Syncope: benign or sinister?

Heart diseases
In most patients, syncope is due to simple fainting (vasovagal syncope) and is benign. However, syncope may also be the presentation of life-threatening illness. It is essential to recognise patients with syncope who are at high risk of cardiac events. Most of these can be successfully treated, but they must be diagnosed and managed in a timely manner.
- Syncope is defined as a transient loss of consciousness due to cerebral hypoperfusion, characterised by rapid onset, short duration and complete spontaneous recovery. The mechanism of cerebral hypoperfusion is usually hypotension.
- All patients presenting with syncope should be classified as either high or low risk of a malignant cardiac cause.
- In most patients, the cause of syncope can be diagnosed from a detailed history, physical examination, postural blood pressure measurements and a 12-lead ECG.
- Vasovagal syncope (fainting) is the most common cause of syncope in all age groups.
- Patients with syncope in the setting of structural heart disease or an abnormal ECG are at high risk of cardiac syncope, and require prompt investigation.
- Patients with syncope during exercise (rather than after cessation of exercise) are at high risk of adverse cardiac events, such as sudden death.
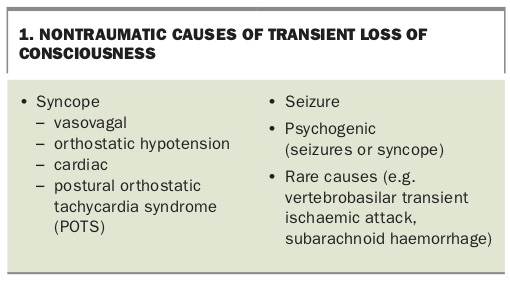
Syncope is common, experienced by 30% of the population at least once in their lives. It is defined as a transient loss of consciousness (TLOC) due to cerebral hypoperfusion, characterised by rapid onset, short duration and complete spontaneous recovery.1,2 Other nontraumatic causes of TLOC that must be distinguished from syncope are shown in Box 1. In particular, syncope must be distinguished from seizures, and these terms should not be used interchangeably.
{kind=link}
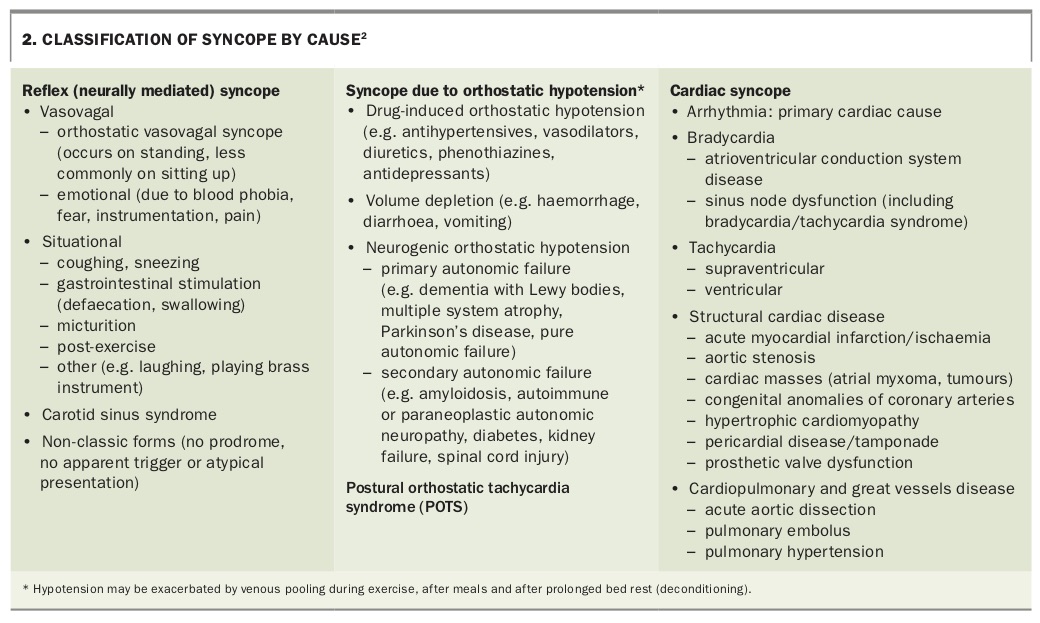
The clinical presentation of syncope and the differential diagnosis reflect the physiological definition. Causes of syncope are summarised in Box 2.2 Vasovagal syncope (fainting) is the most common cause across all age groups. It is crucial to differentiate vasovagal syncope from malignant cardiac causes of syncope.
{kind=link}
This article describes how to assess patients presenting with syncope and to stratify their risk of a cardiac cause. Six patient histories illustrate a range of noncardiac and cardiac causes of syncope, and their assessment and management.
Assessing patients with syncope
The initial steps of assessment for patients presenting with syncope are:
- take a detailed history
- conduct a physical examination
- record a 12-lead ECG
- measure supine and standing blood pressure.
History taking is the most important part of assessment; in 90% of cases, the diagnosis is made on history taking. The first step is to establish that TLOC has occurred. This is defined by four main criteria:
- short duration (limit of five minutes)
- abnormal motor control
- loss of responsiveness (from witness reports)
- amnesia to the loss of consciousness.
The duration of TLOC is often reported inaccurately by both patients and witnesses. Older people are more likely to have amnesia to events and are also more likely to lose awareness of loss of consciousness even when it has occurred. Therefore, falls in older people who do not have amnesia are unlikely to be TLOC. However, a lack of awareness of loss of consciousness does not rule out TLOC and syncope. The history of the event from the patient and witnesses must support the above definition of syncope. The general medical history should provide insight into potential causes of orthostatic hypotension, such as dehydration, drugs and Parkinson’s disease (Box 2).
A detailed history should incorporate the following key questions:
- What were you doing at the precise time that symptoms or syncope began or occurred? Did the episode occur during exercise or after? Were you sitting, standing or in motion? What had you been doing before the event?
- Describe the very first thing you felt when you recognised something was not right.
- Describe in detail step by step the evolution of what occurred.
- What was the time line? (Try to establish a clear time line and duration from symptom onset to recovery.)
- How rapid was recovery?
- How long did post-event confusion or disorientation last if at all?
- Did you have any cardiac symptoms before, during or after (e.g. palpitations, chest pain)?
- Have you had any previous episodes or a family history of sudden death?
Vasovagal syncope: classic features
Classic vasovagal syncope has the following typical features on history taking:
- It usually occurs while the patient is standing or seated.
- It may have a situational trigger such as micturition, pain, coughing or emotional stress.
- Patients describe feeling hot, rising heat, nausea, sweating, palpitations or faster heartbeat, seeing stars and vision greying out.
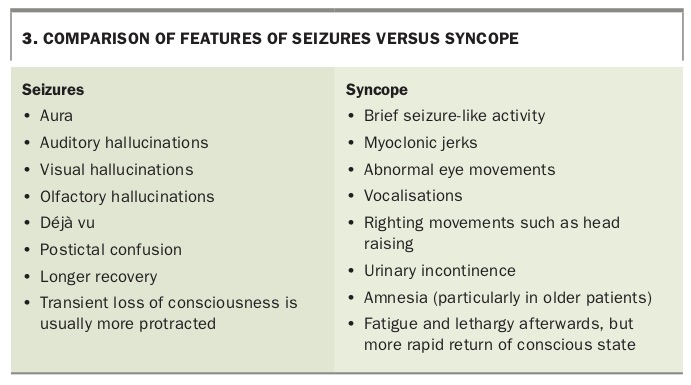
Not all patients with vasovagal syncope have all of these typical features. Witnesses may describe pallor, eyes rolling back and abnormal jerking movements in the limbs (frequently confused with epilepsy). It is common for the pulse to be difficult to feel because of poor cardiac output. This may be exacerbated by marked bradycardia and asystole, which may occur in some forms of vasovagal syncope. Loss of urinary and occasionally bowel control may occur and is not synonymous with a seizure. Cerebral hypoperfusion can result in seizure-like activity, including myoclonic jerks, head turning and vocalisations that may mimic epilepsy. However, the seizure-like activity is short lived and there is no prolonged postictal confusion. Features of seizures are compared with those of syncope in Box 3.
{kind=link}
Cardiac causes of syncope: the crucial role of risk stratification
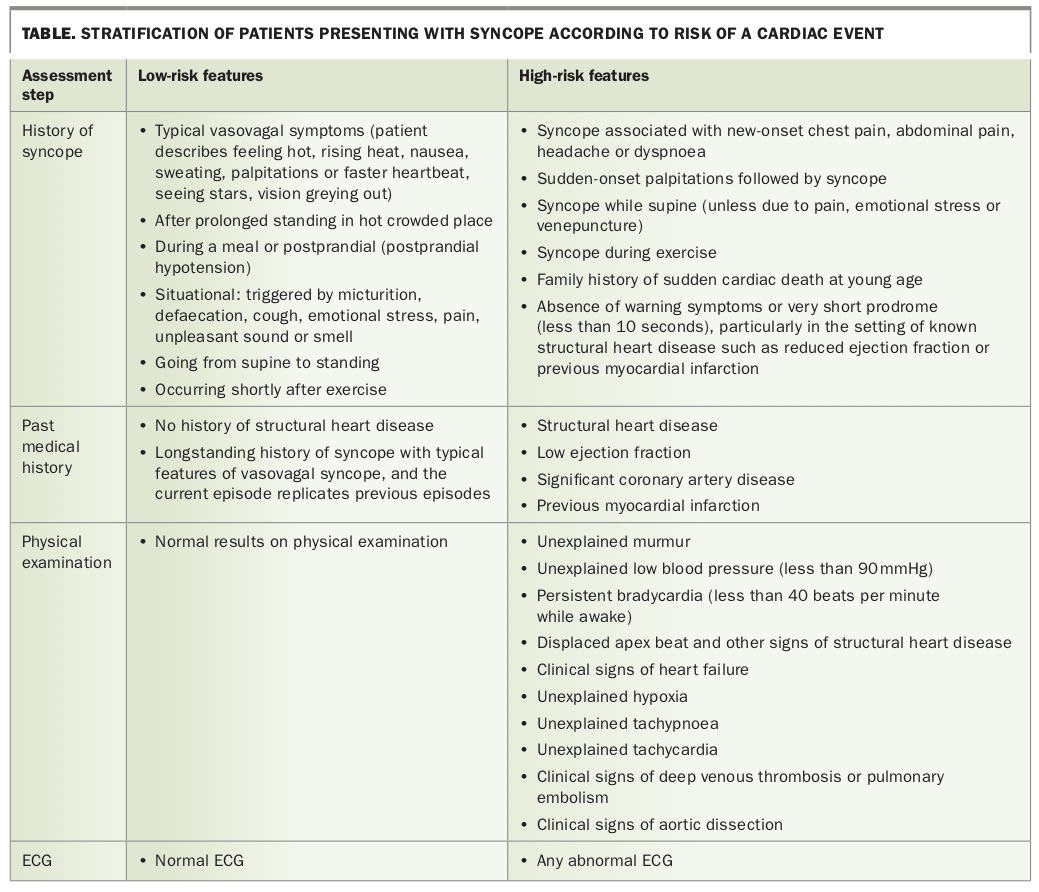
The most time-pressing goal in assessing any patient with syncope is to determine whether they are at high risk of a cardiac event. All patients should be classified as either low risk or high risk of a cardiac event, based on the history of syncope, past medical history, results of physical examination and the ECG (Table).
{kind=link}
Investigating patients with syncope
Patients at high risk of a cardiac event often require admission to hospital or a very rapid cardiology outpatient review. The choice of investigations is then driven by the clinical findings.
Patients at low risk of a cardiac event can be managed in the ambulatory care setting. In general, most patients with a diagnosis of typical vasovagal syncope do not require specific investigations. Routine blood tests, iron studies and thyroid function tests may be performed on a case-by-case basis. Routine 24-hour Holter monitoring and echocardiography are not required.
Investigating noncardiac syncope
Bedside standing test (active standing)
The bedside (active) standing test is useful because it is cheap and can be performed in almost any clinical setting. The duration of the test is variable. A minimum of five minutes is recommended, but longer testing for up to 20 minutes may provide additional useful data in selected patients. Regular monitoring of blood pressure, heart rate and symptoms is required.
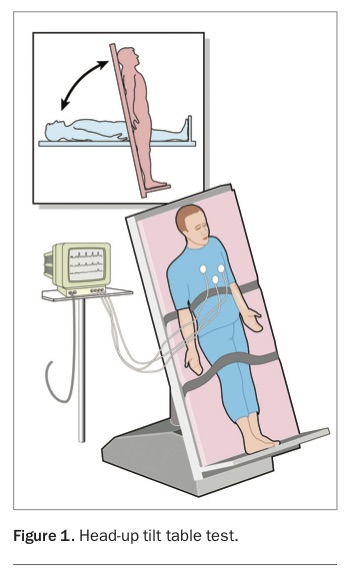
Head-up tilt table test
Use of a head-up tilt table test (HUT) to investigate the causes of syncope was first reported in 1986.3 Protocols vary, but a HUT essentially involves simultaneous monitoring of blood pressure (with an arm sphygmomanometer) and cardiac rhythm while the patient is being maintained for a prolonged period (typically more than 30 minutes) in a semi-upright position (70° angle from horizontal), as shown in Figure 1.
{kind=link}
This position differs from active standing as it minimises the activation of anti-gravity muscles, and hence the test is termed ‘passive HUT’. It results in less venous pump activation in the legs and reduced venous return to the heart, leading to progressive pooling of blood in the veins of the pelvis and lower limbs. This is compensated for by activation of the sympathetic nervous system, increasing heart rate and vasoconstriction. A HUT may also incorporate a pharmacological challenge (sublingual glyceryl trinitrate or intravenous isoprenaline) to increase the probability of triggering vasovagal syncope.
A HUT can be useful for the following:
- If a HUT triggers a vasovagal event that replicates the patient’s usual symptoms then it can help support a clinical diagnosis of vasovagal syncope. A negative result does not rule out vasovagal syncope. A positive result (a vasovagal event) is not a diagnosis unless the patient’s previous symptoms are replicated.
- A HUT may demonstrate asystole during vasovagal syncope, which is a criterion for cardiac pacing in selected patients (see below).
- A HUT can assess for orthostatic hypotension. Some patients develop slow progressive postural hypotension that is not apparent at the bedside.
- A HUT can assess for postural tachycardia syndrome (POTS), which manifests as a rise in heart rate of more than 30 beats per minute (bpm) during standing or a heart rate of more than 120 bpm that is sustained in the absence of hypotension. Although POTS is usually apparent on a bedside standing test, some patients have a more delayed response that is not elicited during the time of a typical clinical encounter.
Carotid sinus massage
Carotid sinus massage (CSM) is used to diagnose carotid sinus syndrome, where stimulus to the carotid sinus induces spontaneous asystole. CSM should not be performed in patients with carotid bruits or known significant carotid vascular disease. The rate of stroke or transient ischaemic attack during CSM is estimated at 0.24%. The consensus view of experts is that the diagnosis of carotid sinus syncope requires reproduction of spontaneous symptoms during CSM and a history compatible with a carotid sinus mechanism (e.g. head turning, craning, tight collars, neck pressure). CSM is best undertaken by a specialist while the patient is undergoing continuous ECG monitoring.
Investigating suspected cardiac syncope
Echocardiography and cardiac rhythm monitoring
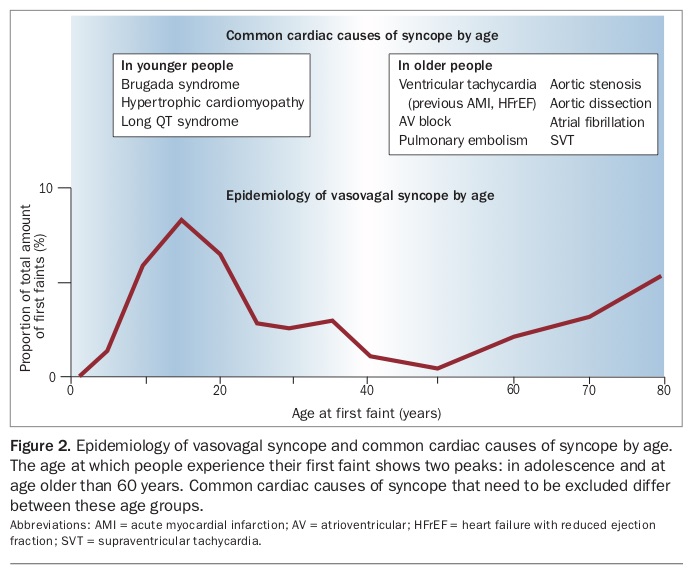
Echocardiography and cardiac rhythm monitoring are the two most important tests for almost all patients with suspected cardiac syncope. The approach to investigations needs to be targeted based on the provisional diagnosis. The cardiac differential diagnosis changes with age (Figure 2). Although vasovagal syncope is the most common cause of syncope in all age brackets, high-risk patients need to have cardiac causes of syncope excluded.
{kind=link}
Implantable loop recorder
Implantable loop recorders (ILRs) are small devices about the size of a USB stick. They can be implanted under the skin to record cardiac rhythm for longer than 12 months. These devices have automatic detect and storage functions but can also be activated via a remote-control device by the patient when symptoms occur. They are useful for obtaining symptom-rhythm correlation in patients with unexplained syncope. A significant proportion of patients with unexplained syncope have a transient arrhythmic basis for events.
Current data support the use of an ILR in patients with unexplained syncope to identify those who have indications for a pacemaker and others who may have an arrhythmic basis for their syncope. The ILR is also of value in excluding arrhythmic cardiac causes of syncope. It is important to remember that vasovagal syncope is accompanied by marked bradycardia or asystole in some patients. Identifying these features on an ILR recording does not rule out vasovagal syncope as a cause for syncope. The presence of asystole can help identify patients with vasovagal syncope who may benefit from cardiac pacing.
Case studies of patients with syncope
Case 1. A young man who collapses during a football game
A 28-year-old man who plays competitive sport for a local football club collapses during the game. He recovers spontaneously but the team coach insists he see his doctor before being allowed to play again for the club. He comes to see you and would like a certificate to continue to play.
Has this patient had syncope?
You take a detailed history from the patient about the event. He remembers running for the ball and then being face down in the mud. He believes that he tripped. He does not recall actually falling and cannot recall seeing himself go down to the ground. There were no warning symptoms beforehand such as chest pain, palpitations, light headedness or changes in vision. There was no trauma. This description suggests at least a TLOC. It is common for patients to ‘construct’ events to fill in gaps in memory – the patient thinks he must have tripped, trying to explain the event. There are no obvious symptoms to suggest a seizure, and other causes such as psychogenic or ischaemic neurological events appear much less likely. I would therefore say this patient has had a TLOC that is likely syncope until proven otherwise.
What is your approach to risk stratification for this patient?
Ascertaining the nature and circumstances of the event is a crucial first step for risk stratification. Syncope occurred while the patient was running for the ball, which means syncope during exercise. This is a high-risk situation that is more likely to have a malignant cardiac cause. It is common to experience presyncope or syncope immediately or shortly after cessation of vigorous exercise, usually because of a combination of volume depletion and vasodilation leading to hypotension. Exercise-induced fainting (vasovagal syncope) is also common, but similarly occurs after, rather than during, exercise. The abrupt onset of syncope without warning in a young person also suggests a cardiac aetiology. In this case it is important to ask about first-degree relatives with a history of sudden death at a young age.
What examination findings would you look for?
A comprehensive physical examination is always important. In a young patient with possible cardiac syncope, it may yield cardiac findings, such as a murmur, third heart sound or displaced apex beat. Postural blood pressures should also be measured.
Should this patient have an ECG?
A 12-lead ECG is a key investigation and should be performed as soon as possible in this patient. Findings to look out for in a young person include features of left ventricular hypertrophy, T wave changes that may suggest cardiomyopathy and conduction abnormalities. The QT interval should also be carefully measured; the computer interpretation should not be relied on as it is frequently incorrect.
What further investigations are needed?
Echocardiography is required in this scenario. It will allow you to exclude key diagnoses such as hypertrophic cardiomyopathy, a common cause of sudden death and syncope in the young. If echocardiography and ECG results are normal then more complex investigations could be considered, including cardiac MRI to look for conditions such as arrhythmogenic right ventricular cardiomyopathy, electrophysiological studies to assess for possible ventricular tachycardia and cardiac rhythm monitoring with an ILR to help detect occult arrhythmias. This patient should be referred to a cardiologist.
Case 2. A woman with a history of AMI who collapses at home
A 63-year-old woman with hypertension and dyslipidaemia, who experienced an acute myocardial infarction (AMI) and had a stent inserted seven years ago, has an unwitnessed collapse at home. She says she blacked out and has no recollection of what happened except that she felt slightly woozy beforehand. She found herself on the floor in the corridor of her home. She attends your clinic the same day.
Is this situation high or low risk?
This is a high-risk situation, with possible cardiac syncope as a cause of TLOC. In the setting of previous AMI, the key cardiac diagnosis to consider is a malignant arrhythmia such as ventricular tachycardia. Myocardial infarction results in scar tissue, which is a common nidus for ventricular arrhythmias, even years after the infarction.
Routine laboratory test results and examination findings are unremarkable. An ECG shows left bundle branch block and sinus rhythm at 78 bpm. An ECG four years ago showed sinus rhythm with normal QRS morphology. The patient has no chest pain and looks well.
What would you do now?
This is a high-risk scenario, as the patient has an abnormal ECG and a clear cardiac history. As the syncopal event occurred very recently, she should be admitted to hospital for cardiac monitoring and work-up. Although the diagnostic yield from cardiac monitoring is generally low, it is maximal immediately following syncope and is higher in patients with a high pre-test probability of an arrhythmic aetiology. The left bundle branch block is unlikely to be due to acute ischaemia in a patient who has no chest pain and looks well. However, progressive conduction system disease (left bundle branch block) in the setting of syncope is correlated with a higher likelihood of a bradyarrhythmic cause. About 40% of these patients may need a pacemaker.4
Case 3. An older man with a long history of collapses
A 68-year-old man with a 20-year history of collapses comes for routine review. He recently collapsed while leaning over to work on a computer. He had little warning, felt slightly light headed and collapsed bruising his ribs. He recovered rapidly and has no other associated symptoms. He reports seeing a cardiologist and other doctors 15 to 20 years ago, when he underwent tests and was told he probably just faints. He was prescribed beta blockers but is unsure if they made much difference. The fainting episodes are infrequent, sometimes with two to three years between episodes. He is obese but has no major medical problems. He has never had syncope driving a car or while seated.
Is this scenario low or high risk from a cardiac perspective?
The longstanding history of similar events implies that this is more likely to be low risk. However, the abrupt nature of the syncope with little warning puts this scenario in a high-risk category. Further investigations are therefore required. The longstanding history makes the diagnosis of vasovagal syncope more likely; patients can sometimes have an atypical presentation with few warning signs before loss of consciousness.
Twenty-four-hour Holter monitoring, a 12-lead ECG, routine blood tests, echocardiography and clinical examination all have normal results. The yield from 24-hour Holter monitoring in this scenario is very low, perhaps 1 to 2%. The crucial step is to obtain symptom (syncope) to rhythm correlation.
You refer the patient to a cardiologist who performs a HUT, which is reported as a ‘negative study’.
How else can we assess for rhythm correlated with symptoms?
In situations such as this, when syncope is recurrent and high risk, with no cause established, then long-term monitoring of cardiac rhythm with an ILR can be valuable.
The patient had an ILR implanted and within months it was clear that he had periods of high-grade atrioventricular block and asystole. A pacemaker was implanted with complete resolution of syncope.
Case 4. A fit young woman with recurrent faints
A 23-year-old woman who works as a receptionist comes to your clinic having had four ‘faints’ this year. The first episode occurred when she stood up to go to the toilet after sitting for about two hours. She felt light headed and started to see spots. She tried to get to the kitchen area to sit down but felt suddenly hot and collapsed. Another episode occurred while she was standing on a tram and felt very similar.
Her blood pressure when supine is 100/60mmHg and her heart rate is 55 bpm. She has no significant past medical history and is fit, running five days a week, training for her first marathon. She describes herself as health obsessed and ensures that all her food is natural and home cooked. Blood tests show she has borderline low iron and normal haemoglobin levels. A 12-lead ECG is normal. She has no family history of sudden death.
Is this high risk or low risk and are you convinced this is syncope?
The history is strongly compatible with vasovagal syncope. Symptoms are related to standing, and the description of the syncope itself is consistent with a typical vasovagal syncope ‘story’. In this case, the history is enough to make the diagnosis and in general further investigations are not required.
Do the history and results suggest any potential exacerbating factors or triggers for the vasovagal events?
The patient’s blood pressure is a little low, although this could be normal for a young woman who is slim and fit. As she is fitness training, adequate fluid and electrolyte replacement are important, and a detailed review of her diet and weight history is essential. Intense exercise can result in lower sustained blood pressure, which may predispose to vasovagal syncope. Weight loss also lowers blood pressure. Her diet, particularly if it is low carbohydrate, will require a high fluid intake to compensate. Salt intake may also be low. Some people who actively avoid salt may in fact develop low blood pressure and syncope. The patient mentions that she usually does not eat breakfast, often having only a cup of coffee in the morning but does try to drink water during her runs.
What would you recommend now?
I would institute an aggressive increase in water intake for this patient, aiming for at least three litres daily, with additional fluids before sport. It is reasonable to also increase salt intake. The patient can be reassured that the tendency to recurrent vasovagal syncope can be resolved with simple nonpharmacological measures in many people (estimated about 70%). However, there are no formal trials of the effects of education and lifestyle modification.
What can you do if the patient continues to faint despite increasing fluid and salt?
There are some further nonpharmacological measures that may be helpful for patients with recurrent vasovagal syncope. Firm thigh-high lower-limb graded compression stockings may assist with venous return and reduce the tendency to vasovagal syncope. In addition, a randomised controlled trial found that physical counterpressure manoeuvres such as leg crossing, handgrip or arm tensing were effective in reducing the burden of syncope, with a relative risk reduction of 39%.5 Isometric exercise increases cardiac output and blood pressure. Patients with a clear prodrome (warning symptoms) may benefit from learning to recognise the warning signs and to perform physical counterpressure manoeuvres to help abort syncope. However, physical counterpressure manoeuvres are ineffective for patients with a very short prodrome and are less effective in those aged over 60 years.
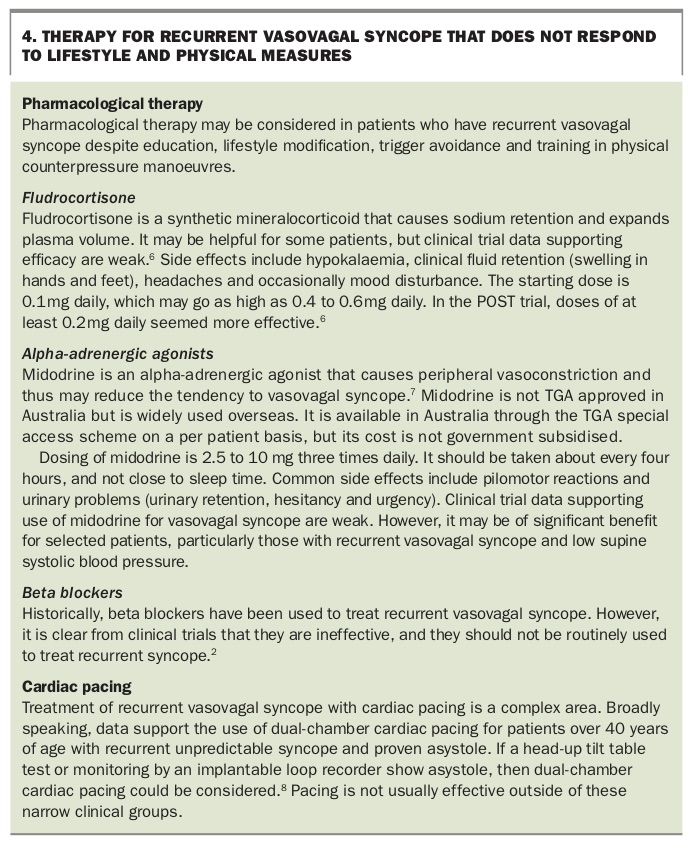
If patients continue to experience recurrent vasovagal syncope despite education, lifestyle modification, trigger avoidance and training in physical counterpressure manoeuvres then pharmacological therapy or cardiac pacing may be considered (Box 4).6-8
{kind=link}
Case 5. A young woman with sudden-onset exercise intolerance and presyncope
A 33-year-old woman presents with fatigue, exercise intolerance and frequent presyncope, especially when she stands for a while. She struggles in queues or on public transport. This began about four weeks ago and has progressively worsened. She is usually well but is now also experiencing intermittent chest pains. She has noticed that her fitness tracker frequently shows a high heart rate. Results of blood tests, a 12-lead ECG and echocardiography are normal. Her blood pressure measured in your office is 110/70 mmHg supine. She has no family history of sudden death.
Is this a low-risk or high-risk cardiac scenario?
The normal echocardiogram and ECG and the postural nature of the patient’s symptoms suggest some form of orthostatic intolerance. She falls into a low cardiac-risk category.
What is a useful test you could do in the clinic?
A simple bedside standing test would be helpful. The patient’s blood pressure and heart rate are documented while she is lying down and then monitored for at least 10 minutes after she stands up. To save time, you can usually do this monitoring while you take a more detailed history. In this patient’s case, she feels unsettled after seven minutes of standing and would like to sit down. Her blood pressure is 115/70 mmHg and heart rate is 110 bpm, whereas her supine heart rate was 65 bpm. This pattern suggests a diagnosis of POTS.
What is POTS?
POTS is a challenging syndrome that may overlap with chronic fatigue syndrome. It is characterised by orthostatic intolerance with an excess sustained high heart rate when standing, in the absence of hypotension.9 Patients describe feeling light headed and having brain fog, anxiety, chest discomfort, palpitations, irritable bowel-like symptoms and exercise intolerance. Those affected are predominantly women, and about 50% of cases appear to follow a viral illness. A proportion improve progressively without intervention, whereas others have a chronic illness that may wax and wane.
There are no good clinical trials that help guide investigations and treatment. Finding a specialist with an interest in the area is worthwhile. Monitoring, supporting and treating psychological and psychiatric conditions are essential. An exercise physiology program can also be of value if delivered by someone with experience in this area.
Case 6. An older man with Parkinson’s disease and repeated falls
A 78-year-old man with Parkinson’s disease and longstanding type 2 diabetes presents for assessment of falls. He is noted to have a supine blood pressure of 170/80 mmHg that falls to 110/60 mmHg when he stands.
What is the provisional diagnosis?
This patient has severe postural hypotension. Parkinson’s disease may be complicated by autonomic failure, which can result in supine hypertension and postural hypotension. Longstanding diabetes can also cause autonomic failure. Medications such as levodopa used to treat Parkinson’s disease can exacerbate postural hypotension.
How can he be treated?
The recommended treatment approach for patients with autonomic failure involves:
- increasing fluid intake
- using lower limb compression stockings to increase blood pressure when the patient stands
- sleeping with the head of bed elevated at 10°; this reduces supine hypertension, which results in increased nocturia and thus dehydration overnight, exacerbating postural hypotension in the morning
- considering treatment with pressor agents such as fludrocortisone and midodrine, which may be helpful
- considering treatment of supine hypertension with short-acting antihypertensive medications such as captopril and hydralazine overnight.
Conclusion
Syncope represents a disparate group of diagnoses. It is crucial that every effort is made to identify patients with syncope who are at high risk of a cardiac event, so that they can receive timely targeted treatment to reduce the risk of sudden death. Most cases of syncope are benign, usually due to vasovagal syncope, but a small subset of patients may experience recurrent syncope which can be challenging to manage. Specialist referral is of value to these patients. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.