A 49-year-old woman with seborrhoeic dermatitis

Skin conditions
A middle-aged woman with mild but recurrent seborrhoea on her face seeks treatment. Seborrhoeic dermatitis tends to be chronic and episodic and there is no long-term cure. What is the most appropriate management of this patient?
Case scenario
Janet is a 49-year-old woman with recurrent flaky patches and red skin around her nasal folds and mouth, as well as her eyebrows and hairline. She is perimenopausal and has no medical conditions and takes no medications.
Commentary
The characteristics of Janet’s skin problem are consistent with seborrhoeic dermatitis. This is a chronic, relapsing condition affecting areas of skin with a high density of sebaceous glands (face, scalp, central chest and genital areas). Adult-onset seborrhoeic dermatitis is a common condition affecting the middle-aged and elderly populations. A recent comparative cross-sectional study found the point prevalence of seborrhoeic dermatitis to be 14.3%, and cited previous estimates of between 2 and 23% in selected populations.1
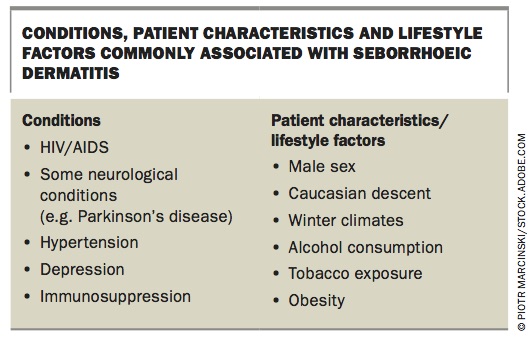
Seborrhoeic dermatitis is commonly associated with other medical conditions and certain patient characteristics and lifestyle factors (Box). The condition is more common in men than in women and is usually diagnosed after the age of 20 years.
{kind=link}
Pathogenesis
Seborrhoeic dermatitis has long been considered a result of the Malassezia spp. of lipophilic yeasts causing inflammation. However, it is not clear why this yeast, which is present on normal healthy skin, may cause inflammation in some people and not others.
Although the use of antifungal medications correlates with reduced inflammation it does not always correlate with reductions in the amount of malassezia yeasts (M. globossa and M. restricta) on the skin.2 A recent proposed model of seborrhoeic dermatitis links a change in the balance of the skin microbiome to an associated interplay between the immune system and skin barrier function.2
Clinical presentation and diagnosis
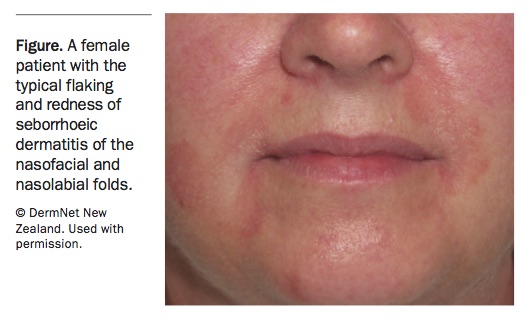
Common characteristics of seborrhoeic dermatitis include erythematous flaking and scaling macules on sebaceous skin. On the face, it commonly affects the folds including those behind the ears, the conchal bowls, the glabella and the nasolabial folds (Figure).
{kind=link}
Seborrhoeic dermatitis is also seen in hair-bearing skin of the scalp, chest, back, axilla and genital areas. In the scalp and beard the scale may be greasy and thick. The condition may be irritating, for example when blepharitis affects the eyelid margins; however, it is the appearance of the skin that is usually of most concern to patients.
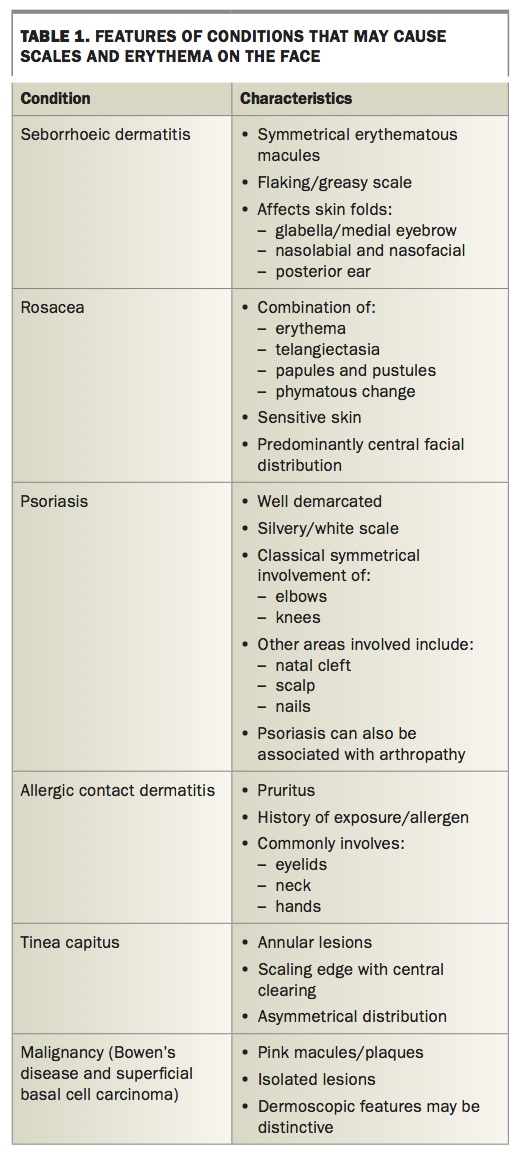
Differentiating seborrhoeic dermatitis from other scaling disorders and conditions involving erythema is important. Features of similar scaling and erythematous facial conditions are presented in Table 1. It is important to take a history and examine the patient for features of these conditions. In many cases there may be a combination of conditions, and treatment of one may worsen the other. For example, using topical corticosteroids on seborrhoeic dermatitis may worsen coexisting rosacea.
{kind=link}
The diagnosis of seborrhoeic dermatitis is a clinical diagnosis. A biopsy may show overlapping features of dermatitis and psoriasis. In severe cases that are unresponsive to treatment, HIV serological testing may be considered.
Treatment
Seborrhoeic dermatitis tends to be chronic and episodic and there is no long-term cure; however, the signs and symptoms can be managed. General advice about managing modifiable lifestyle risk factors should be given, such as reducing alcohol consumption.
Topical therapy
A basic skin-care regimen to help maintain skin barrier function is recommended. This would include a nonsoap wash and gentle emollient. A keratolytic (e.g. salicylic acid) may be added to reduce scale.
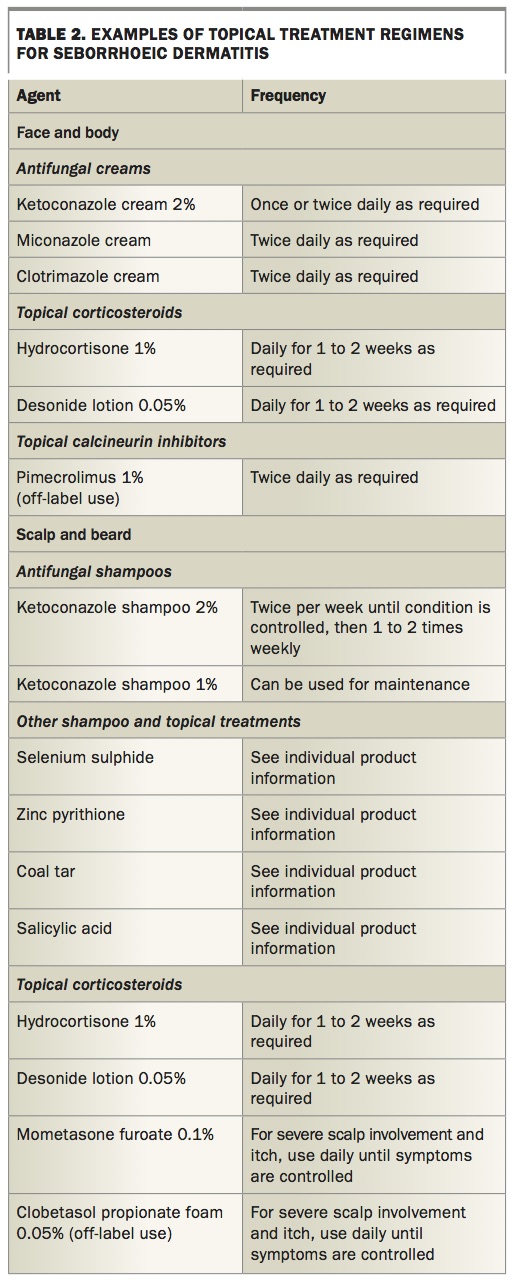
A Cochrane review and recent systematic review of topical therapy found that topical corticosteroids, topical azole antifungal agents and calcineurin inhibitors are effective treatments for seborrhoeic dermatitis.3,4 Table 2 shows examples of some topical treatment regimens.
{kind=link}
Systemic therapy
Oral fluconazole (off-label use), itraconazole and terbinafine (off-label use) have been used to treat moderate-to-severe seborrhoeic dermatitis.5 A recent retrospective review of 46 patients who were treated with low-dose isotretinoin (off-label use) after conventional treatments had failed showed impressive responses to treatment. Clearance of the condition or an excellent response were reported in 41 (89%) of the treated patients.6
Conclusion
Janet’s reported symptoms appear mild. Once other conditions are excluded by history and examination she should be counselled about the chronic nature of seborrhoeic dermatitis.
After lifestyle factors have been discussed, basic skin care advice should be given, starting with recommending a gentle nonsoap cleanser and emollients. If treating Janet, I would expect her to respond to ketoconazole 2% shampoo used twice weekly as required. I advise patients to use the shampoo as a face and body wash by lathering and leaving it on for a few minutes in the shower.
Additionally, the patient may use topical creams including ketoconazole cream or another azole cream, with or without a mild topical corticosteroid (e.g. hydrocortisone). The corticosteroid cream should be applied twice daily for one to two weeks when there is a flare-up not responding to the shampoo.
If the patient fails to respond to these measures, consider whether there might be an underlying systemic illness predisposing them to seborrhoeic dermatitis, such as HIV, neurological illness or a systemic illness. Treatment with systemic antifungals or isotretinoin may also be considered in moderate-to-severe disease when topical therapies fail; however, these require monitoring for safety in most cases. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.