Codeine and headache. ‘Doctor, I just need a script for my headaches’

Harms associated with codeine-based treatments for headache include medication overuse headache and accidental overdose. Suggested management of patients with headache and codeine dependence includes education about harms of codeine, codeine withdrawal with bridging therapy if required, preventive medications and acute treatment for the primary headache disorder, and advice on lifestyle measures.
- Opioid use for episodic migraine is one of the greatest risks for transformation to chronic migraine.
- Lifestyle measures are integral to chronic headache management.
- Codeine is usually withdrawn gradually, with use of a bridging strategy if required.
- Starting a preventive medication is usually recommended at the same time as withdrawing codeine.
Many patients rely on over-the-counter medications to manage headache, without seeking medical advice. A study of patients presenting to their community pharmacy for headache management in Ireland found that codeine-based products were the preferred analgesic medications (43%), and 53% had never consulted their GP for headache. Thirty to fifty percent had episodic migraine and 11% had chronic daily headache in this surveyed cohort.1
With the upscheduling of codeine in Australia, more headache sufferers will present to their GPs to request a codeine prescription or alternative treatment for their primary headache disorder. This is an opportunity to educate and change their management strategies to reduce harm and increase efficacy. This article discusses the management of patients who use codeine-based medications to treat headache.
What harms are associated with codeine use for headache?
Chronic migraine affects 1 to 2% of the population, with an annual rate of transformation from episodic migraine of 2.5%.2 Opioid use for episodic migraine is one of the greatest risks for transformation to the chronic form (44% increased risk).2,3
Medication overuse headache is a significant problem in management of patients with chronic headache. The main drivers of its development are the use of opioid analgesics, triptans or ergots on more than 10 days per month. People with comorbid depression, anxiety and poor sleep are more susceptible to developing medication overuse, and these issues should always be explored and appropriately managed in patients with headache.4 About 30% of patients will have a significant reduction in headache severity and frequency if the only change in their management is cessation of codeine use.5
The harms associated with long-term codeine and opioid use extend beyond the risk of medication overuse headache and transformation to chronic migraine. They include:6
- accidental overdose and death, particularly with polypharmacy (especially with concomitant benzodiazepines)
- worsening overall pain, development of body pain and opioid-induced hyperalgesia
- immunosuppression
- depression and anxiety
- opioid-induced impairment of the hypothalamic-pituitary-adrenal axis leading to decreased sexual function, disruption of the menstrual cycle, osteoporosis, fatigue and weight gain.
Management of a patient with headache and codeine dependence
Suggested steps in managing a patient with headache and codeine dependence are summarised in Box 1.
{kind=link}
Educate the patient about the harms of codeine
After exclusion of primary headache disorders that require prompt specialist referral and red flags, the first step in managing patients with headache and codeine dependence is to reassure them that there are many more effective and better tolerated ways of managing their chronic headache that do not carry the same risks as codeine. It is important that patients do not feel persecuted or blamed for their codeine dependence. It is also important that they understand codeine is not the best long-term option and is probably making their headaches worse. A suggested patient handout on codeine and headaches is available here.
Many patients believe that codeine works, as their headache settles slightly and then flares when the dose wears off, prompting another dose to be taken. Explaining that this is not actually a sign of how well the medication is working but rather a sign of withdrawal headache is important in engaging patients with the withdrawal process.
It is also helpful to outline to patients the timeline for codeine withdrawal. Codeine withdrawal will ultimately help their headache control, but they need to get through the withdrawal period first, which can last about three weeks. During this time they may have transient worsening of headache, as well as other symptoms such as anxiety, cold sweats, diarrhoea and nausea, depending on the degree of their dependence. There are strategies to minimise these symptoms for them.
Recommend patient self-care for headache management
In all patients with frequent or chronic headache, lifestyle measures to manage headache should be reinforced. These include:
- adequate amounts of good-quality sleep, with regular sleeping hours. For patients with problems initiating sleep, a trial can be considered of melatonin 2 mg one hour before bedtime for four to six weeks to reset the sleep cycle, in conjunction with good sleep hygiene. Useful advice on sleep hygiene is available at the Better Health website (www.betterhealth.vic.gov.au/health/conditionsandtreatments/sleep-hygiene).
- regular meals, low in simple sugars and refined carbohydrates. Patients should not skip meals.
- drinking plenty of water to stay well hydrated; 1.5 to 2 litres daily is suitable for most people except those who require fluid restriction for medical reasons.
- regular exercise – walking, swimming and cycling are all good options for people with headaches. Running, aerobics and other activities that involve jumping or thumping can aggravate headache and are probably best avoided.
- limiting caffeinated drinks to a maximum of two cups daily. Patients with sleep problems should avoid caffeine after 3 pm.
- avoiding known headache triggers. Common food triggers for migraine include chocolate, strong cheeses, flavour enhancers such as monosodium glutamate (MSG), citrus, preserved meats and alcohol. Food triggers are often specific to the individual, but it is recommended that patients explore the common triggers to assess their contribution to migraines. If a clear association is found then it is sensible to avoid that food. However, in the absence of obvious food triggers, a restrictive diet is not helpful.
- good workplace ergonomics, particularly for computer users. Take regular ‘mini-breaks’ every 45 minutes to stand, stretch and rest the eyes for a few minutes.
- regular use of a relaxation technique, which can help manage stress. This might include meditation, mindfulness, yoga, progressive muscle relaxation, breathing techniques or guided relaxation using a phone app.
Support codeine withdrawal
Codeine-weaning strategies
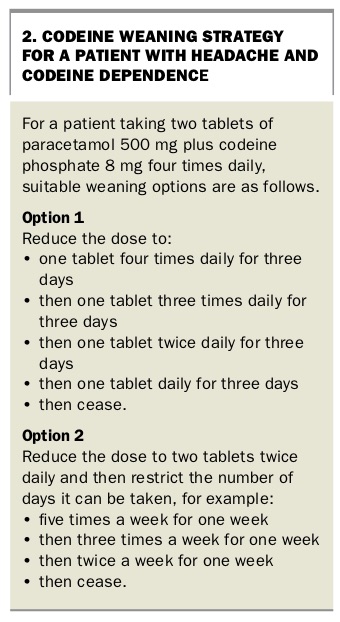
It is generally best to give patients a written plan that weans them gradually off their opioid over seven to 10 days (depending on the daily morphine equivalent). Suitable plans for a patient taking two tablets of paracetamol 500mg plus codeine phosphate 8 mg four times daily are shown in Box 2.
{kind=link}
Some patients are unable to tolerate gradual weaning of their opioid, in which case a more abrupt cessation strategy may be helpful. There are some data to suggest this approach may be more effective long term. There may be dual issues of managing withdrawal headache (NSAIDs, metoclopramide) and managing opioid withdrawal symptoms (consider clonidine). Patients on higher doses of codeine may require inpatient management.
Bridging therapy
If the patient finds (or is likely to find) it difficult to wean off codeine then a bridging strategy can help. Options for bridging therapy include:3
- naproxen 750 to 1000 mg sustained release daily for two to three weeks
- prednisolone for two weeks, at an initial dose of 1mg/kg (maximum 60mg) for three days, then 50mg for three days, then 37.5mg for three days, then 25mg for three days, then 12.5mg for three days, then cease
- unilateral or bilateral greater occipital nerve block.
If outpatient strategies fail then referral for inpatient management of abrupt withdrawal with a lignocaine or ketamine infusion might be appropriate. It might also be appropriate for a psychologist to help with cognitions around pain and acute analgesic use.
Bridging medications should be discontinued after the withdrawal period is successfully navigated. Prophylaxis for gastric ulcers and monitoring of blood sugar level must also be considered.
Prescribe an appropriate acute medication
In patients with migraine or cluster headache, it is worthwhile prescribing an effective triptan for acute treatment. Five triptans are available on the PBS to treat migraine (sumatriptan, zolmitriptan, naratriptan, rizatriptan and eletriptan), and patients may benefit from trying at least two or three to identify the one that is most effective for them.
Prescribe an appropriate preventive medication
At the same time as reducing codeine, it is important to start a preventive medication, if appropriate.5 A preventive should be considered in any patient experiencing more than three to four days of headache per month.
Selecting an appropriate preventive medication depends on diagnosing the underlying headache phenotype. A headache history should be taken, going back to when the headaches first started, as phenotypic features are often clouded by medication overuse. This may mean going back to the patient’s adolescence or even childhood. More detailed information on headache diagnosis and how to select a preventive medication is available in Therapeutic Guidelines: Neurology.7
Primary headache types and specific management
Key features of common primary headache types and suitable preventive medications and acute treatments include the following.
Migraine
The characteristics of migraine include:
- moderate-to-severe headache lasting four to 72 hours with associated nausea and vomiting, photophobia, phonophobia, osmophobia and motion sensitivity
- can be bilateral or unilateral and can alternate sides
- often described as pulsing or pounding
- affects the ability to undertake normal daily activities
- preceding aura lasting 15 to 30 minutes; this may be visual (most common), other sensory or motor (least common)
- often a family history
- may have known triggers, such as alcohol, foods (e.g. chocolate, strong cheese, monosodium glutamate (MSG), citrus, preserved meats), dehydration, sleep deprivation or excess, hot or stormy weather, menstrual periods, stress or relaxation from stress
- perimenstrual headaches, travel sickness and hangovers after minimal provocation are often clues to a migraine diagnosis.
Preventive medications for migraine
Options to consider for preventing migraine include:
- amitriptyline (start with 10 mg and build up to 50 mg at night; off-label use)
- propranolol (start with 10 to 20mg and build up to 40 to 80mg twice daily)
- topiramate (start with 12.5mg and build up to 50 to 100 mg twice daily)
- pizotifen (start with 0.5mg and build up to 1.5 mg at night)
- verapamil, sustained release (start with 90 mg and build up to 240 mg daily; off-label use)
- candesartan (start with 4 to 8 mg and build up to 24 to 32 mg daily; off-label use).
Many more migraine preventive medications are available. For patients who fail to respond or tolerate a reasonable dose in eight to 12 weeks, consider changing to another agent or referral to a neurologist for further advice.
If oral preventive medication fails then therapies such as botulinum toxin type A and erenumab might be considered under the guidance of a neurologist or pain medicine physician. These medications have specific clinical criteria and are not suitable for all patients.
Acute treatment of migraine
Acute treatment options for migraine include:
- soluble aspirin 900 to 1000 mg or ibuprofen 400 to 600mg on a maximum of 15 days per month
- a triptan, to be used on no more than 10 days per month
- the addition of metoclopramide or prochlorperazine to acute treatments, which can have additional benefit beyond simply treating nausea
- combination therapy with aspirin plus a triptan plus metoclopramide.
Medication to treat migraine is most effective if taken early in the attack.
Tension-type headache
The characteristics of tension-type headache include:
- mild to moderate headache, lacking associated features
- lasts 30 minutes to seven days
- often described as pressure, tightness or ‘band-like’
- often does not impair the ability to undertake normal daily activities.
Preventive medications for tension-type headache
Preventive medications to consider for frequent tension-type headache include:
- amitriptyline (start with 10mg, build up to 50mg at night; off-label use)
- mirtazapine (start with 15mg, increase to 30mg as tolerated; off-label use)
- venlafaxine, modified release (start with 75mg and increase to 150mg as tolerated; off-label use).
Acute treatment of tension-type headache
Acute treatment options for tension-type headache include:
- soluble aspirin 600 to 900mg
- ibuprofen 400mg
- naproxen 500 to 750mg
- paracetamol 1g.
Each of these should be used for a maximum of 15 days per month.
Trigeminal autonomic cephalgia
Trigeminal autonomic cephalgia includes cluster headache, hemicrania continua and paroxysmal hemicranias. These are a group of rare headache disorders that, if suspected, should prompt patient referral to a neurologist for diagnosis and management. All are characterised by:
- a strictly one-sided headache
- with associated (typically ipsilateral) autonomic features, such as tearing, conjunctival injection, ptosis, rhinorrhoea, tinnitus, unilateral facial flushing or sweating.
Cluster headache is one of the most severe pains described, and the patient should be referred urgently so that optimal management can be initiated. If the patient experiences frequent episodes then consider starting verapamil 40 to 80mg three times daily while awaiting specialist review. Acute attacks may respond to subcutaneous sumatriptan, a rizatriptan wafer or intranasal sumatriptan. High-flow oxygen (100% at 12 to 15L/min by non-rebreather mask) can also abort an acute attack.
Conclusion
The strategy to manage a patient with headache and codeine dependence is to diagnose the primary headache disorder and direct appropriate treatment towards this, including preventive medications where appropriate. Medication overuse should be addressed concurrently. Codeine should be weaned over seven to 10 days, with bridging therapy if needed. Lifestyle advice is integral to management in this group of patients. MT