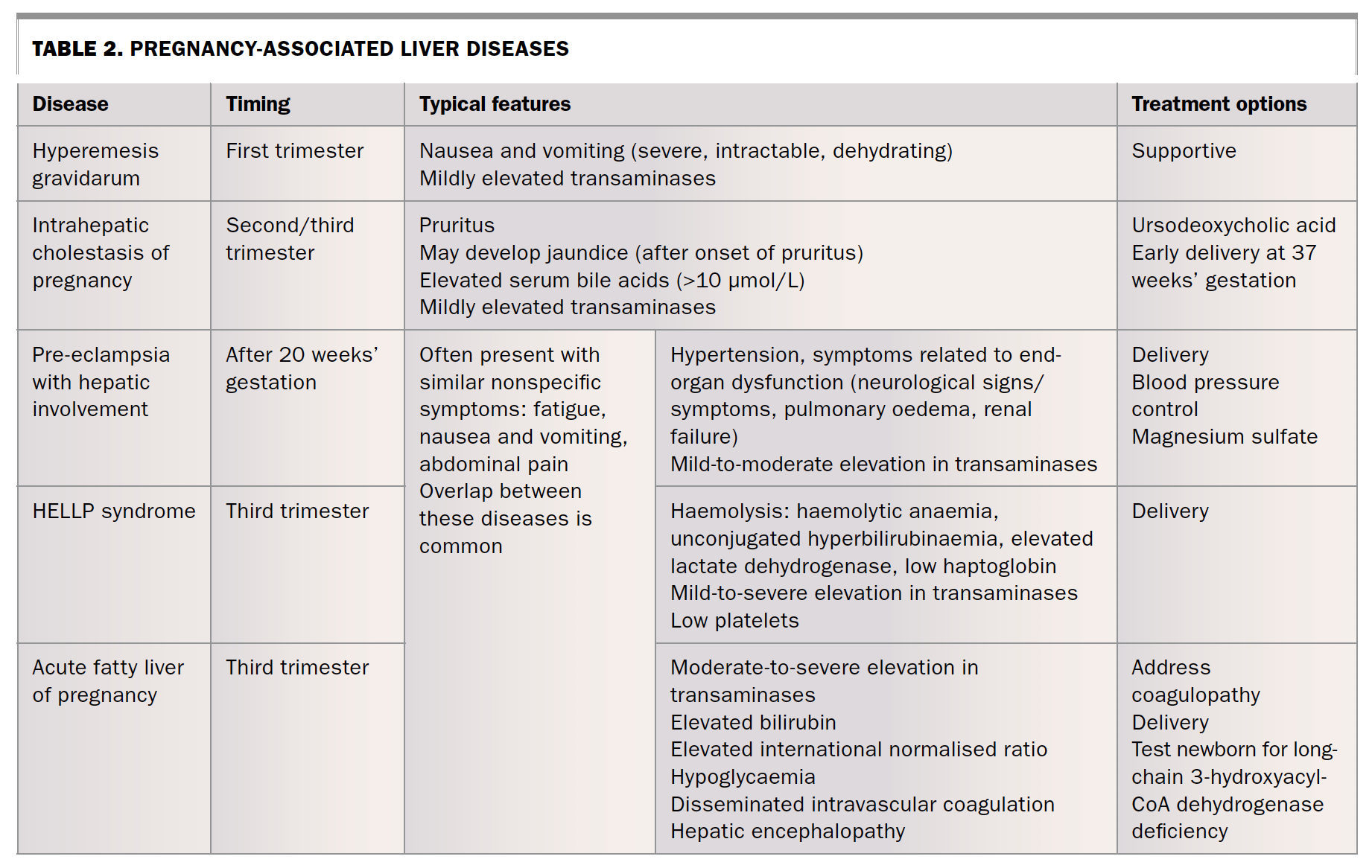
Several liver diseases are unique to pregnancy (Table 2). They can usually be diagnosed by assessing the gestational age of the pregnancy, associated signs and symptoms and the pattern of liver test abnormalities, and by reviewing other laboratory results.
{kind=link}
Hyperemesis gravidarum
Hyperemesis gravidarum presents with severe, intractable, dehydrating nausea and vomiting that begins during the first trimester of pregnancy. Nausea and vomiting that begins after the first trimester should prompt investigation for an alternative explanation. About 50% of women requiring admission to hospital for hyperemesis gravidarum have mildly elevated levels of transaminases (typically less than 300 U/L), with the degree of elevation correlating with the severity of nausea and vomiting.5
Elevations in bilirubin level are not typical in women with hyperemesis gravidarum. However, Gilbert’s syndrome is not uncommon and affected women may develop unconjugated hyperbilirubinaemia in the context of fasting and dehydration from hyperemesis gravidarum.11 Other laboratory results may suggest acute kidney injury and deranged electrolytes.
Management of hyperemesis gravidarum is supportive with dietary modification, avoidance of triggers and consideration of antiemetic therapy. Women who are unable to maintain adequate oral intake should be admitted to hospital for intravenous rehydration, electrolyte replacement and nutritional support.12 Antiemetics that are safe to use during pregnancy include a combination of pyridoxine (vitamin B6) and doxylamine, and short courses of metoclopramide, prochlorperazine, promethazine or ondansetron. Intravenous and intramuscular routes can be used when symptoms preclude oral therapy.13 Liver biochemical abnormalities resolve after the vomiting subsides; persistent elevation requires investigation for another cause.5
Intrahepatic cholestasis of pregnancy
Women with IHCP present with pruritus that begins during the second or third trimester. The pruritus is usually generalised but can be more severe on the palms and soles, and is worse at night. Some women develop jaundice (less than 25%), but only after the onset of pruritus.5 If jaundice precedes pruritus then an alternative diagnosis should be considered. Biliary obstruction is not seen on abdominal ultrasound in women with IHCP.14
A diagnosis of IHCP is supported by elevated levels of maternal bile acids (more than 10 µmol/L). A mild elevation in levels of transaminases is typical (usually less than 300 U/L), although levels may reach values more than 1000 U/L.5 The serum GGT level is usually normal or only mildly elevated, helping differentiate IHCP from biliary obstruction. Hepatic synthetic function remains normal; the international normalised ratio (INR) will only be elevated in severe cases with associated fat malabsorption and vitamin K deficiency. Vitamin K should be replaced before delivery if the INR is elevated.14
Although maternal prognosis is excellent, IHCP is associated with fetal morbidity and mortality. The main complications are premature birth and intrauterine fetal death.15 Higher levels of bile acids correlate with worse fetal outcomes, with most complications occurring with levels of more than 40 µmol/L.16 Treatment consists of symptom control for the mother and early delivery to reduce fetal morbidity and mortality. Ursodeoxycholic acid at a dose of 10 to 15 mg/kg is well tolerated and safe.5,14 It will improve pruritus and maternal liver function tests and may improve fetal outcomes.17 Intrauterine fetal death generally occurs during the last month of pregnancy and early delivery at 37 weeks is recommended.5 Earlier delivery may be considered on an individual basis after weighing the risks of prematurity against the risks of sudden death. Pruritus usually resolves a few days after delivery and liver enzymes return to normal within a few weeks.14 Delayed resolution should prompt consideration of other hepatobiliary diseases. Cholestatic liver diseases (including primary biliary cholangitis and primary sclerosing cholangitis) and chronic HCV infection may also present with pruritus late in pregnancy.18 Mild IHCP may recur in up to 70% of subsequent pregnancies.14
Pre-eclampsia, HELLP syndrome and acute fatty liver of pregnancy
Pre-eclampsia with hepatic involvement, HELLP syndrome and AFLP may present with similar clinical features. Women may be asymptomatic or may experience nonspecific symptoms such as fatigue, nausea and vomiting, and right upper quadrant pain. HELLP syndrome and AFLP generally develop during the third trimester, whereas pre-eclampsia may present as early as 20 weeks’ gestation.19
There is significant overlap between these diseases. Up to 20% of women with severe pre-eclampsia will develop HELLP syndrome.5 Although uncommon, HELLP syndrome may also occur without any features of pre-eclampsia. About 50% of women with AFLP will have features of pre-eclampsia and may also have overlapping features of HELLP syndrome.19
Pre-eclampsia and HELLP syndrome
Pre-eclampsia is characterised by new-onset hypertension with either proteinuria or end-organ dysfunction after 20 weeks’ gestation. Hepatic involvement occurs in about 10% of affected women and elevates the diagnosis to ‘severe pre-eclampsia’.19 Women may present with nonspecific symptoms (e.g. fatigue, nausea, vomiting, right upper quadrant pain) or with signs and symptoms due to other end-organ dysfunction (e.g. neurological signs and symptoms, pulmonary oedema, renal failure). Levels of transaminases are often mildly to moderately raised (often up to 500 U/L), but higher elevations may occur. Elevations in bilirubin levels are uncommon. Although the degree of elevation in liver enzymes parallels the risk of adverse maternal outcomes, it does not correlate with fetal outcomes.5
HELLP syndrome usually presents during the third trimester and is recognised by a typical pattern of blood results including haemolysis, elevated liver enzyme levels and low platelet levels. Levels of transaminases may be mildly to moderately increased; however, severe elevations are more common than in pre-eclampsia with hepatic involvement alone (at times more than 1000 U/L). Haemolysis can be recognised by peripheral blood film changes (e.g. microangiopathic anaemia with schistocytes), unconjugated hyperbilirubinaemia, elevated lactate dehydrogenase levels and reduced haptoglobin. Serious complications, including hepatic infarction, subcapsular haematoma and hepatic rupture, are more common in women with HELLP syndrome than in those with pre-eclampsia with hepatic involvement alone.
A diagnosis of severe pre-eclampsia with hepatic involvement or HELLP syndrome is an indication for delivery. Delivery is the only curative treatment and should be performed promptly for pregnancies at 34 weeks’ gestation or longer. Although conservative management may be reasonable for a select group of pregnancies less than 34 weeks, delivery should be considered if there are nonreassuring fetal tests or features of severe maternal disease (e.g. multiorgan dysfunction, disseminated intravascular coagulation, hepatic infarction or haemorrhage).19 Corticosteroids have a role in accelerating pulmonary maturity in the fetus, but do not alter the progression of liver dysfunction. Other aspects of management include blood pressure control and intravenous administration of magnesium sulfate for seizure prevention. If severe thrombocytopenia is present (less than 50 x109/L) then platelet transfusion should be considered before delivery.5 Hepatic rupture is a rare, catastrophic complication that requires surgical and/or interventional radiological management.
Acute fatty liver of pregnancy
AFLP occurs almost exclusively during the third trimester.19 It is important to recognise because it can rapidly progress to acute liver failure. A typical pattern of clinical and laboratory results is sufficient to make a diagnosis of AFLP. Typical symptoms are fatigue, anorexia, nausea and vomiting, upper abdominal pain and jaundice. Features of pre-eclampsia will be detected in 50% of affected women and hepatic encephalopathy is a late clinical feature.
Transaminases are typically moderately elevated (about 300 to 500 U/L) in women with AFLP, but levels more than 1000 U/L can occur. Other laboratory findings include hyperbilirubinaemia, coagulopathy (elevated INR) and hypoglycaemia. Thrombo-cytopenia, disseminated intravascular coagulation and renal dysfunction may also be detected.
Prompt delivery is the only curative treatment for AFLP. The mother should be stabilised and coagulopathy reversed during and after delivery. Women who continue to deteriorate despite delivery should be evaluated for liver transplantation.5
A diagnosis of AFLP also has implications for the child. About 20% of women who develop AFLP carry a child with a deficiency in long-chain 3-hydroxyacyl-CoA dehydrogenase (LCHAD).20 All newborns from pregnancies complicated by AFLP should be tested for this. Newborns with LCHAD deficiency are at risk of hypoketotic hypoglycaemia and fatty liver. Dietary modification is required and significantly reduces fetal morbidity and mortality.19
Pre-existing liver diseases
Hepatitis B
All pregnant women should be screened for chronic hepatitis B virus (HBV) infection at their first antenatal visit.21,22 Women who are positive for hepatitis B surface antigen (HBsAg) should have their disease staged by assessment of liver biochemistry, hepatitis B envelope antigen (HBeAg), hepatitis B envelope antibody (HBeAb) and viral load (HBV DNA). The viral load must be established before the third trimester to allow for timely initiation of antiviral therapy when required. Most women of childbearing age will be in the immune-tolerant phase; however, as more women enter pregnancy at older ages, increasing numbers of pregnant women are in the immune-clearance phase.22
The risk of vertical transmission of HBV is as high as 90% without immunoprophylaxis. The risk is highest among women who are positive for HBeAg and/or have a high HBV DNA level.5 All infants born to HBsAg-positive women should be given a dose of monovalent HBV vaccine and hepatitis B immunoglobulin (HBIG) at birth, concurrently but in separate thighs. The HBV vaccination schedule should be completed with three subsequent doses of an HBV-containing vaccine at 2, 4 and 6 months of age.21
In addition to standard active–passive immunoprophylaxis, antiviral therapy should be offered to women with a high viral load (over 200,000 IU/mL or over 1,000,000 copies/mL) to prevent mother-to-child transmission.5,21 This viral load threshold is a conservative recommendation. Therapy should be commenced early in the third trimester (28 to 32 weeks’ gestation) to allow sufficient time for the viral load to decrease, even if delivery occurs earlier than expected.15 Although the safety data are somewhat limited, current evidence suggests that tenofovir is safe to use in pregnant women with chronic HBV infection.22 The safety profile, potency and low risk of resistance make tenofovir a suitable first-line therapy.21,22
The optimal time to stop antiviral therapy is not clear. However, Australian guidelines recommend continuing therapy until six or 12 weeks postpartum, partly because of the risk of postpartum flares.21,22 When antiviral therapy is stopped, women should be monitored for hepatic flares by checking liver biochemistry. Most flares will settle without reintroduction of antiviral therapy.22
Some women will already be taking antiviral therapy for HBV infection before becoming pregnant. The appropriateness of therapy should be re-evaluated and a decision made on whether to continue it throughout pregnancy. For women requiring ongoing antiviral therapy, switching to tenofovir should be considered.22 Women who do require ongoing therapy should be educated on the safety profile of tenofovir and the potential consequences if therapy is stopped inappropriately.
Infants who receive HBIG and the first dose of HBV vaccine at birth can be breastfed.21 Breastfeeding is also considered to be safe among women who continue tenofovir after birth; however, long-term safety data are limited. Although low levels are present in breast milk, they are unlikely to cause significant consequences.22
Infants born to mothers with chronic HBV infection should have HBsAb and HBsAg levels measured three to 12 months after completing the primary vaccine course, at 9 to 18 months of age.21 Testing should not be performed before 9 months of age to avoid detection of HBsAb from HBIG given at birth.
Hepatitis C
The Royal Australian and New Zealand College of Obstetricians and Gynaecologists recommends that all pregnant women should be screened for chronic HCV infection by testing for HCV antibodies at the first antenatal visit.23 Women with positive serology need HCV RNA testing to confirm persistent infection. The risk of mother-to-child transmission is about 5% for chronic HCV infection, significantly lower than the risk of vertical transmission for chronic HBV infection.6,23
Although new direct-acting antivirals against HCV are now available, they do not have sufficient safety data for routine use during pregnancy.24 Ideally, women with chronic HCV infection should have their infection treated before becoming pregnant. Those identified during pregnancy as being infected can be linked to a viral hepatitis service for treatment after pregnancy. With new direct-acting antivirals, high rates of cure from HCV infection can be achieved with well-tolerated, simple, eight to 12-week courses of oral medications for patients without cirrhosis.
Infants born to HCV-positive mothers should be screened for HCV infection. The method and timing of testing for the infant are influenced by several factors. Maternal IgG antibodies may cross the placenta and the presence of anti-HCV antibodies in the infant does not necessarily indicate infection. It may take more than 12 months for these passively acquired maternal antibodies to clear. In addition, infants infected during delivery may not have detectable HCV RNA until several weeks after birth. A reasonable approach is to test for anti-HCV antibodies at 18 months of age; if positive then HCV RNA should be checked.25
With both HBV and HCV infections, invasive procedures such as amniocentesis, chorionic villus sampling, use of fetal scalp electrodes and fetal scalp blood sampling may increase the risk of vertical transmission and should be avoided if possible.5 If invasive procedures are required then women need to be counselled on the potential risk of transmission. HBV or HCV infection is not an indication for a caesarean section; the mode of delivery should be based on maternal preference and obstetric indications.5,21,23
The risk of transmission of HBV and HCV during breastfeeding is negligible and women should be encouraged to breastfeed. However, care should be taken to prevent bleeding from cracked nipples; breastfeeding should be avoided if this occurs.5,21,23
Autoimmune liver disease
AIH is more common in women than in men and may present during the childbearing years. Pregnant women with AIH have a higher risk of fetal loss, premature birth and low birth weight. These risks are highest when their disease is not under control.26 AIH is generally treated with azathioprine and/or corticosteroids; both are considered safe to continue during pregnancy.5 Primary biliary cholangitis may also occur in pregnant women. There is limited evidence supporting the use of ursodeoxycholic acid therapy for primary biliary cholangitis during pregnancy.5,27 When ursodeoxycholic acid is used to treat intrahepatic cholestasis of pregnancy, it is commenced in the second or third trimester. Although the safety data are lacking during the first trimester, current international guidelines recommend continuing ursodeoxycholic acid throughout pregnancy as the benefits of disease control likely outweigh potential risks.5
Cirrhosis
Women with cirrhosis have significantly higher rates of adverse fetal and maternal outcomes. Although women with cirrhosis have reduced fertility, pregnancy is possible, especially with advances in assisted reproductive technology.1,5 The decision to conceive ultimately lies with the patient; however, the significant risk of maternal mortality must be conveyed to any woman with cirrhosis and portal hypertension contemplating pregnancy. Adverse fetal outcomes include a higher rate of fetal loss and premature birth.1 Maternal morbidity and mortality is increased, with poor outcomes correlating with higher MELD (model for end-stage liver disease) scores at conception. The severity of portal hypertension influences the maternal risk with the major concern during pregnancy being worsening of portal hypertension and acute variceal haemorrhage. Other complications of cirrhosis such as ascites and hepatic encephalopathy may also occur.2,28
Variceal haemorrhage is the most common cause of maternal morbidity and mortality, occurring in up to 30% of pregnant women with cirrhosis.5 An episode of variceal bleeding has a maternal mortality rate of up to 50%.1,5 A variceal bleed may occur at any stage; however, the period during labour and delivery carries the highest risk.1 Women with suspected portal hypertension who are planning pregnancy should be screened for varices with an endoscopy. Women should be referred early during pregnancy as a series of endoscopies with variceal banding may be required.
For women who are already pregnant, the optimal approach is uncertain. Given the high risk of maternal morbidity and mortality from variceal bleeding, most guidelines recommend that women with suspected portal hypertension undergo a gastroscopy during the second trimester.5 The benefits likely outweigh the small risks associated with sedation and the procedure. The second trimester is thought to be the ideal time for a gastroscopy because it is after organogenesis has occurred and before the period of highest risk. If large varices are detected then band ligation and/or administration of nonselective beta blockers such as propranolol should be considered.5 Propranolol appears to be safe in pregnant women; however, infants should be monitored for side effects including neonatal bradycardia.
{kind=link}
Acute variceal haemorrhage during pregnancy is managed in the same way as for nonpregnant women. Urgent endoscopic haemostasis, antibiotic prophylaxis and intensive support are required for the mother and fetus.5
The optimal mode of delivery for women with cirrhosis is uncertain. Caesarean section carries a risk of bleeding in women with portal hypertension and coagulopathy. Prolonged labour and Valsalva manoeuvres during delivery may be associated with an increased risk of variceal haemorrhage. The mode of delivery should be individualised based on patient preference, obstetric indications, risks of bleeding, surgical site complications and the likelihood of variceal haemorrhage.1
Pregnancy after liver transplantation
After liver transplantation, women often regain fertility rapidly and pregnancy outcomes are generally favourable for both the mother and infant. Risks include a higher rate of prematurity, fetal growth restriction, gestational diabetes, hypertensive disorders and pre-eclampsia.29
Long-term immunosuppression is necessary after liver transplantation. Most experts advise women to delay conception until at least one year post-transplantation.1,5 This allows for stabilisation, use of lower doses of immunosuppressive medications and a lower risk of acute cellular rejection and ensures pregnancy occurs during a period with lower rates of opportunistic infections. The risk of using immunosuppressive medications during pregnancy must be considered. In general, women should continue their immunosuppressive medications except for mycophenolate.5 Any woman considering pregnancy after transplantation should consult with their transplant team before attempting to conceive.
Conclusions
Abnormal liver biochemistry results are not uncommon during pregnancy and may reflect pre-existing, coincidental or pregnancy-related liver disease. Careful history taking and examination in addition to further investigation generally will establish the cause. Treatment depends on the diagnosis and at times involves prompt delivery. Management decisions often require input from the patient, family practitioner, obstetrician, gastroenterologist and haematologist to achieve the best possible outcome for mother and baby. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.