ACL injuries in children: prevention and management

Sports injuries
The incidence of anterior cruciate ligament rupture – once considered a rarity in the paediatric population – is rising at an alarming rate.
In Australia, there has been an annual growth rate in anterior cruciate ligament (ACL) rupture of 8.8% in girls and 7.7% in boys between 5 and 14 years of age, and an overall increase of more than 70% across males and females between 5 to 24 years of age in the past 15 years.1 Rupture of the ACL is a serious and debilitating injury because it lacks the ability to heal and return to normal function, inevitably increasing the subsequent risk of further knee injury and degenerative lesions. About 70% of ACL tears occur through noncontact mechanisms such as pivoting, stepping and landing from a jumping position.2
Although the exact reasons remain uncertain, the rise of ACL injuries in children and adolescents has been attributed to an increase in average body mass index, an increase in competitive activity at a younger age, increased training load, single sports specialisation with an emphasis on year-round participation and a lack of time for free play.3 These increased rates have occurred on a background of improved rates of diagnosis due to better imaging and diagnostic tools.4
The consequences of an ACL injury are serious. In the short term, an ACL rupture often results in loss of an entire athletic season, surgical reconstruction and extensive physiotherapy that can last up to 12 months. Although a high proportion of paediatric patients return to competitive-level sports at pre-injury level (81%), there is a risk of a second ACL injury either due to graft rupture or injury to the contralateral ACL with rates reported as high as 13% and 14%, respectively.5
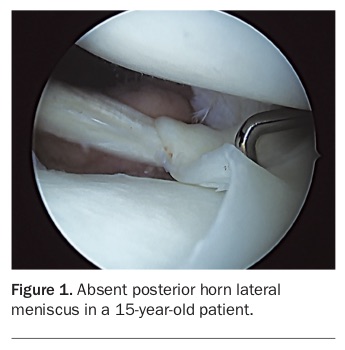
Almost all individuals who rupture their ACL are at increased risk of early onset of osteoarthritis with resultant disability, regardless of whether an ACL reconstruction is performed or not.6 Concerningly, this risk is substantially increased in those that also sustain a concurrent meniscal injury (Figure 1).1 This is of clinical importance for children, with recent reports of osteoarthritis developing as early as 10 years after injury, suggesting that a 10-year-old child who sustains an ACL injury can develop symptomatic knee osteoarthritis by 20 years of age and be at much greater risk of needing to undergo a knee replacement by 40 years of age.7,8 Asymptomatic osteoarthritis precursor chondral lesions post-ACL rupture and meniscal loss have also been noted in athletes as young as 15 years of age.
{kind=link}
Over the past 20 years, multiple randomised controlled trials have revealed that injury-prevention programs involving neuromuscular-type training reduce the risk of primary ACL injuries, as well as lower the risk of new ACL injuries among adult athletes who return to sport after ACL reconstruction. More recently, evidence suggests that these programs may also benefit skeletally immature patients.8 Primary musculoskeletal healthcare providers involved in the management of paediatric athletes are well placed to actively advocate injury-prevention programs.
Diagnosis of an ACL injury
Providing an accurate and timely diagnosis is the starting point for effective management planning. If a ‘wait-and-see’ approach is adopted, and the patient returns to sport without a correct diagnosis, there is a high risk of sustaining a devastating subsequent meniscal injury.
GPs should begin an examination on a child with a suspected ACL injury with a thorough history followed by physical examination. The patient will often report hearing an audible ‘pop’ in the knee during a landing or stepping event, pain with weight-bearing and a feeling of ‘giving way’. Within 24 hours of injury a large haemarthrosis may develop. However, haemarthrosis is not pathognomonic as studies have shown that ACL injuries are present in about 65% of adolescents with acute traumatic haemarthrosis.9
The three most commonly used physical examination tests to assess an ACL injury are:
- the Lachman’s test
- the anterior drawer test
- the pivot shift test.
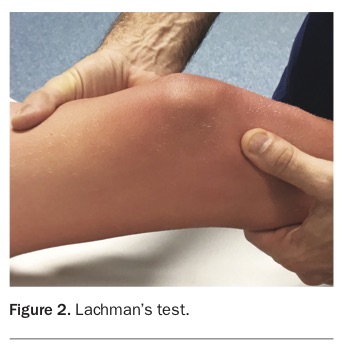
The Lachman’s test is the most accurate of the three, with a sensitivity of 68% for partial ruptures and 96% for complete ACL ruptures reported.10 The Lachman’s test is performed with the patient supine with the knee in about 15 to 20° of flexion (Figure 2). The examiner slowly translates the tibia anteriorly on the femur, feeling for the quantity of translation and quality of the endpoint relative to the contralateral side. Increased translation with a soft endpoint suggests the ACL is torn; however, young patients are more physiologically lax, hence the importance of examining the other side for comparison.
{kind=link}
Physical examination of a painful swollen knee to confirm an ACL injury can be challenging, even for specialists. MRI is reported to be highly sensitive and specific for detecting ACL ruptures in children with values reported to be 95% and 88%, respectively.11 GPs should therefore recommend that all knee injuries in young athletes from an acute traumatic event that resulted in the athlete leaving the field of play undergo an MRI unless the diagnosis can be made with absolute certainty without MRI. There is no reason to delay the MRI, even if significant swelling is present. The role of mandatory plain radiographs remains uncertain. However, they can be helpful to exclude fracture, osteochondral injury or physeal injury that can occur with or without ACL rupture.12
Management options
Once the diagnosis of an ACL rupture is confirmed, a shared decision-making process regarding best management practice can be initiated between the child, the parents/guardian and the clinician. Management goals are to restore a stable and pain-free joint that is functional, while also reducing the risk of subsequent meniscal tear-induced osteoarthritis and minimising the risk of a surgically induced physeal injury.7
To help achieve these goals, a child with an ACL rupture should undergo high-quality rehabilitation, irrespective of whether a reconstruction is planned or not. Rehabilitation should primarily focus on dynamic multi-joint neuromuscular control. If the child is less than 12 years of age and/or has markedly open physis, there should be less emphasis on the development of muscular strength and hypertrophy until the onset of puberty and maturation.8
Postoperative rehabilitation should last at least nine months, however, with the high risk of a second ACL injury following surgery the patient should be advised not to return to sports until at least 12 months after reconstruction, especially if they participate in a pivoting-type sport. Once the child returns to sport, continued strength and neuromuscular training is crucial to reduce the risk of further ACL injury to the ipsilateral or contralateral side.
In the paediatric population, there are three indications for ACL reconstruction:
- the injured child has symptomatic or recurrent knee instability
- the injured child has a repairable meniscal tear or osteochondral defect, which requires ACL reconstruction at the same time to achieve a stable joint
- future participation restrictions placed on the injured child are unacceptable.
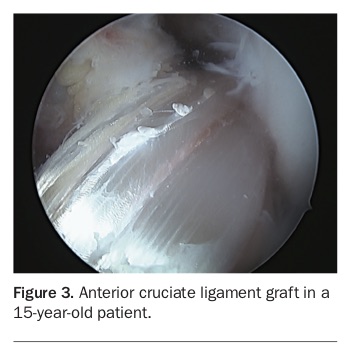
Controversy exists as to who should be offered an ACL reconstruction (Figure 3) and when, with hazards for both operative and nonoperative methodologies. Patients treated nonoperatively have a high risk of subsequent meniscal tears, irrespective of their symptoms of instability, whereas patients with open physis have a small but concerning risk of growth arrest. Population level data with long-term follow up has also suggested a lower risk of osteo-arthritis in patients who undergo reconstruction compared with those who do not.13 Although the optimum method remains uncertain in this cohort, three surgical techniques (transphyseal, partial transphyseal and physeal sparing) exist to reduce the risk of physeal damage and growth disturbance in the child athlete. The type of graft choice is also complicated with no perfect option. However, if there is an open physis the patella tendon graft should not be used.
{kind=link}
Protective knee bracing is recommended in the skeletally immature child during the prehabilitation phase as well as for two to six weeks after ACL reconstruction, depending on concomitant surgical procedures. It is also recommended that the child wear a protective brace during strenuous activities if being treated nonsurgically. However, the effectiveness of bracing following ACL injuries or reconstruction in paediatric patients remains uncertain.8
Preventing ACL injuries
Noncontact ACL injuries are largely preventable by athletes participating in an integrated strengthening and neuro-muscular training program as part of their warm-up routine.14 Many sports already have these programs in place, and while each of these programs are sport specific, they all include components of strength, agility, co-ordination and balance, as well as safe-stepping and controlled landing exercises where emphasis is made on landing on a flexed knee. Stepping manoeuvres while balanced using a wider stance are also practised in order to markedly reduce the loads placed on the ACL during directional changes. Two of these programs have been tailored to younger athletes, FIFA 11+ Kids (soccer) and Netball Australia’s KNEE Program (Box). Both programs, which are available online at no cost, aim to prevent and reduce the number and severity of injuries by improving the child’s physical competence and sport-specific movement skills. For maximum effectiveness, all preventive programs (regardless of sport) should be completed at least twice a week throughout the season.
{kind=link}
To reduce the ACL epidemic in young Australians, prevention programs that emphasise strength, agility and teaching the correct technique should be a priority. GPs and other musculoskeletal healthcare providers are uniquely positioned to raise awareness about the importance of ACL injury-prevention programs to young athletes and their parents, schools and sporting clubs. Medical and associated allied health groups, such as the Australian Orthopaedic Association, AFL Doctors Association, Arthritis Australia, Sports Medicine Australia and the Australian Physiotherapy Association, are currently advocating the funding of a national sports injury-preventive program. It has been calculated that such a program, targeted at 12- to 25-year-olds playing high-risk sports, could prevent one ACL rupture for every 27 athletes trained, at a national cost saving in excess of $300 million.6
Conclusion
Rupture of the ACL is a serious and debilitating injury because it lacks the ability to heal and return to normal function, inevitably increasing the subsequent risk of further knee injury and degenerative lesions; and because almost all individuals who rupture their ACL are at increased risk of early onset of osteoarthritis with resultant disability. Prevention programs that emphasise strength, agility and teaching correct technique can prevent the incidence of ACL injuries in the paediatric population. GPs are well placed to raise awareness about the importance of ACL injury-prevention programs in their communities. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.