Heart failure with reduced ejection fraction. Advances in management


Dr Wang is an Advanced Trainee at Cardiology Department, Royal Prince Alfred Hospital, Sydney.
Associate Professor Lattimore is Director of Chronic Heart Failure Services at Cardiology Department, Royal Prince Alfred Hospital, Sydney, NSW.
Heart failure
Heart diseases
Heart failure (HF) is a leading cause of morbidity and a major burden on healthcare resources. Targeting modifiable risk factors and use of guideline-directed medical therapies in at-risk individuals is a crucial first step in the prevention of HF progression. All eligible patients with HF and reduced ejection fraction should be treated with the ‘big four’ pharmacological therapies to reduce cardiovascular mortality and HF hospitalisation.
- Prevention of heart failure (HF) progression is a crucial first step in the management of HF. Aggressive risk factor management (particularly blood pressure control) and use of proven therapies, such as angiotensin converting enzyme inhibitors, beta blockers, sodium-glucose cotransporter-2 (SGLT-2) inhibitors, and novel agents, such as finerenone, are needed in at-risk populations.
- The SGLT-2 inhibitors dapagliflozin and empagliflozin are recommended first-line drugs for patients with HF with reduced ejection fraction (left ventricular ejection fraction <40%) to reduce the risk of HF hospitalisation and death.
- All eligible patients with HF with reduced ejection fraction should be treated with the ‘big four’ pharmacological drug classes – angiotensin receptor neprilysin inhibitors, beta blockers, mineralocorticoid receptor antagonists and SGLT-2 inhibitors – which have proven benefit in reducing cardiovascular mortality and HF hospitalisation. These drugs are also effective for patients with HF and left ventricular ejection fraction of 40 to 49%, although the evidence is less robust.
- Percutaneous edge-to-edge mitral valve repair should be considered in carefully selected patients with secondary mitral regurgitation who are not eligible for surgery and are symptomatic despite optimal medical therapy.
Heart failure (HF) is a clinical syndrome consisting of cardinal symptoms (e.g. breathlessness, fatigue and ankle swelling) and signs (e.g. elevated jugular venous pressure, pulmonary crackles and peripheral oedema) caused by a structural and/or functional abnormality of the heart.1 This results in elevated intracardiac pressures and/or inadequate cardiac output at rest or during exercise.
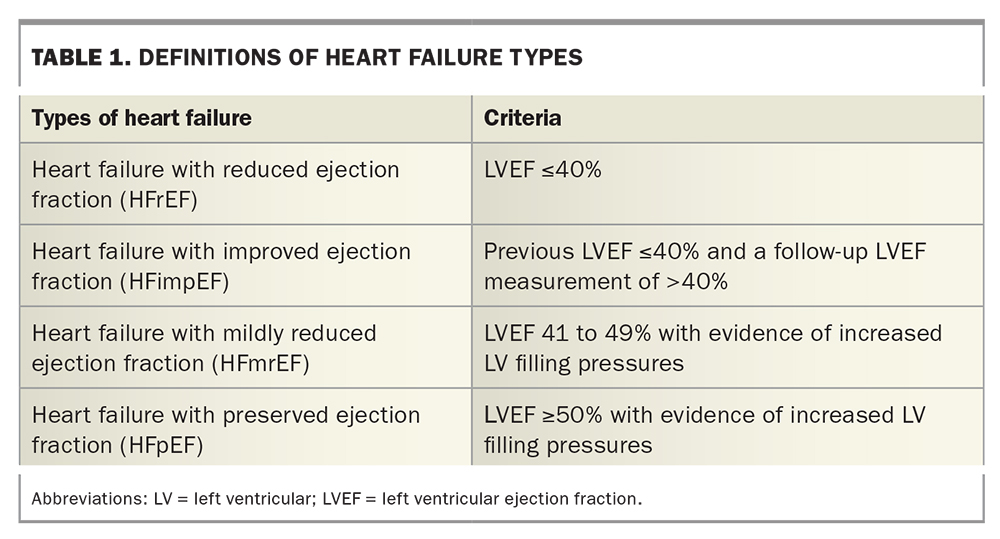
The 2018 National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand guidelines defined heart failure with reduced ejection fraction (HFrEF) as a diagnosis of HF and a left ventricular ejection fraction (LVEF) of less than 50%.2 However, the most recent consensus statement on the management of HF published in the Medical Journal of Australia defines HFrEF as HF and an LVEF of less than 40% (i.e. a significant reduction in left ventricular systolic function) (Table 1).3 Patients with an LVEF between 41% and 49% have mildly reduced left ventricular systolic function (HFmrEF). Making this distinction is important because patients with HFmrEF appear to have a slightly different response to current and potentially novel treatments compared with patients with HFrEF and those with HF with preserved ejection fraction (HFpEF). In particular, all guideline-directed medical therapies for HFrEF appear to provide similar but somewhat attenuated benefits in patients with HFmrEF.1,3,4 HFpEF is defined as HF and an LVEF of 50% or more (Table 1).3
{kind=link}
Patients who previously had an LVEF of 40% or below and then a follow-up LVEF measurement above 40% are termed as having HF with improved ejection fraction (HFimpEF). These patients should continue guideline-directed medical therapy for HFrEF because withdrawal of pharmacological treatment can lead to a decrease in LVEF and worsening HF.5
Heart failure workup
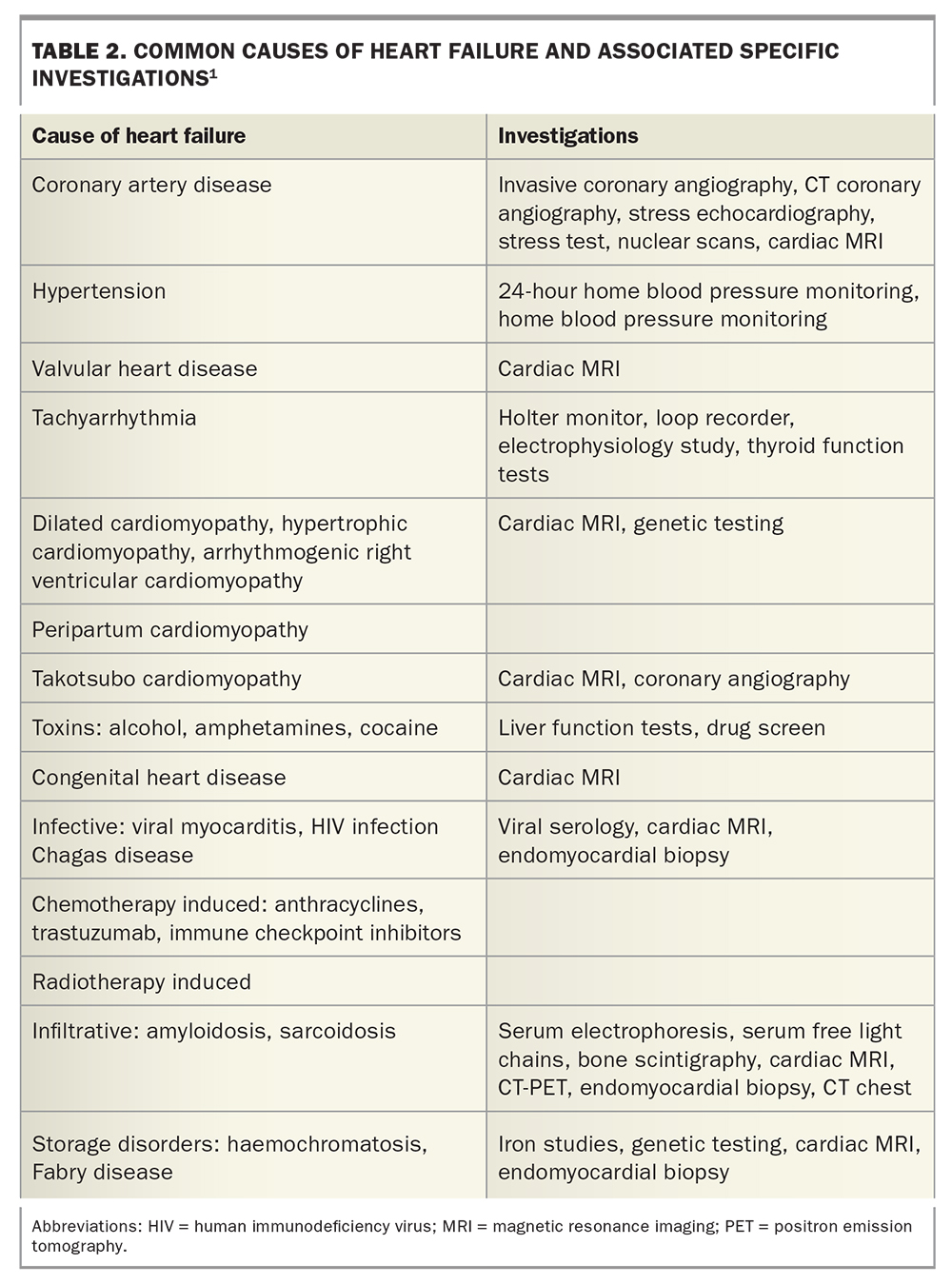
Workup for HF requires careful assessment to delineate the underlying aetiology of the cardiac dysfunction, as each pathology determines specific treatments and prognosis. Common causes of HF include ischaemic heart disease, hypertension, valvular heart disease, familial or genetic cardiomyopathies, amyloidosis, cardiotoxic-related causes including chemotherapies, alcohol, cocaine and methamphetamine use, tachycardia-induced cardiomyopathy, right ventricular pacing or stress-induced cardiomyopathy (Table 2).
{kind=link}
Treatment of HF usually begins with addressing the underlying aetiology. For example, for patients with tachycardia-induced cardiomyopathy, addressing the underlying tachycardia can usually lead to improved cardiac function. Disease-specific therapies are available for certain conditions, such as tafamidis for transthyretin cardiac amyloidosis, immunosuppressants for cardiac sarcoidosis and, more recently, mavacamten (a cardiac myosin inhibitor) for hypertrophic obstructive cardiomyopathy.6-8
Preventing heart failure progression
HF is one of the leading causes of morbidity and a major burden on healthcare resources both in Australia and globally.9 This burden is expected to increase with an ageing population and ongoing improvements in mortality across the spectrum of cardiac diseases. Major advances in prevention (both primordial and primary prevention) and early detection of HF are needed to help prevent the development and progression of clinically significant HF.
The American College of Cardiology/American Heart Association guidelines define patients according to a spectrum, ranging from those at risk of developing HF (stage A), those who have preclinical cardiac dysfunction (stage B) and those with symptomatic/advanced HF (stages C/D).4 Patients with stage A HF are asymptomatic, without evidence of structural heart disease or abnormal cardiac biomarkers, but have risk factors for the development of HF, such as hypertension, coronary artery disease, diabetes, metabolic syndrome, exposure to cardiotoxins or a positive family history or genetics for cardiomyopathy. Patients with stage B HF are asymptomatic with evidence of either structural or functional heart disease. Both stages A and B HF patients are important groups to target for prevention of clinically significant HF.
Elevated systolic and diastolic blood pressure are major risk factors for the development of symptomatic HF and many randomised clinical trials have shown that adequate blood pressure control reduces the risk of HF. For example, a meta-analysis showed that blood pressure control was associated with a 40% reduction in HF events.10 Therefore, all patients with hypertension should receive appropriate treatment in accordance with published blood pressure guidelines.
Healthy dietary habits and regular physical activity are also important strategies for the prevention of HF because they help maintain normal blood pressure, regulate blood glucose levels and prevent obesity.11-14 The Mediterranean diet, whole grain and plant-based diets and the Dietary Approaches to Stop Hypertension (DASH) diet are particularly effective and can offer some protection against the development of HF.15-17
Aside from targeting modifiable risk factors, there is evidence that some of the guideline-directed medical therapies can prevent the development of clinically significant HF in at-risk individuals. Both angiotensin converting enzyme (ACE) inhibitors and beta blockers have been shown to prevent the development of HF in patients with left ventricular (LV) dysfunction, particularly after a myocardial infarction.18-21
Patients with type 2 diabetes or those with established cardiovascular disease or at high risk of cardiovascular disease should receive sodium-glucose cotransporter-2 (SGLT-2) inhibitors, which have been proven to prevent HF hospitalisations. Most patients enrolled in these trials did not have HF at baseline, and so the SGLT-2 inhibitors are an effective option for the primary prevention of symptomatic HF.22,23 In a clinical trial of patients with diabetic chronic kidney disease, finerenone, a nonsteroidal mineralocorticoid receptor antagonist (MRA), was associated with a significant reduction in HF hospitalisation and new-onset HF.24 Finerenone may become an important treatment option to prevent HF in patients with diabetic chronic kidney disease.
Early referral of the patient to a cardiologist is also an important strategy in the prevention of LV dysfunction. In one single centre study, patients at risk of HF (identified by the presence of hypertension, diabetes or known vascular disease with elevated brain-type natriuretic peptide levels), but without established LV systolic dysfunction or symptomatic HF at baseline, underwent echocardiography and were referred to a cardiologist. These patients had lower rates of newly diagnosed HF and asymptomatic LV dysfunction compared with those who continued with usual care.25
Pharmacological management of HFrEF
The pharmacological management of HFrEF is centred around the use of guideline-directed medical therapies that have proven efficacy in improving survival and reducing the risk of HF hospitalisation and symptoms of HF.3 Four major drug classes (known as ‘the big four’) should be used in as many patients with HFrEF as possible:
- angiotensin receptor neprilysin (ARN) inhibitors or ACE inhibitors
- beta blockers
- MRAs
- SGLT-2 inhibitors.
A combination of these four therapies can reduce the risk of all-cause death by over 60%, the risk of cardiovascular death or HF hospitalisation by 64% and cardiovascular death by 67% compared with placebo in patients with HFrEF.26 These four drugs should be initiated as soon as possible, ideally during the index HF hospitalisation, and should be aggressively uptitrated to the maximally tolerated doses.3
Previous HF guidelines recommended the step-wise up-titration of guideline-directed medical therapies, but this approach might delay starting these highly effective therapies.2 In particular, the HF therapies have proven efficacy regardless of the background treatment, which suggests the drugs should be used in combination.27,28 Furthermore, the benefits of ARN and SGLT-2 inhibitors are seen early after initiation, making a strong case for starting these treatments upfront before full titration of the individual medications, which may include starting more than one drug simultaneously.29,30 The recent Australian and New Zealand HF consensus document recommends the preferential use of SGLT-2 inhibitors and ARN inhibitors in patients who are congested, whereas beta blockers should be reserved for those who are euvolaemic (Flowchart).3
ARN or ACE inhibitors
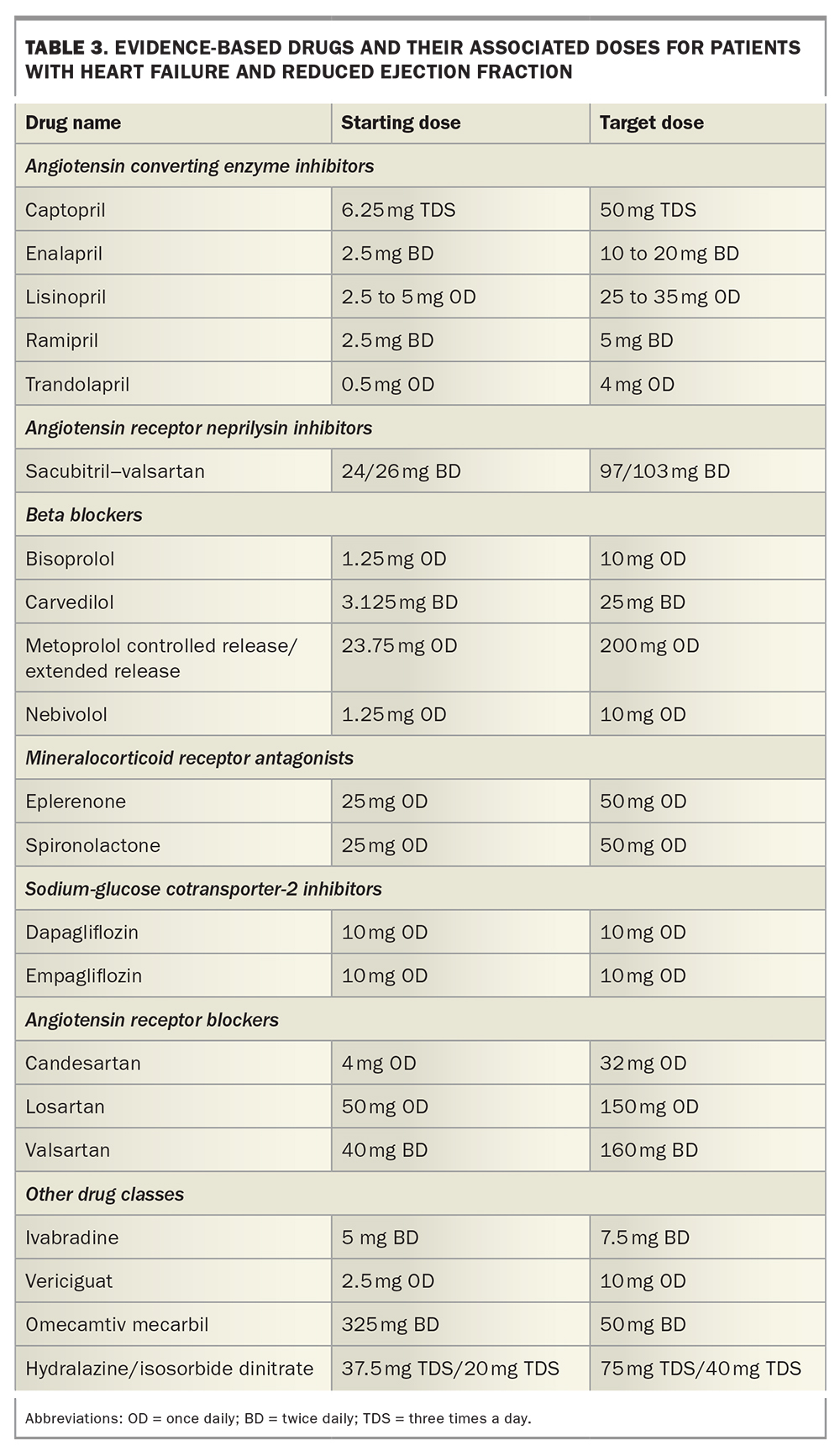
Use of ACE inhibitors reduces mortality and HF hospitalisation and improves symptoms in patients with HFrEF.31-33 They should be started at a low dose, and increased to the target dose when tolerated (Table 3).
{kind=link}
ARN inhibitors (sacubitril–valsartan) have been shown to provide additional benefit, in terms of reducing death and HF hospitalisation in patients with HFrEF, above and beyond an ACE inhibitor alone.34 Patients starting on sacubitril–valsartan should have adequate blood pressure and an estimated glomerular filtration rate (eGFR) of 30 mL/min/1.73m2 or above. If an ARN inhibitor is used in replacement of an ACE inhibitor, there needs to be at least a 36-hour washout period after the ACE inhibitor is ceased to minimise the risk of angioedema. Subsequent analyses have shown that benefits from sacubitril–valsartan are derived within 30 days of introduction, and benefits are seen when used in hospitalised patients who were not previously treated with ACE inhibitors.35-37 These studies support the earlier introduction of ARN inhibitors in the treatment pathway of HFrEF, such that ARN inhibitors should ideally be used as the first-line agent (Flowchart).3 Patients should be started at a low dose, with the aim to increase the dose to the maximally tolerated dose. Patients who are initiated on an ARN inhibitor need to have their renal function and electrolyte levels monitored about one to two weeks after initiation or dose titration. Angiotensin receptor blockers may be used as an alternative to ACE inhibitors in the setting of intolerable cough, or as alternatives to ACE inhibitors and ARN inhibitors in patients with a history of angioedema.2,38
Beta blockers
Beta blockers have been shown to reduce mortality and morbidity in patients with HFrEF, with benefits seen in addition to background ACE inhibitor use.39-41 A beta blocker should only be initiated in patients with HF who are clinically stable and euvolaemic.2,3 Beta blockers should be used with caution in any patient with acute decompensation of HFrEF in case of precipitating a risk of further deterioration given its negative inotropic effects. Patients with severe asthma should be monitored carefully when given beta blockers and under close supervision by a respiratory specialist. Chronic obstructive pulmonary disease should not be a reason against using beta blockers.42 Only one of the four beta blockers with proven benefit in HF should be used. Clinicians should prescribe beta blockers at a low dose and uptitrate to target doses as tolerated (Table 3).
Mineralocorticoid receptor antagonists
Use of MRAs have shown to consistently improve all-cause mortality, HF hospitalisations and symptoms across a wide range of patients with HFrEF.43,44 An eGFR of 30 mL/min/1.73 m2 or less or the presence of hyperkalaemia are contraindications to MRA initiation. Electrolytes, in particular potassium levels, should be carefully monitored in all patients who are started on an MRA. Use of SGLT-2 inhibitors reduces the risk of hyperkalaemia, which may facilitate the use of MRAs in patients with HF. This approach reinforces the need to use these two drug classes in combination, often initiated at the same visit, rather than uptitration of a single drug class at a time.45 If available, eplerenone should be used over spironolactone because of the higher selectivity of eplerenone for the aldosterone receptor, which results in lower rates of adverse effects such as gynecomastia and vaginal bleeding in women.44 Eplerenone is not currently available for GP prescribing under the PBS.
Sodium-glucose cotransporter-2 inhibitors
The two major trials of SGLT-2 inhibitors in patients with HFrEF show that dapagliflozin and empagliflozin are associated with significant reductions in the composite endpoint of cardiovascular death and HF hospitalisation compared with placebo.46,47 The drugs were well tolerated, with a favourable adverse event profile, and the benefits were independent of background therapy and similar in patients with and without diabetes.27,46,47 The benefits of SGLT-2 inhibitors are seen within 30 days of starting therapy.28,48 Although SGLT-2 inhibitors are generally well tolerated, they have not been evaluated in patients with severe renal impairment (eGFR <25 mL/min/1.73 m2). Either dapagliflozin 10 mg once daily or empagliflozin 10 mg once daily can be used and, unlike the other guideline-directed HF therapies, no dose titration is needed. SGLT-2 inhibitors should no longer be seen as only diabetes drugs, but also as first-line therapies for HFrEF.
Other pharmacological therapies
Ivabradine is an inhibitor of the If channel in the sinus node, and therefore lowers resting heart rates in patients with sinus rhythm. Use of ivabradine has been shown to reduce the composite endpoint of cardiovascular mortality and HF hospitalisation in patients who had symptomatic HF and an LVEF of 35% or less, were in sinus rhythm with a resting heart rate of 70 beats/min or more and had been admitted to hospital recently for HF.49,50 Only patients with a resting heart rate of 77 beats/min or more had a reduction in mortality. Patients should have their beta blocker dose uptitrated to the maximum tolerated dose before use of ivabradine.
Vericiguat, a soluble guanylate cyclase stimulator, activates the cyclic guanosine monophosphate (cGMP) pathway by directly stimulating soluble guanylate cyclase through a binding site independent of nitric oxide. It also sensitises soluble guanylate cyclase to endogenous nitric oxide by stabilising nitric oxide binding to the binding site.51 Vericiguat showed a modest (about 10%) reduction in cardiovascular death and HF hospitalisation compared with placebo in a randomised trial of patients with HFrEF with evidence of worsening HF.52 It is possible that select groups of patients with progressive HF, but not very advanced HF, will benefit from use of vericiguat. Vericiguat is listed on the PBS from 1st December 2022.
The selective cardiac myosin activator omecamtiv mecarbil (not currently available in Australia) was shown in a placebo-controlled, randomised trial to decrease cardiovascular death and HF hospitalisation in patients with HFrEF.53 It appears that patients with the lowest LVEF derive the most benefit from use of omecamtiv mecarbil.54 This drug may become an important therapeutic option in patients with very low LVEF.
Diuretics, both loop diuretics, such as frusemide, and thiazide (or thiazide-like) diuretics, such as hydrochlorothiazide, have no role in improving the prognosis of patients with HFrEF. Diuretics are used for symptom relief to aid in decongestion only. Maintenance doses of diuretics are often needed to help keep patients euvolaemic, although the dose may need to be reduced to allow adequate blood pressure for use of guideline-directed medical therapies.
Nonpharmacological therapies for HFrEF
Nonpharmacological management of patients with HF should begin with lifestyle changes. In particular, patients with HF should limit their dietary salt intake to less than 5 g per day.1,4 Fluid restriction is also often advised, with limits of about 1.5 to 2.0 L per day a reasonable starting point. Fluid allowances should be adapted to the patient’s weight and according to climate and presence of diarrhoea or vomiting. Excessive alcohol intake should be avoided and completely abstained in patients with alcoholic cardiomyopathy.1,4
Regular exercise should be encouraged, and exercise regimens should be tailored to the patient’s physical and functional limitations. An individual patient meta-analysis of 13 trials of 3990 participants (97% with HFrEF) showed that exercise-based cardiac rehabilitation was associated with significant improvements in quality of life and exercise capacity.55
All patients with HF should receive annual influenza vaccines and be up to date with pneumococcal vaccines as they appear to be associated with lower rates of HF hospitalisation and death.56
Intravenous iron
Intravenous iron should be given to patients with HFrEF who have iron deficiency to improve HF symptoms and quality of life.57 Patients with serum ferritin level of less than 100 mcg/L or ferritin level of 100 to 299 mcg/L with transferrin saturation below 20% should receive intravenous iron.3,57
Cardiac resynchronisation therapy
Cardiac resynchronisation therapy (CRT) remains an important treatment strategy for symptomatic patients with HFrEF who have evidence of cardiac dyssynchrony, as determined by the width of the QRS complex on electrocardiograms. The strongest indication for CRT is in patients in sinus rhythm with a QRS duration of 150 ms or more, a left bundle branch morphology, and an LVEF of 35% or less despite optimal medical therapy. In these patients, CRT has been shown to improve morbidity and mortality.58-61 CRT should also be used in patients with HFrEF who require ventricular pacing (e.g. a pacemaker for high-degree atrioventricular block). This is because right ventricular pacing leads to dyssynchrony (equivalent to a left bundle branch block) and worsening of HF symptoms.62,63 Patients with symptomatic HF, an LVEF of 35% or less, in sinus rhythm and QRS durations of 130 to 149 ms or non-left bundle branch morphologies with QRS of 150 ms or more also derive benefits from CRT.64,65
Implantable cardioverter defibrillators
Implantable cardioverter defibrillators (ICDs) are used to treat potentially life-threatening ventricular arrhythmias, a known complication and major cause of mortality in patients with HFrEF. ICDs should be used in all patients for secondary prevention purposes in which a patient has survived a severe ventricular arrhythmia that does not have a reversible cause (such as within 48 hours of a myocardial infarction). The patient needs to have a reasonable life expectancy of more than a year and good functional status.
The use of primary prevention ICDs in HFrEF remains a topic of debate. The strongest indication for an ICD is in patients with symptomatic HF (New York Heart Association class II-III) with ischaemic cardiomyopathy and an LVEF of 35% or less despite three months or more of optimal medical therapy, provided the patient has one year or more life expectancy and good functional status.66,67 Patients with non-ischaemic cardiomyopathy may also derive benefit from ICDs, although the evidence for this is less strong than those with ischaemic cardiomyopathy.66,68,69
Subcutaneous ICDs are an alternative to transvenous ICDs, and are preferred in patients with difficult venous access or those at risk of lead infections. However, subcutaneous ICDs are unable to provide pacing therapy for bradyarrhythmia or anti-tachycardia pacing, and so careful patient selection is needed.70-72 Given the advances in medical therapy for HF in recent years, it is now unclear whether the benefits of ICDs in primary prevention are applicable with the modern era of optimal medical therapy that includes ACE/ARN inhibitors, beta blockers, MRAs and SGLT-2 inhibitors.
Transcatheter edge-to-edge repair
Patients with moderate or severe mitral regurgitation have an extremely poor prognosis in the setting of HF.73,74 Secondary mitral regurgitation is mitral regurgitation that occurs as a consequence of disease in the left ventricle or left atrium rather than disease of the mitral valve apparatus (leaflets or chords). In patients with persistent symptoms and moderate-severe or severe mitral regurgitation despite optimal medical therapy, mitral valve surgery (ideally repair over replacement) is recommended. However, many patients with HFrEF are not suitable candidates for invasive cardiac surgery. Transcatheter edge-to-edge repair can be used in carefully selected patients with significant secondary mitral regurgitation who are symptomatic despite optimal medical therapy.75,76 The Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation (COAPT) trial showed that transcatheter edge-to-edge repair in select patients with significant secondary mitral regurgitation on optimal medical therapy was associated with a 47% reduction in HF hospitalisation, with a number needed to treat to prevent one hospitalisation for heart failure within 24 months of 3.1.77 In contrast, the Percutaneous Repair with the MitraClip Device for Severe Functional/Secondary Mitral Regurgitation (MITRA-FR) trial showed that transcatheter edge-to-edge repair was not associated with a significant reduction in death from any cause or HF hospitalisation in patients with severe secondary mitral regurgitation and HFrEF.78
The differing results between the COAPT and MITRA-FR trials are likely explained by the different patient populations enrolled in the trials. Patients in the COAPT trial tended to have more severe mitral regurgitation, with relatively less severe LV dysfunction and dilatation, whereas patients in the MITRA-FR trial tended to have less severe mitral regurgitation relative to a very dilated and weak left ventricle.79 Transcatheter edge-to-edge repair is likely a very effective treatment strategy for patients with HFrEF and secondary mitral regurgitation, but careful patient selection is needed, which requires early referral of the patient to a multidisciplinary heart team consisting of interventional, imaging and HF cardiologists and cardiothoracic surgeons.
Mechanical circulatory support devices
Finally, some patients with HF inevitably progress to advanced stages and develop persistent symptoms despite use of maximal medical therapy. In select patients with advanced HF, mechanical circulatory support has been shown to improve survival and symptoms.1,4 In Australia, short-term mechanical circulatory support devices such as LV assist devices are used as a bridge to heart transplantation. Decisions about a patient’s suitability for heart transplantation are made in a multidisciplinary team, and contributing patient factors include good compliance, appropriate capacity to care for their device and psychosocial support.
Conclusion
HFrEF remains a major cause of death and morbidity and is a major burden to healthcare worldwide. There is now an armamentarium of treatment options available for HFrEF, and the combination of the ‘big four’ pharmacological therapies – ARN inhibitors, beta blockers, MRAs and SGLT-2 inhibitors – can reduce cardiovascular mortality and HF hospitalisation by over 60%. Early use of these four drug classes should form the cornerstone of HFrEF management. Transcatheter edge-to-edge repair has emerged as a highly effective treatment option in select patients with secondary mitral regurgitation, and early referral of the patient to a multidisciplinary heart team should be considered.
Despite these improvements, the burden of HFrEF will continue to increase with an ageing population and ongoing improvements in survival with general cardiovascular diseases. There is an urgent need for a concerted effort that focuses on the prevention of HF progression in all at-risk patients to help address this global epidemic. MT